
Abstract
Background:
Suicide is a public health issue, and there are differences between men and women in terms of suicide ideation, behavior, and completion. Obstetrician/gynecologists (OB/GYNs) are uniquely positioned to assess women's suicide risk.
Materials and Methods:
A 53-question survey was distributed to the Pregnancy-Related Care Research Network, assessing practice, attitudes, and knowledge regarding suicide risk assessment and management, and personal experience with suicide. Wilcoxon signed-rank tests with paired samples were used to compare the frequency of screening and interventions for different groups of women, and practices of those with and without suicide experience. Significance was set at p < 0.05.
Results:
Response rate was 31.9%. Respondents were largely White females. OB/GYNs reported more frequently screening for suicide ideation/intent/behavior among pregnant and postpartum patients than nonpregnant/nonpostpartum patients of childbearing age. The most common assessment tool was the Edinburgh Postnatal Depression Scale; half ask about past suicide ideation/behavior or current thoughts/plans. The most common intervention for at-risk patients was a mental health referral; all interventions were reported more frequently for pregnant patients. Common barriers to screening were inadequate mental health services, time constraints, and inadequate training. Most agreed suicide screening is within their purview, and were knowledgeable about the topic, although gaps were identified. Few reported adequate training in suicide risk assessment, and believed continuing education would be beneficial. A majority endorsed experience with suicide and some practice differences emerged.
Conclusions:
OB/GYNs view suicide risk assessment in their scope. Some knowledge gaps were identified, and respondents believe additional training would be beneficial.
Introduction
Suicide is a public health problem 1 that can have wide-ranging consequences. 2 –8 Despite significant efforts to eliminate suicide, it continues to be a leading cause of death in the United States. 1 For females, the age-adjusted suicide rates increased significantly (by 53%) between 1999 and 2017, growing from 4.0 per 100,000 in 1999 to 6.1 in 2017. 9 In fact, suicide is now a leading, and preventable, cause of maternal mortality. 10 –12
There are a number of differences between men and women in terms of suicide ideation, suicide behavior, and death by suicide. For example, females engage in nonsuicidal self-directed violence, and also make more suicide attempts, than males. 13,14 They also tend to use less lethal means during attempts, 14 although firearms are a common means of completed suicide for women. 1 Furthermore, women have a greater lifetime prevalence of suicide ideation, 15 although they die less often by suicide than men do. 13,14 Women are also more likely to experience sexual abuse, sexual trauma, and intimate partner violence, 16 –19 traumatic experiences that contribute to suicide risk. Furthermore, women's suicide ideation and behavior fluctuate over the course of the reproductive and life cycle, and may be increased in the context of premenstrual dysphoric disorder, 20,21 oral contraceptive use, 22 pregnancy, 23,24 postpartum, 25 perimenopause, 26 and hormone replacement therapy. 27
Suicide and suicide risk are complex, 28 but accurately identifying and mitigating suicide risk among women is an essential aspect of suicide prevention and women's health efforts. Almost half of all individuals who die by suicide had a physician visit in the month before their death, and about one-third were seen in the week before suicide; women who died by suicide were more likely to have had health care contact than men. 29 Therefore, we must highlight the need for women's health care providers, such as obstetrician/gynecologists (OB/GYNs), to be knowledgeable about suicide as a preventable cause of women's morbidity and mortality, and be willing and able to screen for and mitigate risk. 30,31
Unfortunately, suicide screening is often not part of a clinical encounter. For example, in a study of primary care providers, suicide was discussed in about 1 in 10 encounters with patients who had screened positive for suicidal ideation. 32 Similarly, just over one-third of primary care physicians discussed suicide in encounters with standardized patients who presented with major depression or adjustment disorder or sought antidepressants. 33 One study of prenatal visits in a community-based, academic-affiliated, obstetrics practice primarily serving a Medicaid-insured population revealed that only four of the nine participants endorsing suicidal ideation had a suicide risk assessment documented in their chart. Few who had discussed issues related to mood at intake had documented follow-up at the second visit, even when they saw the same provider. 34
There are many barriers to conducting suicide screening, such as limited clinician confidence, 35,36 limited knowledge and training, 37 clinician attitudes, 38,39 limited access to mental health resources, 40 low compensation for behavioral health problems, 37 among others. 41 However, little, if any, literature has specifically explored OB/GYNs' attitudes, knowledge, and practice regarding suicide risk screening. As such, this article fills this gap by surveying practicing OB/GYNs about these topics as a critical step in identifying areas for improvement with regard to suicide prevention among women.
