
Abstract
Equitable access to high quality adolescent sexual and reproductive health (ASRH) services can help reduce unintended pregnancies, sexually transmitted diseases, and disparities in these outcomes. The Centers for Disease Control and Prevention (CDC), Division of Reproductive Health, has a long history of working to improve access to and quality of ASRH services through applied research and public health practice. This report from CDC summarizes the evolution of these efforts from more than a decade of work—from community-based demonstration projects to an initiative to support wide-scale implementation. We describe a community-wide teen pregnancy prevention program model that includes a component addressing ASRH services (2010–2015), focused efforts related to quality improvement (QI) of and community–clinic linkages to ASRH services (2015–2020), and the development of a QI package that collates implementation strategies and tools to improve ASRH services (2020–2022). We conclude by discussing future directions. In disseminating key strategies and resources from this work, we aim to support broader public health and clinical efforts to strengthen ASRH care in the United States in ways that promote health equity.
Introduction
The birth rate for females aged 15–19 years in the United States has declined 63% since 2007 and reached a record low of 15.4 births per 1000 in 2020. 1 Nevertheless, the United States continues to have among the highest teen birth rates of industrialized countries, and disparities persist by race/ethnicity, geography, and socioeconomic status. 2 –4 Moreover, rates of chlamydia and gonorrhea are highest among adolescents and young adults. 5 Equitable access to high quality adolescent sexual and reproductive health (ASRH) services (e.g., contraceptive counseling and provision; sexually transmitted disease [STD] counseling, screening, or treatment) can help reduce unintended pregnancies, STD/HIV infections, and disparities in these outcomes. 6 –9
In addition, supporting ASRH care can lay a foundation for health and well-being into adulthood. 10 Unmet health care needs during adolescence are associated with poor health outcomes in adulthood, 11 and consequences of adverse ASRH outcomes can be long term (e.g., infertility associated with untreated chlamydia/gonorrhea). 12 Adolescence is also a unique developmental period, during which health risks associated with early childhood trauma can be mitigated, 13 and lifelong protective behaviors, including health care seeking, can be established. 14
Despite the importance of ASRH care, many adolescents do not receive recommended services. For example, receipt of any contraceptive service (such as counseling about birth control) among 15–17-year-old females in the United States was 31% in 2015–2019. 15 National estimates from 2011 to 2013 indicate that only 38% of women 15–24 years who were sexually active in the past year had been tested for chlamydia in that year, despite recommendations for annual screening. 16,17 Issues with both access to and quality of care contribute to suboptimal receipt of services. Adolescents face numerous barriers to seeking health care, including sexual and reproductive health (SRH) services, such as limited awareness of the need for services, cost, lack of transportation, and confidentiality concerns. 18 –21 For adolescents who are able to access health care, missed opportunities for providers to deliver recommended SRH services (e.g., contraceptive counseling, STD screening) and implement youth-friendly practices (e.g., time alone with a provider to support confidentiality, low- or no-cost services, weekend/evening hours) have been documented and underscore a need to improve quality of care. 19,22 A recent national survey found that among adolescents who had a preventive visit in the past 2 years, only 20% of 11–14-year-old females and 44% of 15–17-year-old females had time alone with a provider at their last preventive visit. 22 In addition, fewer than one-third of adolescents reported discussions about SRH topics other than puberty at their most recent preventive visit. 22
The Centers for Disease Control and Prevention (CDC), Division of Reproductive Health, has a long history of working to improve access to and quality of ASRH services through applied research and public health practice. This report from CDC describes the evolution of these efforts from more than a decade of work—from community-based demonstration projects to an initiative to support wide-scale implementation. In disseminating key findings and resources from this work, we aim to support broader public health and clinical efforts to strengthen ASRH care in the United States in ways that promote health equity.
A Community-Wide Approach
From 2010 to 2015, CDC, in collaboration with the U.S. Department of Health and Human Services Offices of Adolescent Health and Population Affairs, funded nine state- and community-based organizations and five national organizations through a cooperative agreement, Teenage Pregnancy Prevention: Integrating Services, Programs, and Strategies through Community-Wide Initiatives (referred to as CWI). 23 The state- and community-based organizations implemented their initiatives in localities that experienced disproportionately high rates of teen birth. These initiatives addressed five components. Two were considered pillar components: improving access to and quality of ASRH services and implementing evidence-based teen pregnancy prevention programs. These pillar components were supported by the other three components which focused on building community support: Community Mobilization, Stakeholder Education, and Working with Diverse Communities. The five national organizations were funded to provide training and technical assistance (T/TA), each focusing on one of the five components.
