
Abstract
Background:
Polycystic ovary syndrome (PCOS) is a common endocrine pathology affecting women of reproductive age characterized by chronic anovulation, hyperandrogenism, and polycystic ovaries. Coronary artery calcification (CAC) is a marker of subclinical atherosclerosis and prognostic of cardiovascular disease (CVD) risk. Some studies have shown that women with PCOS have a greater risk of CAC; however, a few others report contrary findings. The objective of this study is to examine and quantify the association between PCOS and CAC.
Materials and Methods:
We searched EMBASE, Google Scholar, PubMed, and Web of Science from inception to November 2021 to identify studies that provided information on PCOS and CAC. We used a random-effects model to aggregate the odds ratios (ORs) for CAC (score >0) among women with PCOS compared with controls adjusted for sociodemographic characteristics and CVD risk factors.
Results:
From the 36 articles reviewed, 3 prospective cohort and 4 cross-sectional studies met the inclusion criteria with a total of 2341 participants. Six studies used CAC > 0 as an outcome and were included in the pooled analysis. Using the Hartung–Knapp–Sidik–Jonkman method, the pooled adjusted ORs for the associations between PCOS and the presence of CAC were 2.48 (95% confidence interval: 2.11–2.84) with no significant heterogeneity (I 2 = 0.10%, p = 0.97) for the cohort studies and 1.88 (0.71–3.06) with no significant heterogeneity (I 2 = 13.95%, p = 0.87) for the cross-sectional studies.
Conclusion:
In pooled analyses, women with PCOS had approximately twofold greater odds of having CAC compared with women without PCOS. However, additional prospective studies will be needed to further understand the relationship between PCOS and CAC.
Introduction
Polycystic ovary syndrome (PCOS) is one of the most common endocrine pathologies found in women of reproductive age characterized by chronic anovulation, hyperandrogenism, and polycystic ovaries. 1 –3 The prevalence of PCOS in the general population is between 5% and 13% based on criteria from Rotterdam, National Institutes of Health (NIH), as well as the Androgen Excess and PCOS Society. 4 Although the etiology is largely unknown, insulin resistance plays a central role in the pathogenesis of PCOS. 2,5 –7
Insulin resistance, along with high prevalence of obesity in women with PCOS, increases the risk for dyslipidemia, type 2 diabetes, hypertension, and cardiovascular disease (CVD). 2,8 –11 Several observational studies have shown up to a twofold increase in the risk for coronary heart disease and stroke among women with PCOS 12 –17 ; however, a few other studies provide conflicting results. 18 –20 Genetic studies have questioned the direct causal role of PCOS in CVD, 21 suggesting the relationship may be mediated through shared cardiometabolic risk factors. 19
To reduce the burden of CVD among women with PCOS, early detection of clinical CVD can be facilitated by the measurement of surrogate markers of subclinical atherosclerosis such as coronary artery calcification (CAC). CAC has emerged as a superior prognostic marker of CVD risk compared with traditional risk factors and other biomarkers, improving CVD risk classification including upgrading risk when CAC is present (i.e., CAC > 0) and downgrading risk when CAC is absent (i.e., CAC = 0). 22,23 Therefore, CAC has been incorporated into recent United States primary prevention guidelines to help guide shared decision making regarding the initiation of statin therapy in cases where risk is otherwise uncertain. 24
Women with PCOS may have a greater risk of CAC due to the clustering of cardiovascular and metabolic aberrations. 25 –31 However, epidemiological studies vary in their findings of an association between PCOS and CAC. 25 –31 The aim of this systematic review and meta-analysis is to examine and quantify the risk of CAC, an outcome that is strongly predictive of CVD events, among women with PCOS compared with women without PCOS. We hypothesized that women with PCOS will have a greater risk of CAC due to the cardiometabolic dysfunction associated with PCOS.
Materials and Methods
Data sources and search strategy
An independent search of EMBASE, Google Scholar, PubMed, and Web of Science was conducted from inception to November 2021 to identify studies with information on PCOS and CAC. We reported the findings of this review using the guidelines from the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) (Supplementary Appendix). 32 The search strategy combined MeSH terms and keywords and had no language restriction.