Materials and Methods
A 53-question, web-based, cross-sectional survey was developed for the current study. The survey assessed provider practice regarding suicide risk assessment and management, barriers to suicide risk assessment, knowledge on risk factors for suicide, attitudes and beliefs about suicide, and personal experience with suicide (through a friend, family member, or patient). Questions included yes/no, select all that apply, and 5-point Likert-type formats.
The survey was distributed by email to all physicians registered with the Pregnancy-Related Care Research Network (PRCRN; N = 524). The PRCRN is a research program based at the University of Washington that aims to improve women's health care by surveying a national convenience sample of OB/GYNs who provide care to pregnant patients, women, or patients with female reproductive organs in the United States. Providers registered with the PRCRN have consented to receiving quarterly surveys about their practice patterns and knowledge. PRCRN recruits physicians by contacting OB/GYNs from American College of Obstetricians and Gynecologists' membership lists. Physicians in the PRCRN must have completed residency and be board certified. The PRCRN is supported by the Health Research and Services Administration Grant UA6MC31609 and has University of Washington Institutional Review Board (IRB) approval for all surveys distributed to registered PRCRN providers.
The survey was distributed through Qualtrics (Qualtrics; Provo, UT), a commercial survey sampling company, during July and August 2021 to PRCRN providers nationwide. Seven weekly reminders were sent to providers who had not responded to the survey. PRCRN-registered providers consent to survey participation within each survey. The time commitment of the survey was estimated to be 15 minutes.
All data cleaning and analysis were completed in R Version 4.1.1. 42 Unweighted proportions were calculated to summarize the data. Medians were calculated to summarize the Likert scales for frequency of screening for mental health disorders and use of interventions used to address suicide risk (1 = Never, 5 = Frequently). Wilcoxon signed-rank test with paired samples was used to compare the frequency of providers screening for mental health disorders in pregnant women, postpartum women, and perimenopausal women, compared with nonpregnant, nonpostpartum women of child-bearing age. Additionally, Wilcoxon signed-rank test with paired samples was used to compare the frequency of providers using specific interventions (prescribing psychotropic medication, mental health referral, safety planning, etc.) to address suicide risk in pregnant women, postpartum women, and perimenopausal women, compared with nonpregnant, nonpostpartum women of child-bearing age.
Wilcoxon signed-rank test with unpaired samples was also used to compare medians of the Likert scales for frequency of screening and use of interventions to address suicide risk by providers with and without personal or patient experiences with suicide. A significance level of 0.05 was used to determine statistical significance.
Results
Respondents
One hundred sixty-seven providers responded to the survey (31.9%). Demographics are presented in Table 1.
Demographics of Respondents (N = 167)
OB/GYN, obstetrician/gynecologist; SD, standard deviation.
Clinical practice
Figure 1 depicts the frequency with which respondents reported screening specific patient populations for suicide ideation, intent, or behavior. A majority reported “often” or “frequently” screening for suicide ideation/intent/behavior among pregnant (57.5%) and postpartum (70.7%) patients, compared with only 40.1% often or frequently screening nonpregnant, nonpostpartum patients of childbearing age. The median response for frequency of screening nonpregnant, nonpostpartum patients of childbearing age for suicide ideation/intent/behavior was “sometimes” (median = 3), whereas the medians for screening pregnant and postpartum patients were “often” and “frequently,” respectively (median = 4, median = 5). The median for the nonpregnant, nonpostpartum group was significantly higher for the pregnant (p < 0.01) and postpartum (p < 0.01) groups. Figure 2 portrays the percent of respondents who reported often or frequently screening for various mental health and substance use issues, stratified by patient subgroups.