Focusing on the ASRH services component given its influence on later projects developed by CDC's Division of Reproductive Health, state- and community-based organizations partnered with at least five health centers (e.g., community health centers [CHCs], health departments) and, with support of the national T/TA organization funded for this purpose, Cicatelli Associates, Inc., (CAI), provided T/TA on quality improvement (QI). QI focused on implementation of recommended SRH services and youth-friendly practices in the following six domains: contraceptive access; quick start provision of contraception; STD/HIV testing and treatment; cost, confidentiality, and consent; health center infrastructure; and health center environment.
CWI had a twofold approach to increasing access to quality ASRH services. The first strategy involved referral of adolescents participating in evidence-based teen pregnancy prevention programs to partner health centers, which was facilitated by formal or informal agreements between partner health centers and the youth-serving organizations (YSOs) implementing the evidence-based programs.
A second strategy involved the three community engagement components of the program intended to build community support for ASRH services and evidence-based teen pregnancy prevention programs. These community engagement components have been described in detail previously. 23,24 In brief, with Community Mobilization, each grantee mobilized the community, including youth, through the creation of community partner teams integral to planning and implementing program activities. Stakeholder Education involved grantees and the community partner teams engaging in broad community education about local teen pregnancy data and evidence-based prevention strategies. The Working with Diverse Communities component was integral for addressing health equity and included engaging communities disproportionately affected by teen birth and ensuring Community Mobilization efforts involved a diverse set of civic leaders and members.
Evaluation findings suggest that the ASRH component of the community-wide approach was effective at improving several ASRH best practices among participating health centers. Among health centers participating in the CWI, there was an increase in the number with policies for routine sexual health assessment, increased availability of hormonal contraception and intrauterine devices (IUDs) and same-day initiation of IUDs, and improvement on several youth-friendliness measures. 24 In addition, evaluation results showed significant increases in contraceptive coverage* and utilization of long-acting reversible contraception over the course of the intiative. 24 These results complement other studies documenting the benefits of strengthening ASRH services, including improved behavioral outcomes, 6,7,25 –27 improved client knowledge and satisfaction, 6,28,29 and reductions in teen pregnancy and births. 8,30
Focus on QI and Community–Clinical Linkages
Following the CWI, CDC implemented the Teen Access and Quality Initiative (TAQ) from 2015 to 2020. This demonstration project focused specifically on improving access to and quality of ASRH services. The TAQ program model (Fig. 1) was similar to the ASRH services component of CWI. Nonprofit organizations in three southern states partnered with publicly funded health centers and CAI to support QI related to delivering recommended SRH services and implementing youth-friendly practices. 31 For the access component, grantees partnered with local YSOs to improve YSO staff knowledge related to ASRH and to support referrals to health centers. 32
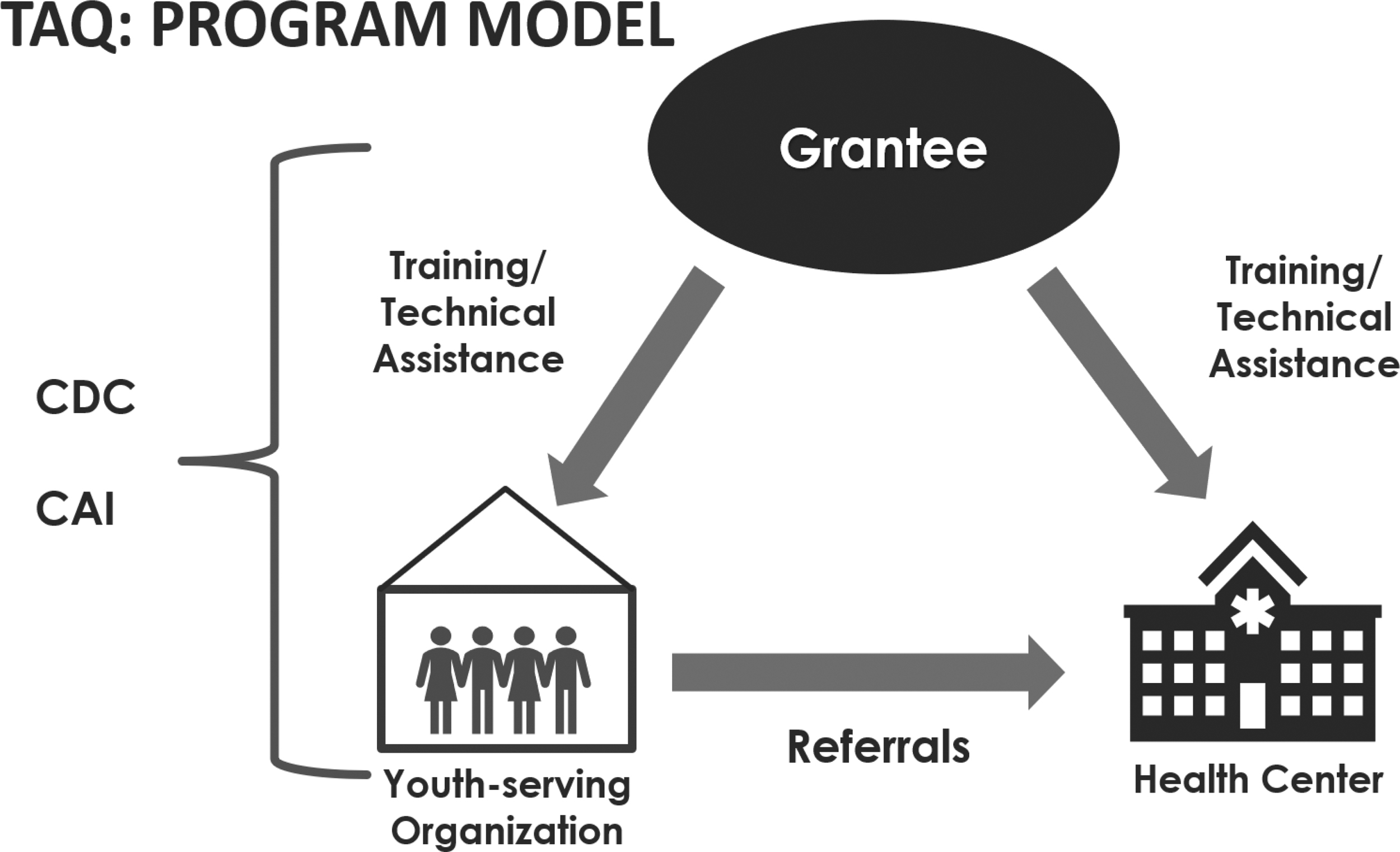
Teen Access and Quality Initiative program model. CAI, Cicatelli Associates, Inc.; CDC, Centers for Disease Control and Prevention; TAQ, the Teen Access and Quality Initiative.