We used MeSH terms or keywords such as polycystic ovary syndrome, polycystic ovarian syndrome, syndrome polycystic ovary, coronary artery calcium, and coronary artery calcification (Supplementary Table S1). In addition to the database search, the reference lists of articles were screened. Two authors (O.Os. and O.Og.) independently reviewed and selected studies with information on PCOS and CAC. Disagreements were resolved by consensus. Institutional review board approval was not required for this study because it is a systematic review and meta-analysis.
Study selection
The inclusion criteria for the studies in this systematic review and meta-analysis are as follows: (1) studies with information on PCOS and CAC, (2) studies conducted among human populations, and (3) peer-reviewed studies. Studies without the exposure or outcome of interest and review articles were excluded. We retrieved, reviewed, and extracted data from the full texts of studies that satisfied the selection criteria (Table 1).
Descriptive Characteristics of Studies
Controls indicate women without PCOS.
BMI, body mass index, IQR, interquartile range; PCOS, polycystic ovary syndrome, SD, standard deviation.
Quality assessment
The methodological quality of the studies that met the selection criteria was assessed using the Newcastle-Ottawa Scale (NOS) for the case–control and cohort studies 33 or a modified version of the NOS for the cross-sectional studies. 34 The NOS was developed by a collaboration between the University of Newcastle, Australia, and University of Ottawa, Canada, to evaluate the quality of nonrandomized studies.
The quality of each study is rated based on three broad areas: (1) selection of study groups, (2) comparability of the groups, and (3) ascertainment of either the exposure or outcome of interest. For the NOS, a maximum of 9 stars can be awarded to a study where ≤3, 4 to 6, and 7 to 9 stars are rated as weak, moderate, and strong, respectively. 33 The modified NOS awards a study a maximum of 7 stars where ≤3, 4 to 6, and 7 stars are rated as poor, fair, and good, respectively. 34 The quality assessment for this review was independently conducted by two authors (O.Os. and O.Og.) (Supplementary Figures S1 and S2).
Statistical analysis
We used STATA 16.0 (StataCorp, College Station, TX) to perform the meta-analysis for this study. Considering the small number of studies included in this meta-analysis, we used the Hartung–Knapp–Sidik–Jonkman method that generates robust variance estimation for random effects. 35,36 We included studies in the pooled meta-analysis that reported the association of PCOS with the outcome of CAC presence (score >0).
We conducted two separate pooled analyses for the three prospective cohort studies and three cross-sectional studies that met the inclusion criteria for the meta-analyses. In addition, we conducted a combined pooled analysis of six studies that included the three prospective cohort studies and three cross-sectional studies. All the studies in the meta-analyses reported adjusted odds ratios (ORs) with 95% confidence intervals (CIs) as measures of effect. We inputted into STATA the ORs and created forest plots with a random-effects model to produce summary estimates of the pooled ORs. The heterogeneity between studies was measured using I2 statistics and was considered substantial if >50%.
Results
Literature search
As shown in Figure 1, 43 articles were identified using the search strategy previously described and 7 duplicate articles were excluded after screening the titles and abstracts. We assessed the full texts of the remaining 36 articles for eligibility and excluded 29 articles that did not meet the inclusion criteria. Seven articles were included in the systematic review and six were included in the meta-analysis. The study excluded from the pooled meta-analysis defined the CAC outcome differently from the other studies. 29

PRISMA flow diagram of literature search strategy. PRISMA, preferred reporting items for systematic reviews and meta-analyses.
Study characteristics
The descriptive characteristics of the studies that met the inclusion criteria of this review are presented in Tables 1 and 2. A total of 2341 individuals participated in this systematic review, whereas 2027 were included in the meta-analysis (1443 from the prospective cohort studies and 584 from the cross-sectional studies). Five studies reported a mean age between 32 and 49.4 years, whereas two studies reported a median age between 38.5 and 42 years. The study design of three studies was prospective cohort 25 –27 and four studies were cross-sectional. 28 –31 All the studies were conducted in the United States. PCOS was diagnosed differently across studies but generally included clinical features of hyperandrogenism, chronic anovulation, and luteinizing hormone–follicle-stimulating hormone ratio >2.0.
Descriptive Characteristics of Studies Continued
Controls indicate women without PCOS. CAC was measured in Agatston units. aOR was hand calculated for Talbott et al. and Chang et al. Shroff et al. Chang et al. and Calderon-Margalit et al. did not report mean CAC scores.
