
Abstract
Background:
The impact of gender on outcomes in patients suffering from coronavirus disease 2019 (COVID-19) is frequently debated. However, the synchronous influence of additional risk factors is seldom mentioned. With increasing emphasis on identifying patients who are at risk of complications from COVID-19, we decided to conduct a retrospective review to assess the influence of age and body mass index (BMI) on gender-based differences in outcomes.
Materials and Methods:
A retrospective review of 1288 patients was conducted at a tertiary care hospital. Binary logistic regression was used to assess differences in risk factors and outcomes between genders. The associations between predictors and outcomes were described using odds ratios in tables, forest plots, and regression curves plotted using Sigma Plot.
Results:
Majority of patients were women (53.6% vs. 46.4%). Median BMI in men was higher than women (p = 0.003). Key predictors for all-cause morbidity/mortality in men were diabetes, chronic kidney disease, and regular use of angiotensin-converting enzyme inhibitors. In women, age >65 and regular use of inhaled steroid were additional risk factors. Men had a higher risk of acute respiratory distress syndrome (2.83 [1.70–4.70]), acute renal failure (1.96 [1.20–3.20]), and had a longer length of stay (0.11 [1.52]). Obesity has a stronger bearing on outcomes in women, and age has a more pronounced effect on outcomes in men.
Conclusion:
Extremes of BMI and older age are associated with worse outcomes in both men and women. Obesity has a stronger bearing on outcomes of COVID-19 infection in women, while the effect of older age on outcomes is more pronounced in men.
Introduction
The coronavirus disease 2019 (COVID-19) pandemic, caused by severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), has infected ∼261 million people globally as of November 2021. 1 Vaccination against the SARS-CoV-2 strain was introduced in December 2020 and campaigns to increase vaccination coverage have achieved an 82.7% vaccination rate across the United States for adults, with at least one vaccination. 2 Restrictions implementing protective practices such as physical distancing and use of face masks are being lifted formally in many areas with adequate vaccination coverage.
However, the emergence of the delta and omicron variants, informal relaxation of protective practices in areas with inadequate vaccination coverage, and uncertain immunization rates achieved through vaccination threaten another global crisis. Identification of patients at a higher risk of clinical deterioration and poor prognosis following infection is one strategy of facilitating a system of selective implementation of protective restrictions to minimize disease burden as the world reverts to prepandemic practices.
Gender is a major risk factor for SARS-CoV-2 infections that influences the prevalence of the disease and its clinical outcomes. Prior studies investigating gender differences have found increased rates of cardiac, renal, and respiratory complications, mortality, and length of hospital stay in men infected with COVID-19. 3 –10 However, others reported contradictory findings, where no gender-based differences in outcomes were observed between men and women. 8 Similarly, the influence of risk factors on both genders varies; however, the extent to which these risk factors influence gender-based outcomes has not been studied.
With increasing emphasis on identifying patients who are at risk of complications from COVID-19, we decided to conduct a retrospective review to assess the influence of age and body mass index (BMI) on gender-based differences in outcomes. In addition to this, we also identified the differences in risk factors and outcomes between both genders.
Materials and Methods
Before conducting the study, the study was approved by the Committee on Clinical Investigations (CCI), the Institutional Review Board (IRB) for the Beth Israel Deaconess Medical Center, Boston, MA. The need for informed consent was waived.
Study setting and participants
We conducted a retrospective review of the hospital course of 1355 patients who were admitted between March 2020 and August 2020 at the Beth Israel Deaconess Medical Center in Boston. All patients admitted with a primary diagnosis of COVID-19, confirmed using a reverse transcription-polymerase chain reaction test, were included in the study. Patients younger than 18 years and patients with missing variables (gender [n = 30] and age [n = 49]) were excluded from the study (Fig. 1). Data were electronically exported using Medical Record (MR) numbers from the hospital's system. All patients were deidentified.

Flow diagram of data extraction from Beth Israel Deaconess Medical Center patient database.