Promoting health equity was a central goal of TAQ. Funded grantees worked in communities where the teen birth rate exceeded the national average and, by collaborating with publicly funded health centers and YSOs such as those working in juvenile justice or foster care, the initiative aimed to reach young people disproportionately affected by adverse SRH outcomes.
Clinic-based QI activities included partnership building, staff training, workflow modifications, and parent and adolescent engagement. As an example, use of process mapping at one CHC in North Carolina identified opportunities to modify the workflow to ensure time alone between adolescent patients and clinical staff; the revised workflow also included distribution of parent educational materials on adolescent confidentiality policies and practices. 33
Grantees worked with health center partners to collect performance measure data quarterly to guide improvement activities and overall project evaluation. Health center organizational assessments, provider surveys, and adolescent patient surveys were also conducted periodically over the course of the project. Baseline data suggested a particular need to increase availability of long-acting reversible contraception and communication about confidentiality, 34 and outcome analyses are underway.
To address access, staff training was a key activity with YSO partners. Topics addressed included what ASRH services are recommended and why, where, and how to refer adolescents to ASRH services (including how to develop a referral policy and create a referral guide), what adolescents should expect at a clinic visit, and state laws and regulations related to minors' rights and confidentiality. Preliminary data from YSO staff surveys suggest that knowledge and confidence about providing youth with ASRH information improved. 35 YSO partners also focused on conducting community engagement activities to build community support for adolescent access to quality SRH services, similar to CWI, although at a smaller scale.
Moving Toward Scale
Through CWI and TAQ, CDC and its partners have developed strategies, tools, and resources to support implementation of health center QI initiatives focused on strengthening recommended ASRH services and youth-friendly practices. 36 –39 Other organizations have also developed and tested ASRH-related QI implementation materials. 40 –43 To synthesize these resources and facilitate scale-up of QI related to ASRH care provided specifically in the context of primary care in CHCs, CDC launched the Quality and Access for Reproductive Health Equity (QARE, pronounced “care”) for Teens project in 2020 in collaboration with the National Association of Community Health Centers (NACHC). CHCs are an important setting in which to improve equitable access to and quality of ASRH care as they serve areas where economic, geographic, or cultural barriers limit access to affordable health care; provide services regardless of patients' insurance status or ability to pay; and have governing boards largely made up of CHC clients. 44,45 Across the United States in 2019, nearly 1500 CHCs funded by the Health Resources and Services Administration collectively served more than 2.25 million 15- to 19-year-old adolescents, 11% of the U.S. population aged 15–19 years. 46
A central goal of QARE for Teens is to develop a QI package that collates existing change strategies (i.e., actionable strategies that can be rapidly implemented and evaluated to assess improvements) and related tools and resources, similar to other change packages developed by CDC. 47 –49 To identify content for the QI package, NACHC and CAI convened 26 experts in ASRH, QI, and health equity, including academic researchers, health care providers, T/TA specialists, and national association representatives. In addition, CAI conducted an environmental scan of QI initiatives described in peer-reviewed and gray literature.