CAC, coronary artery calcification; CT, computed tomography; EBCT, electron beam computed tomography; EBT, electron beam tomography; FSH, follicle-stimulating hormone; HOMA-IR, homeostasis model assessment-insulin resistance; LH, luteinizing hormone; NIH, National Institutes of Health; OR, odds ratio; SBP, systolic blood pressure; TG, triglycerides.
Two of the included studies specified the NIH or Rotterdam criteria for the diagnosis of PCOS. Coronary artery calcification was measured by electron beam computed tomography (CT) or electrocardiogram-gated noncontrast cardiac CT. Six studies measured CAC > 0 25 –28,30,31 whereas one study measured CAC ≥ 10. 29 Using the NOS, prospective cohort studies were awarded seven stars that is considered strong quality (Supplementary Fig. S1), whereas the cross-sectional studies were awarded six stars using the modified NOS indicating fair quality (Supplementary Fig. S2).
Association between PCOS and CAC
Three prospective cohort studies examined the association between PCOS and CAC. 25 –27 One study found that women with PCOS were more than twice as likely as controls (women without PCOS) to have CAC > 0 (OR = 2.31 [95% CI: 1.00–5.33] p = 0.049), after adjusting for age and body mass index (BMI). 25 A second study found that women with PCOS were more than twice as likely as controls to have CAC > 0 (OR = 2.46 [1.56–3.88]). The women with PCOS were matched by age and race to controls.
The women with PCOS were matched by age and race to controls. 26 The third study found that women with PCOS were almost three times as likely as controls to have CAC > 0 (2.70 [1.31–5.60]) after adjusting for age, race, education, smoking, menopausal status, BMI, systolic blood pressure, triglycerides, and homeostasis model assessment-insulin resistance (HOMA-IR). 27 In our meta-analysis of the three prospective cohort studies, the pooled OR was 2.48 (2.11–2.84) with no significant heterogeneity (I 2 = 0.10%, p = 0.97) (Fig. 2).
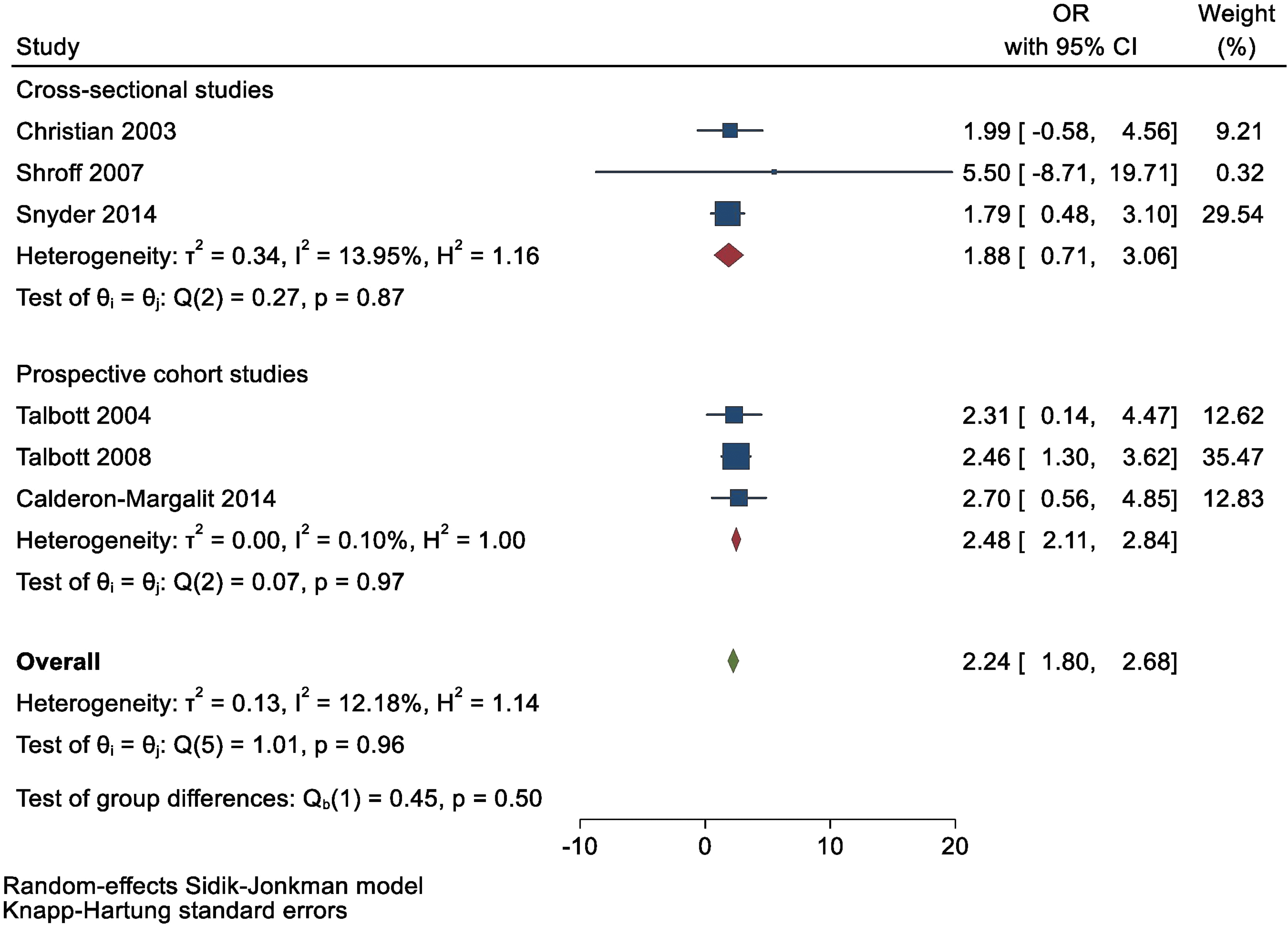
Forest plot showing pooled adjusted ORs with 95% CIs of the association between PCOS and coronary artery calcification (CAC > 0). CAC, coronary artery calcification; CI, confidence interval; OR, odds ratio; PCOS, polycystic ovary syndrome.