Variables
Independent variables: Data were manually extracted for 25 relevant variables. Relevant variables were chosen based on prior studies investigating COVID-19 impact on patient outcomes (Supplementary Appendix S1). Key demographic variables of interest included age, gender (men or women), and BMI. Patient comorbidities included history of smoking, history of kidney disease, alcohol use, diabetes, hypertension, stroke, asthma, chronic obstructive pulmonary disease, pneumonia, and obstructive sleep apnea (OSA) (Table 1). We also collected data on the use of statins, diuretics, aspirin, beta-blockers, acetaminophen, bronchodilator, calcium channel blockers, angiotensin-converting enzyme (ACE) inhibitors, inhaled steroids, angiotensin receptor blockers (ARBs), nonsteroidal anti-inflammatory drugs, insulin, and metformin (Table 1). In addition to this, data for presenting symptoms were also collected for patients admitted to the hospital (Fig. 2) (Supplementary Appendix S2).

Gender-wise comparison of presenting symptoms for COVID-19 patients admitted to the university hospital. COVID-19, coronavirus disease 2019. * indicates significant statistical difference between males and females in presenting symptoms at time of admission.
Patient Comorbidity and Drug Use Characteristics Stratified by Gender
Data are presented as n (%) or median (Quartile 1-Quartile 3).
ACE, angiotensin-converting enzyme; BMI, body mass index; COPD, chronic obstructive pulmonary disease; NSAID, nonsteroidal anti-inflammatory drug.
Outcome variables
Outcome data were recorded for all patients during the intrahospital stay. All postoperative complications were recorded for the duration of the hospital stay unless specified otherwise. This included acute respiratory distress syndrome (ARDS), acute renal failure (ARF), cardiac complications (congestive heart failure, myocarditis, QT prolongation, arrhythmias, or cardiac arrest), and sepsis/bacteremia complications, along with mortality. In addition to this, data for intensive care unit (ICU) admissions and length of stay were also collected (Table 2). All-cause morbidity and mortality were defined as mortality or morbidity during hospitalization (cardiac complication, ARDS, sepsis/bacteremia, or renal failure).
Gender-Wise Comparison of Patient Outcomes Following Hospital Admission
Statistical significance p < 0.05 shown in bold.
Data are presented as n (%) or median (Q1–Q3) unless stated otherwise.
p < 0.05 is threshold for significance following Bonferroni's correction.
Adjusted for: BMI, alcohol use, aspirin, asthma, and gender.
Cardiac complications include congestive heart failure, myocarditis, QT prolongation, heart arrhythmia, and cardiac arrest.
BMI, body mass index; ICU, intensive care unit.
Statistical analysis
Data analysis was performed using SPSS Version 27, IBM Corporation. A descriptive analysis of all demographic variables including medication history and features of their hospital stay was conducted. The Shapiro–Wilk test for normality (p > 0.05) was used to assess all continuous demographic variables against all-cause morbidity and mortality to satisfy the assumption of normality for gender.
For normally distributed data, mean ± standard deviation was used to describe central tendencies, while median (interquartile range) was used to describe central tendency for skewed data. We used the multivariable regression model to identify differences in risk factors for all-cause morbidity and mortality in both genders independently and described our findings using a forest plot. To show how the effects of BMI and age on outcomes of COVID-19 infection are influenced by gender, we used Sigma plot to depict the probability of all-cause morbidity and mortality with varying BMI in men and women separately. The cutoff for univariate analysis was <0.25, while the cutoff for multivariable regression was p < 0.05. Variables found to be insignificant in univariate analysis were excluded from the multivariable analysis.
A linear regression model was used to assess differences in length of stay between both genders. Bonferroni's correction was applied to adjusted p-values to reduce risk of type-I errors.
Results
Patient characteristics
In the 1188 patients included in the study, the majority of the patients were women (n = 604, 53.54%) (Table 1). There was no difference in median age (men [m] = 63 years, women [f] = 62 years, p = 0.3), however, men had a significantly higher median BMI than women (m = 30, f = 28.4, p = 0.003), daily alcohol use (17.2% vs. 10.4%), and use of aspirin before admission (16.4% vs. 10.3%). Similarly, a significantly larger number of women, compared with men, with preexisting asthma were admitted for COVID-19-related symptoms (6.8% vs. 3.8%).