Through these activities, the following change strategies were identified: (1) establishing and leveraging administrative and clinical champions for ASRH QI efforts; (2) training both clinical and nonclinical staff, as appropriate, particularly related to client-centered contraceptive counseling, long-acting reversible contraception services, and confidentiality practices; (3) modifying workflows; (4) enhancing health information systems; and (5) engaging adolescents and parents. Engagement of adolescents and parents was identified as a particularly important change strategy for promoting health equity. Specific trainings, process mapping tools and example workflows, electronic health record templates, and adolescent and parent materials were identified as resources to help implement these change strategies. With input from clinical leaders at CHCs, a draft QI package has been developed and will be piloted in selected health centers before being finalized and widely disseminated.
QARE for Teens is addressing adolescent access to SRH services in two ways. First, improving quality of care through QI initiatives, particularly around confidentiality practices, has the potential to also enhance adolescent access to services, given that confidentiality concerns are a known barrier to adolescent health care seeking. 19 Second and separate from the QI package, QARE for teens is developing resources to support provision of ASRH services via telehealth, recognizing that innovative models for delivering services outside of the clinic setting can also improve access. Like the ASRH QI package, these resources will be piloted in several CHCs, revised as needed, and then disseminated.
Future Directions
From more than a decade of work addressing access to and quality of ASRH services, we have identified and developed strategies and resources to improve the quality of ASRH services. By compiling these resources into a user-friendly package for CHCs, we aim to minimize the development of duplicative materials and support QI implementation to reduce disparities in access to quality care. This package can also provide a foundation for future adaptations, such as supporting ASRH QI initiatives in clinical settings other than CHCs.
Complementary packages addressing access to ASRH services could be developed for clinical and community audiences. Such a resource could include strategies and tools related to delivery of ASRH services via telehealth, such as those being developed as part of QARE for Teens. TAQ data also highlighted the importance of parents in facilitating adolescent access, as parents were the most common referral source reported by adolescent patients. 50 Resources for parents to support adolescent health care seeking, including through parent–adolescent communication about SRH services, may be beneficial.
Health equity in ASRH has been a key aim of all of the initiatives described in this report, however, this remains a critical yet unattained goal within the United States. 51 Community engagement is one important approach to promoting health equity, 52,53 and the CWI employed extensive and diverse community engagement strategies, including engagement of adolescents from communities disproportionately affected by teen pregnancy. However, there is a need to identify the most effective and feasible community engagement strategies and tools in relation to supporting adolescent access to care. The collection and use of local-level data can help identify which community engagement strategies and tools have the potential to be most effective. One method well suited for this purpose is rapid ethnographic assessment (REA), which involves iterative qualitative data collection and analysis to develop an understanding of a local issue of concern and develop tailored actionable strategies to address it. 54 With a state, regional, and local health department, we are currently conducting an REA that is exploring the impact of the coronavirus disease 2019 (COVID-19) pandemic on equitable access to quality ASRH services in a rural southern county with disproportionately high rates of teen births and STDs. Such community-engaged research can potentially be used in other ways to promote health equity, such as understanding the pathways by which ongoing structural and interpersonal racism may contribute to racial/ethnic disparities in ASRH outcomes, including those related to access to care.
Another future direction for public health includes population-based data collection on access to and quality of ASRH services. The field could benefit from additional national- and state-level data on access to and quality of ASRH services, such as adolescents' sources of information, knowledge about minors' rights and other confidentiality protections, and satisfaction with care. Routine collection of such data would allow for monitoring over time and could inform what interventions should be prioritized, including those that build upon the initiatives described in this report to support access to quality SRH care for all adolescents in the United States.
Footnotes
Disclaimer
The findings and conclusions in this report are those of the authors and do not necessarily represent the official position of the Centers for Disease Control and Prevention.
Acknowledgments
We acknowledge and thank our colleagues for contributions to the initiatives described in this article. This includes Kim Burley, Taleria R. Fuller, L. Duane House, Trish Mueller, Teresa Powell-Robinson, Lisa Romero, Alison Spitz, Heather D. Tevendale, Bala Venugopalan, and Carla P. White. We thank each of the funded organizations and their community partners for implementing the Teenage Pregnancy Prevention: Integrating Services, Programs, and Strategies through Community-Wide Initiatives, the Teen Access and Quality Initiative, and Quality and Access for Reproductive Health Equity for Teens and for their dedication and innovation in promoting adolescent sexual and reproductive health in the United States. We recognize the essential contributions of the U.S. Department of Health and Human Services Offices of Population Affairs and Adolescent Health to the described work.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received to assist with the preparation of this manuscript.