Four cross-sectional studies examined the association between PCOS and CAC. 28 –30 One study found that women with PCOS were twice as likely as controls to have CAC > 0 (OR = 1.99 [0.68–5.82]) after adjusting BMI. 28 The second study found that the prevalence of CAC was low in both women with PCOS and controls (5.4% and 6.3%, respectively, p = 0.74), and women with PCOS were less likely than controls to have CAC ≥ 10 (OR = 0.78 [0.29–2.08]). The women with PCOS were matched by age and BMI to controls. 29 The third study found that women with PCOS were almost twice as likely as controls to have CAC > 0 (OR = 1.79 [0.91–3.53]), after adjusting for age, C3 complement, BMI, insulin, and African American race. 30
The fourth study found that women with PCOS (matched by age and BMI to controls) were more than five times as likely as controls to have CAC > 0 (OR = 5.5 [1.03–29.45]). 31 In the meta-analysis of the three cross-sectional studies by Christian et al., 28 Shroff et al., 31 and Snyder et al., 30 the pooled OR was 1.88 (0.71–3.06) with no significant heterogeneity (I 2 = 13.95%, p = 0.87) (Fig. 2). In a combined meta-analysis of six studies that included the three prospective cohort studies and three cross-sectional studies, the pooled OR was 2.24 (1.80–2.68) with no significant heterogeneity (I 2 = 12.18%, p = 0.96) (Fig. 2).
Discussion
Summary of findings
In this systematic review and meta-analysis of 2341 participants from 7 studies, we found in the meta-analysis of 3 prospective cohort studies that women with PCOS had ∼2.5-fold risk of having CAC > 0, even after adjustment for BMI and cardiometabolic risk factors, compared with women without PCOS. However, in the meta-analysis of three cross-sectional studies, the risk of having CAC > 0 was almost twofold greater, but this finding was not statistically significant. In the combined meta-analysis of six of the seven studies, women with PCOS were two times more likely to have CAC > 0 compared with women without PCOS.
Of note, there was no substantial heterogeneity between studies. The study excluded from the meta-analysis observed that the prevalence of CAC ≥ 10 was low for both women with PCOS and controls. Additionally, women with PCOS were less likely to have CAC ≥ 10 compared with controls with no statistically significant difference. 29 These findings have important implications regarding the assessment of CVD risk in women with PCOS.