There was no evident difference in mortality between the two genders (m = 4.2%, f = 3.6%, p = 0.631). However, men were more frequently admitted to the ICU (m = 42.7%, f = 29.0%) and had a much larger comorbidity burden.
Risk factors
Results of the multivariable regression analysis, examining risk of all-cause morbidity and mortality, found several statistically significant predictors, identifying hypertension and daily alcohol use as risk factors for both genders (Fig. 3). Key risk predictors in men with COVID-19 include age >65 (1.97 [1.07–3.96], p = 0.017), diabetes (2.22 [1.07–4.59], p < 0.001), history of kidney disease (0.36 [0.14–0.88], p = 0.023), and preadmission use of ACE inhibitors (3.05 [1.21–7.70], p < 0.001). In women, age >65 (2.16 [1.09–4.29], p = 0.013) and prior use of inhaled steroids (3.75 [1.34–10.50], p = 0.24) were significantly associated with a higher risk of morbidity and mortality.
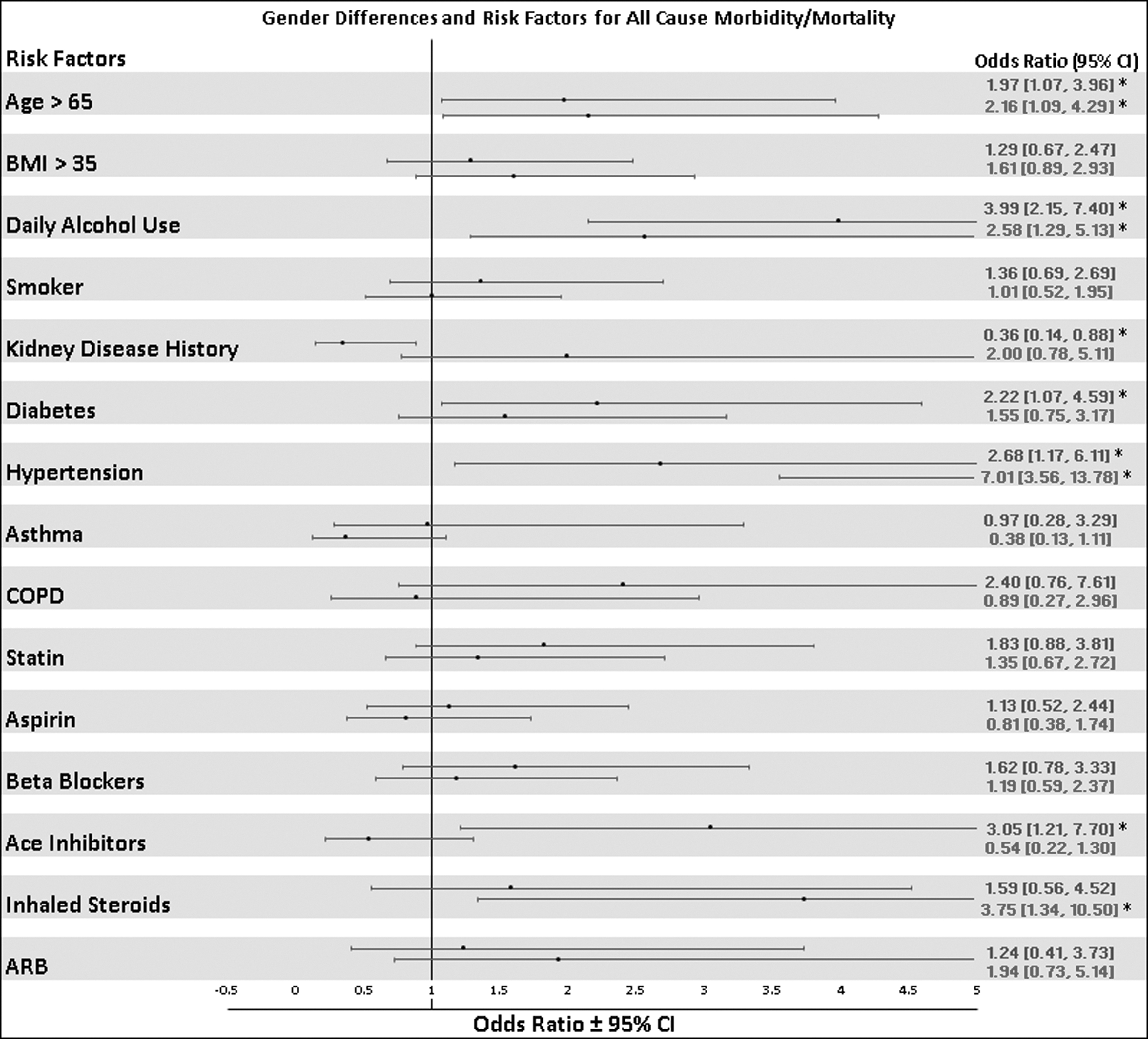
Comparison of risk factors among men and women for adverse outcomes during hospital admission. Odds ratio and 95% confidence intervals are determined by comparing the relative risk of all-cause morbidity and mortality within the same gender.