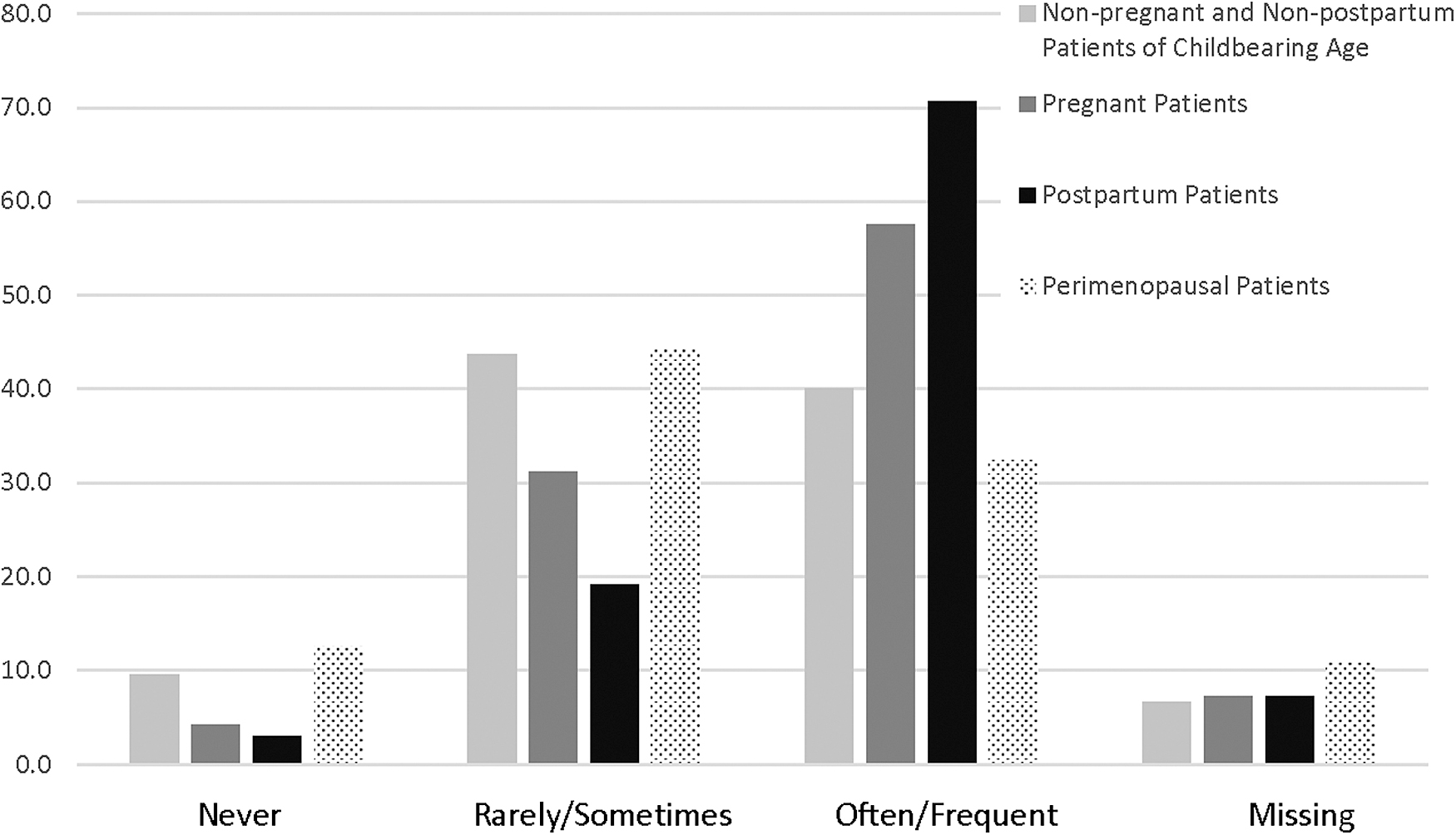
Reported clinical practice regarding screening for suicide ideation, intent, or behavior.