Explanation of findings
A number of biological pathways have been postulated to explain the association between PCOS and CAC (Fig. 3: graphical abstract). Christian et al. 28 found that the greater prevalence and extent of CAC in women with PCOS compared with controls may be attributable to obesity and visceral adiposity, as well as higher levels of low-density lipoprotein cholesterol.
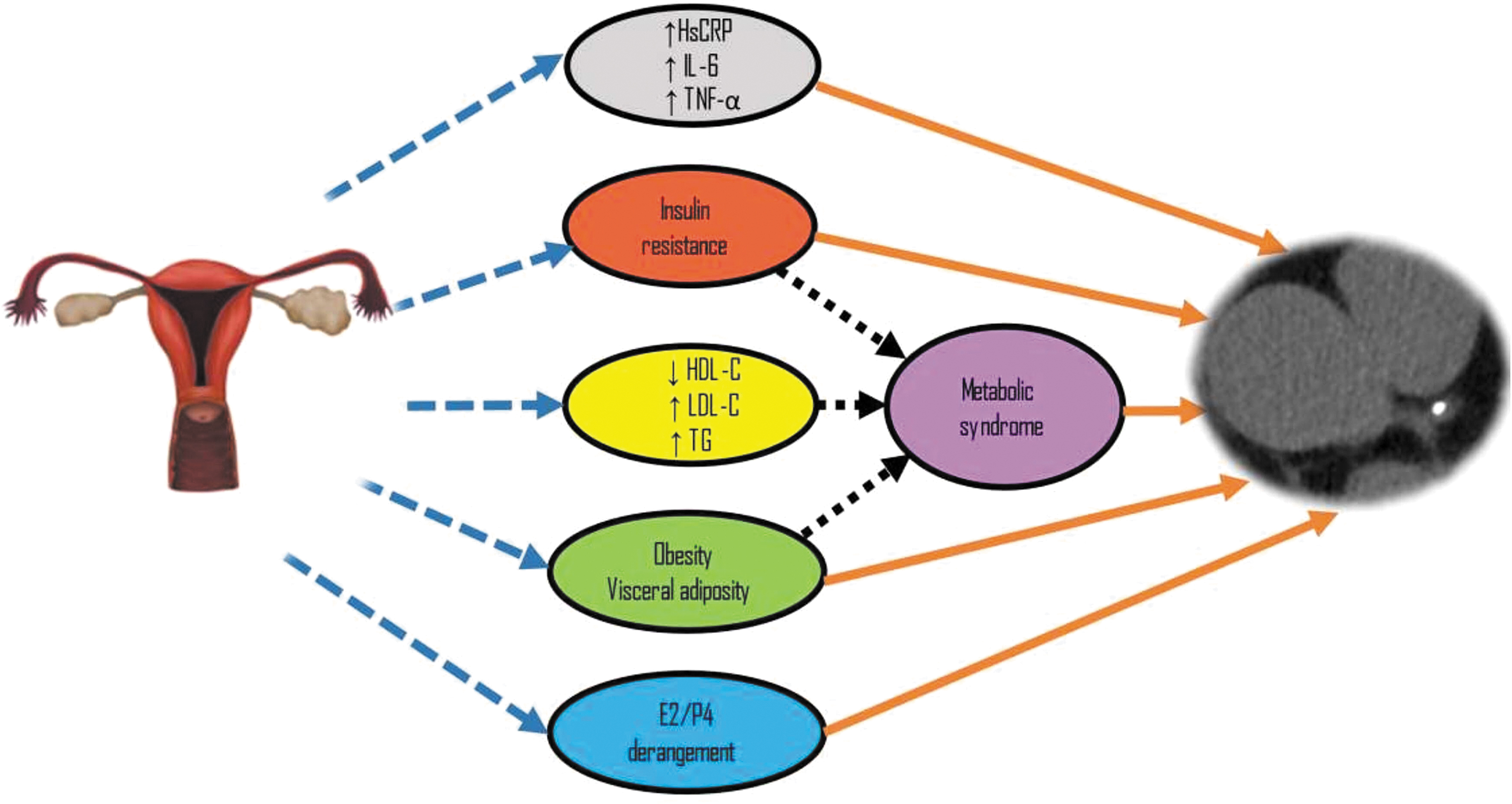
Graphical abstract illustrating the cardiometabolic pathway between PCOS and coronary artery calcification. *PCOS image used with permission from Shutterstock.