Patient outcomes
In a multivariable regression model, men were associated with a higher risk of ARDS (2.83 [1.70–4.70], p < 0.001), ARF (1.96 [1.20–3.20], p = 0.044), and longer length of stay (0.11 [1.52], p < 0.001) (Table 2). We observed no difference in mortality (1.24 [0.62–2.48], p = 0.99), total duration in ICU (−0.14 [2.13], p = 0.63), occurrence of sepsis/bacteremia (1.56 [0.76–3.22], p = 0.99), and cardiac complications (0.72 [0.36–1.43], p = 0.99) between men and women in our regression analysis model.
Impact of age and BMI
The effect of age and BMI on probability of morbidity and mortality following COVID-19 infection varies between men and women (Figs. 4 and 5). At lower BMIs (20–35 kg/m2), women had a lower probability of adverse outcomes from COVID-19 infection than men. At higher BMIs (>40 kg/m2), however, the influence of BMI on outcomes was more pronounced for women than men as indicated by a steeper gradient of the trend line for women (Fig. 4).
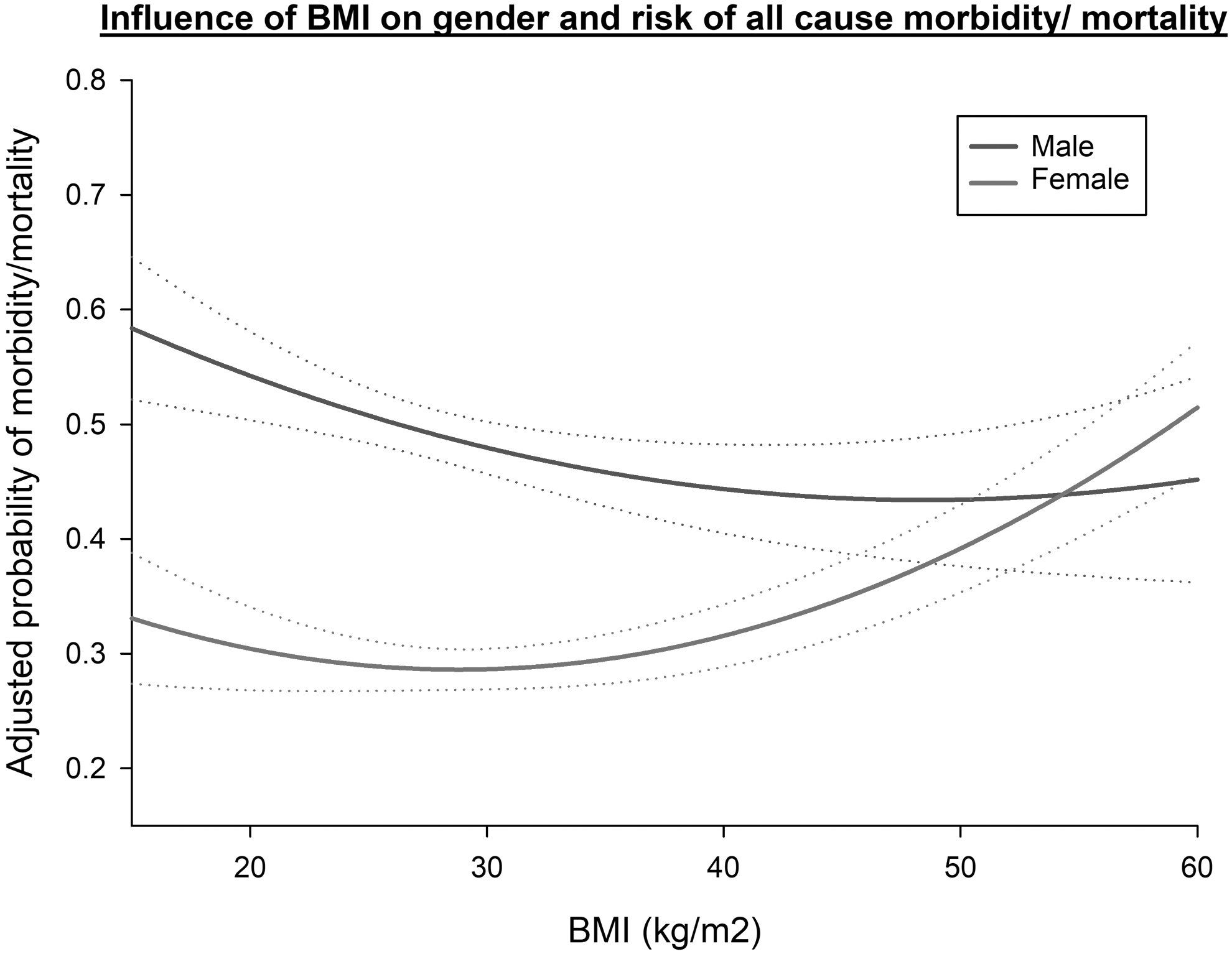
Gender-wise comparison of BMI influence on all-cause morbidity and mortality. Probability of all-cause morbidity and mortality has been adjusted for BMI, asthma, aspirin use, and history of alcohol use. Dotted line represents 95% confidence interval (CI).
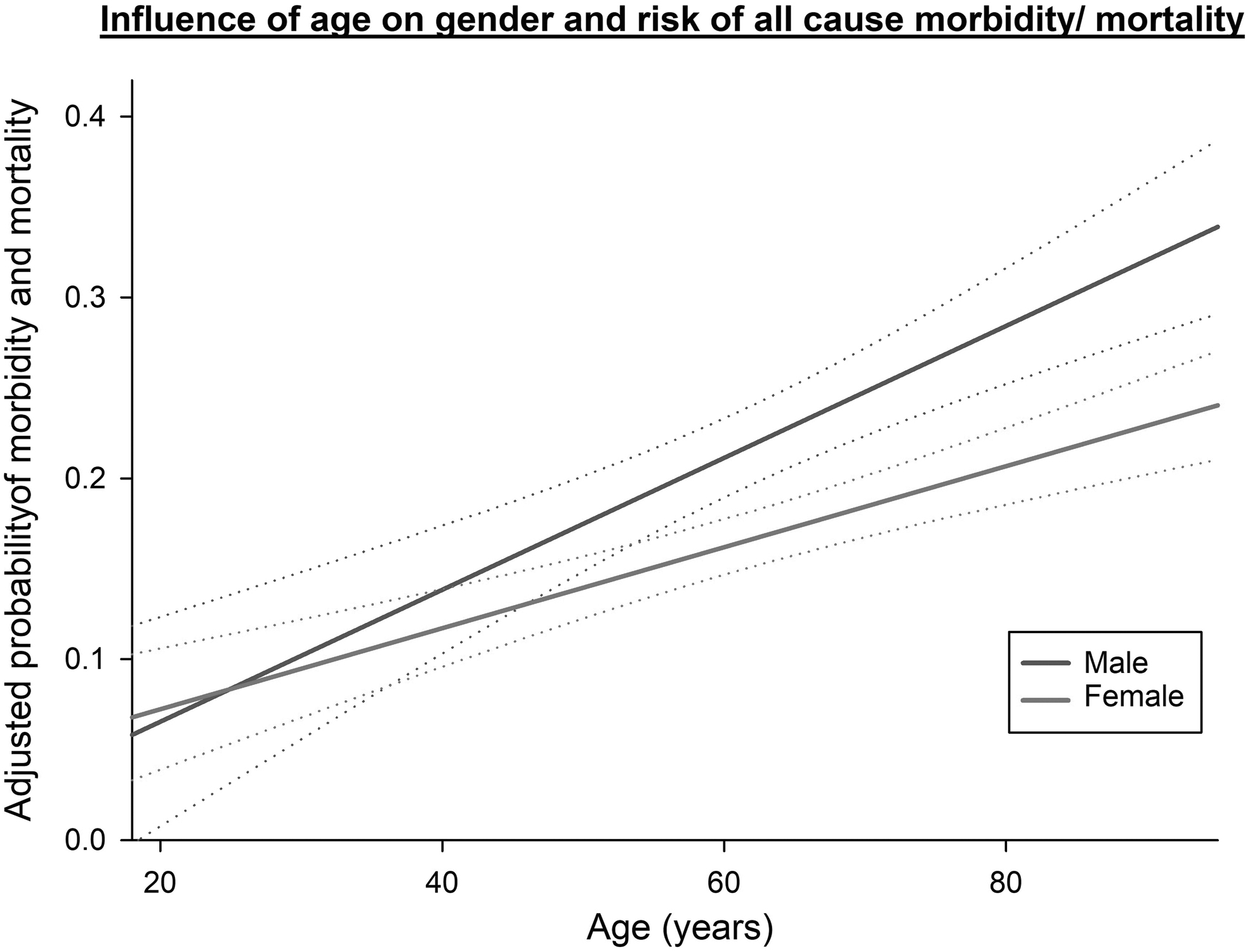
Gender-wise comparison of age influence on all-cause morbidity and mortality. Probability of all-cause morbidity and mortality has been adjusted for BMI, asthma, aspirin use, and history of alcohol use. Dotted line represents 95% confidence interval (CI).