Talbott et al. 25 in their study on the association of metabolic syndrome with coronary and aortic calcification among women with PCOS found that the greater prevalence of CAC and the magnitude of CAC scores in women with PCOS compared with controls could be explained by the presence of obesity, metabolic syndrome, and insulin resistance. However, among the features of metabolic syndrome, only high-density lipoprotein cholesterol and triglycerides considerably mediated the effect of PCOS on CAC.
In a study conducted by Shroff et al., 31 early onset coronary atherosclerosis as measured by CAC was found in young obese women with PCOS. Although the authors did not have significant evidence to support their findings, they posited that women with PCOS may have an increased risk for CAC because of a higher prevalence of metabolic syndrome and higher levels of inflammatory markers such as high sensitivity C-reactive protein, interleukin-6, and tumor necrosis factor-alpha.
In another study conducted by Talbott et al. 26 that examined the effect of PCOS and menopause on subclinical atherosclerosis, the authors found that the early atherosclerotic changes and increased prevalence of CAC seen in women with PCOS compared with controls were likely due to an early onset exposure to an unfavorable cardiovascular profile, which includes central obesity and insulin resistance.
Furthermore, in a study by Snyder et al. 30 that investigated the association between C3 complement and CAC among women with PCOS and controls, the authors suggested that C3 complement may be a CVD risk marker among women with PCOS and the general population. However, the findings of the study imply that C3 complement is not the driver of the association between PCOS and CAC but may play a role in the inflammatory process given that C3 complement is part of the innate immune system. Calderon-Margalit et al. 27 found an increased risk of subclinical CVD assessed by CAC after a 20-year follow-up among women with PCOS compared with controls. This association was explained by the higher HOMA-IR, higher triglycerides, and higher prevalence of diabetes and metabolic syndrome found in women with PCOS.
In addition, the authors suggested that derangements in hormones of the PCOS milieu such as estrogen, progesterone, and the ratios of both hormones with androgens may contribute substantially to the development of subclinical CVD. In contrast to the findings of the aforementioned studies, Chang et al. 29 in their study on the relationship between PCOS and subclinical atherosclerosis did not find more detectable CAC among women with PCOS compared with controls. According to the authors, their findings give credence to the hypothesis that the association between PCOS and CVD is largely attributable to insulin resistance and obesity, and not as a result of hyperandrogenemia.
Public health implications
Subclinical atherosclerosis, such as the presence of CAC, is likely one of many mediating pathways through which PCOS increases clinical CVD risk. 10 Some studies have reported that there is no evidence to suggest a higher risk of CVD among women with PCOS after accounting for adiposity, 18,20 but other studies have reported contrary findings, 12,13,16 including a recent study that estimated a 19% higher risk for CVD among women with PCOS compared with women without PCOS. 14
This finding was mainly due to a higher prevalence of metabolic abnormalities from dyslipidemia, hypertension, insulin insistence, and obesity among women with PCOS. With the substantial CVD burden associated with PCOS noted in these latter studies, 14,16 early detection of subclinical atherosclerosis may be a useful strategy to reduce the incidence of CVD in these women by prompting initiation or intensification of lifestyle changes and preventive pharmacotherapy.
According to the guidelines, a diagnosis of PCOS should be followed by a comprehensive risk assessment for glucose intolerance, dyslipidemia and a family history of diabetes or hypertension, and familial hypercholesterolemia. 2,37 Moreover, population-based cohort studies have provided evidence that suggest the presence and progression of CAC predict the incidence of CVD events beyond traditional risk factors, even among otherwise low-risk women. 38 Testing for CAC can be employed in women with PCOS to identify those at risk of future CVD so that appropriate interventions such as statin therapy can be initiated. 39
However, the age to begin testing in these women is still under debate. CAC scores can be utilized to refine risk assessment in women with PCOS when CVD risk is ambiguous. For example, a CAC score >0 is indicative of subclinical atherosclerosis, and statin initiation may prove beneficial for CVD prevention. 24 Statin therapy can also improve the pattern of dyslipidemia and androgen excess in PCOS, 40 reducing the risk for atherosclerosis development and progression.
Metformin has been used in PCOS to improve weight and cardiometabolic profile. 41 The use of glucagon-like peptide receptor agonists (GLP-1RA) is also being evaluated for the treatment of obesity and insulin resistance in PCOS. 42 However, it has not yet been established whether GLP-1RA can reduce atherosclerotic CVD in women with PCOS. Most importantly, early lifestyle interventions (such as eating a healthy diet, regular physical exercise, and weight control) can be implemented in women with PCOS to decrease the initiation and progression of subclinical atherosclerosis. 2,37
Limitations
Our study has some limitations. First, we cannot make causal inferences from the association of PCOS with CAC because all the studies included in this systematic review and meta-analysis were observational studies. Second, the sample size for most of the studies was small so they may not have been adequately powered to accurately detect an association between PCOS and CAC. Also, in the pooled analysis, two studies accounted for ∼65% of the sample weight. 26,30 Third, the interpretation of our findings should take into consideration that there may have been some overlap in the selection of study participants from two studies with participants from the Pittsburgh PCOS cohort. 25,26
Fourth, the pooled estimates from the combined meta-analysis of six studies should be interpreted with caution because of the different study designs. Furthermore, the different diagnostic criteria for PCOS may have resulted in misclassification of PCOS; therefore, the pooled estimates from our meta-analysis may be biased. Fifth, it is worth noting that CAC scores have some limitations in the clinical management of patients. The presence of noncalcified atherosclerotic plaque cannot be ruled out by CAC scores. 43
In addition, the use of high CAC scores alone in asymptomatic patients may lead to unnecessary invasive tests.43 Sixth, we could not assess publication bias because of the small number of studies included in each meta-analysis. Additionally, our pooled estimates may have been attenuated if more studies with negative results were published. Lastly, we cannot rule out residual confounding in the reported estimates of the association between PCOS and CAC, although most of the studies that met our inclusion criteria adjusted for potential confounding factors.
Conclusion
In this systematic review and meta-analysis, women with PCOS had a greater burden of CAC compared with women without PCOS, which may be due to the cardiometabolic abnormalities associated with PCOS. However, well-designed large prospective cohort studies are needed to accurately measure the risk for CAC in women with PCOS using consistent diagnostic criteria for PCOS and clinically meaningful interpretation of CAC scores established for the management of patients. These new studies are required to corroborate the findings of this review so that evidence-based recommendations can be provided to prevent the onset and progression of subclinical atherosclerosis in women with PCOS.
Since PCOS has different phenotypes, future studies could explore the pathogenic implications of the heterogeneity of PCOS as a determinant of the risk of CAC. In addition, more research should be directed toward the development of novel interventions that target the biological pathways responsible for insulin resistance and metabolic syndrome in women with PCOS.
Footnotes
Authors' Contributions
O.Os. contributed to conceptualization, formal analysis, investigation, methodology, software, visualization, supervision, writing—original draft, and writing—review and editing. O.Og. was involved in conceptualization, formal analysis, investigation, methodology, software, visualization, supervision, writing—original draft, and writing—review and editing. O.B.K. carried out methodology, visualization, supervision, and writing—review and editing. A.G.H. carried out methodology, visualization, supervision, and writing—review and editing.
V.O. was involved in methodology, visualization, supervision, and writing—review and editing. A.M. carried out methodology, visualization, supervision, and writing—review and editing. M.G. was in charge of methodology, visualization, supervision, and writing—review and editing. E.D.M. carried out methodology, visualization, supervision, and writing—review and editing. All authors approved the final draft of the article for submission.
Author Disclosure Statement
E.D.M. has served on advisory boards for AstraZeneca, Amarin, Bayer, Boehringer Ingelheim, Esperion, Novartis, Novo Nordisk, and Pfizer. The other authors have no conflicts of interest to disclose.
Funding Information
E.D.M. is supported by the Amato Fund in Women's Cardiovascular Health at Johns Hopkins University. A.M. is supported by NHLBI Training Grant T32HL007024. The funding sources played no role in the study design; collection, analysis, and interpretation of data; in the writing of the report; and in the decision to submit the article for publication.
Supplementary Material
Supplementary Figure S1
Supplementary Figure S2
Supplementary Appendix
Supplementary Table S1
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.