Increasing age was associated with higher incidence of morbidity and mortality in both genders. However, increasing age had a greater bearing on outcomes in men than women (Fig. 5).
Discussion
The novel finding of our study shows that extremes of BMI and age influence men and women differently, where the increasing BMI has a stronger bearing on outcomes in women and increasing age has a more pronounced effect on outcomes in men. In addition to contributing to the pool of evidence for gender-based differences in outcomes, our finding is of significant importance in identifying patients at high-risk of complications from COVID-19 infection. Given the waning of vaccine-induced immunity, inequity in vaccine accessibility, surges in infections from newer variants, and struggle to increase booster coverage rates, the identification of risk factors for poor outcomes is particularly helpful in adopting a targeted approach to booster dosing toward patients who would benefit most.
Our study also confirms prior findings of significantly higher incidence of ARDS, renal failure, ICU admissions, and prolonged length of hospital stay following COVID-19 infections in men, however, we observed no differences in mortality. 7,9,11,12
Numerous efforts have been made to understand the biological causes underlying the observed gender differences, and several potential mechanisms involving ACE-2 expression and immune system responses have been identified. 3,13 –15 Cell membrane-bound ACE-2 has been implicated as the receptor for internalization of SARS-CoV-2. This receptor is expressed in a greater concentration on the surface of several pulmonary and extrapulmonary cell types, including cardiac, renal, intestinal, and endothelial cells in men, and may promote viral internalization, replication, and subsequent viral load and immune reaction. 16,17 Similarly, chemokine and immune cell analyses have also shown differential immune responses to COVID-19 infection in men and women. 15,17 However, despite observing significant differences in morbidity between men and women, we saw no difference in mortality. Prior evidence on differences in mortality is conflicting; however, consensus among meta-analyses has reported independently significant higher mortality in men. 4 –6
Similar to previous literature, we observed several differences in predictors of poor outcome (morbidity and mortality) between men and women (Fig. 3). The use of ACE inhibitors was an interesting risk factor for poor outcomes in men in our study. Although differences between genders are multifactorial, recent studies have shown a paradoxical increase in ACE-2 (receptor for viral internalization) expression following the use of ACE-1 inhibitors and ARBs, which could favor SARS-CoV-2 infection by promoting viral internalization into host's cells and tissues. 18,19 The influence of the use of ACE inhibitor and ARBs may possibly be different in men and women, however, this has not been reported in the past.
The association of obesity with worse outcomes following COVID-19 infection has been reported by previous studies. 11,20 –22 Aside from confirming these findings, our study goes a step beyond and identifies that obesity has a greater bearing on outcomes of COVID-19 infection in women than men. Our results show that, at normal ranges of BMI, the probability of adverse outcomes is lower in women than men. At higher BMIs, the increase in probability of adverse outcomes in women is greater than that of men and even crosses that of men at very high BMIs (>55 kg/m2). This highlights that obesity is a more important consideration for women than men in impacting outcomes of COVID-19 infection.
However, the number of patients with high BMIs is low and results should be interpreted with caution. Obesity has been recognized as a proinflammatory state by several studies. 11,20 –22 Infections with COVID-19, such as many other viral illnesses, exert most damage through induction of an inflammatory state in the body. 22 The difference in outcomes between men and women in response to obesity can be explained by a greater body mass of adipose tissue in women as opposed to lean body mass in men. In addition to this, obesity is well known for causing lung volume changes including low functional reserve capacity, right heart dysfunction, and increases the incidence of OSA. These changes may increase the likelihood of poor outcomes following COVID-19 infection.
Prior studies have also described worse outcomes in elderly patients. 5,23 They have been attributed to increased comorbidity burden and frailty in large, however, the association persists despite adjusting for potentially confounding comorbidities in several studies. 5,7,23 This can be, in part, attributed to inflamm-aging. 22 –24 Inflamm-aging describes subclinical systemic inflammation owed partially to immunosenescence in older individuals. We also observed a more pronounced effect of increasing age on worse outcomes in men and women, in patients with COVID-19. This may also be explained by accelerated inflamm-aging and immunosenescence in men, reported in prior studies. 22,25 In addition, decreased levels of soluble anti-inflammatory ACE-2 have been shown in older men compared with older women. 20,25
Strengths and limitations
This study is a retrospective review that is able to suggest broad associations and display data trends. However, no definitive cause-and-effect relationships can be established. Our study was conducted only in patients who were hospitalized for COVID-19, representing a subset of the population who are suffering from severe disease. However, accounting for outcomes in asymptomatic or mildly symptomatic patients is challenging as the majority of patients are undiagnosed. We could not record the laboratory and preadmission values for a large population to include in our study, however, we recommend the inclusion of these values in future studies.
In addition, the number of patients at extremes of BMI (<20 and >50 kg/m2) in our study is small. Further evidence from larger studies is needed to derive definitive conclusions. This is the first study assessing the influence of age and BMI on gender-based outcomes in addition to assessing gender differences in outcomes. Lastly, as all patients were hospitalized during a 3-month period, no significant changes in practice for COVID-19 treatment were made during this time, ensuring uniformity in the management of patients.
Conclusion
Our study demonstrates that men have greater morbidity, including ARDS, renal failure, ICU admissions, and prolonged length of stay, following infection with COVID-19 compared with women. Our findings also show that increasing age is associated with worse outcomes in both men and women. We also observed that increasing BMI may have a stronger bearing on outcomes of COVID-19 infection in women compared with men.
Ethics Statement
Before conducting the study, the study was approved by the CCI at the Beth Israel Deaconess Medical Center, Boston, MA. The need for informed consent was waived.
Footnotes
Acknowledgments
We thank the CORE Steering Committee—L. Farrell, A. Asnani, S. Parikh, E. Baedorf Kassis, S. Bose, A. Collier, R. Gerszten, D. Katz, D. Krakower, M. Lai, A. Law, J. Patel, N. Shapiro, G. Szabo, J. Zwicker, and the numerous research assistants and fellows who contributed to data collection.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Supplementary Material
Supplementary Appendix S1
Supplementary Appendix S2
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.