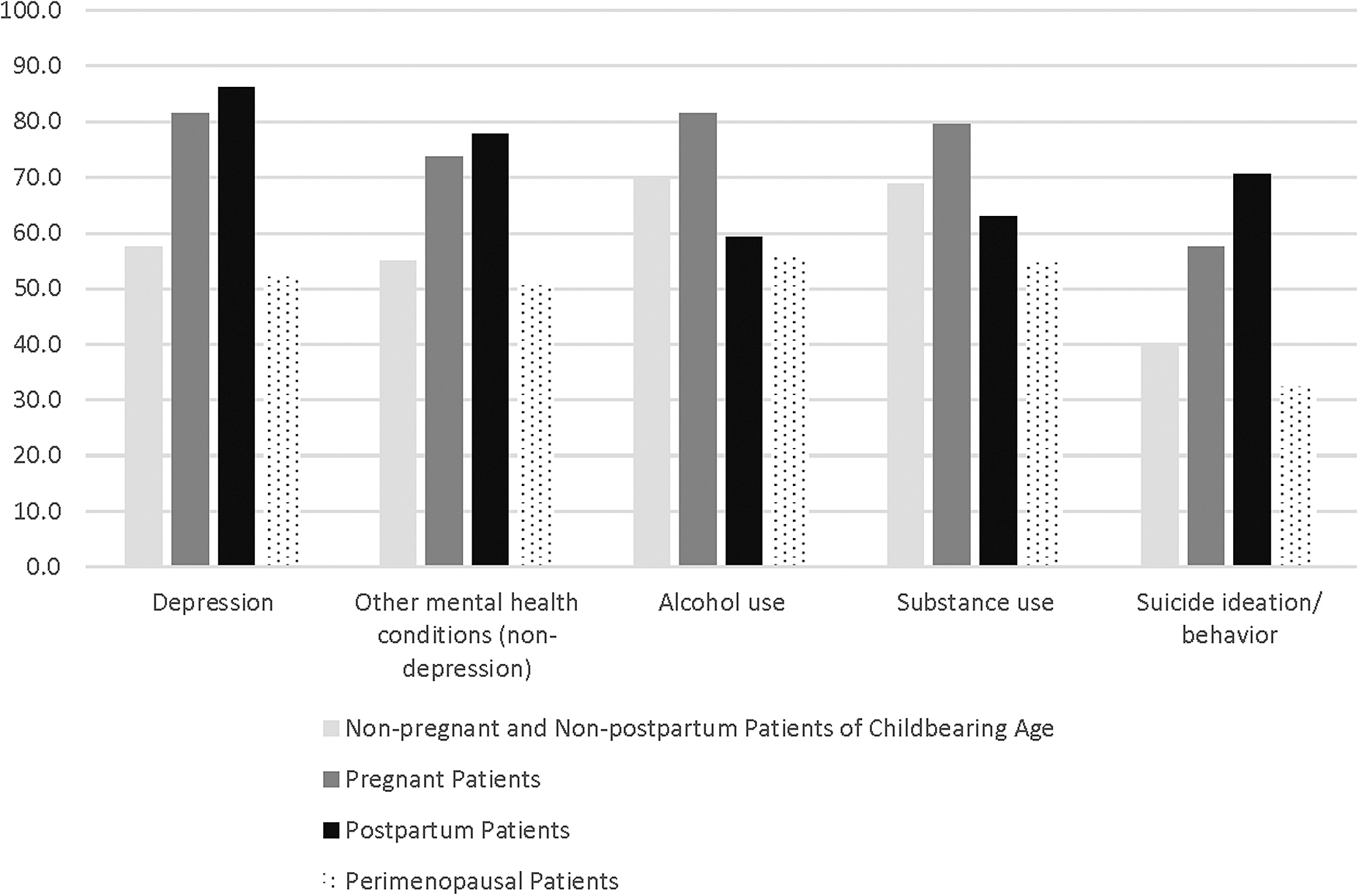
Percent of respondents who “often/frequently” screen for various conditions in different populations.
The most commonly reported tool used to screen for suicide risk was the Edinburgh Postnatal Depression Scale (EPDS 43 ) with 64.1% of providers reporting they “often” or “frequently” use it. About half of respondents often or frequently ask about personal history of suicide ideation or behavior (52.7%), and ask directly if a patient is having suicidal thoughts or plans (54.5%). Just over one-third (38.9%) often/frequently use the Patient Health Questionnaire-9 (PHQ-944), and few often/frequently use the Beck Depression Inventory-II (7.8%), 45 the SAD PERSONS scale 46 (0.6%), or the Columbia-Suicide Severity Rating Scale (C-SSRS) (0.6%). 47
The survey asked about clinical practice with subgroups of patients (nonpregnant/nonpostpartum patients of childbearing age, pregnant patients, postpartum patients, and perimenopausal patients) who are identified as at risk for suicide. Among all patient subgroups, the most common course of action by providers was making a referral to a mental health provider such as a psychologist or psychiatrist (range: 70.1% −88.0% often/frequently take this course of action depending on the patient population). This was followed by asking about suicide intent or plans (58.1%–79.6%), providing the patient a crisis call center number (range: 46.7%–57.5%), conducting safety planning (range: 38.3%–56.9%), prescribing psychotropic medication (range: 29.3%–47.9%), or discussing lethal means' safety (range: 28.7%–37.7%). Compared with nonpregnant/nonpostpartum women of childbearing age, providers were more likely to execute all the above interventions if patients were pregnant (all p < 0.05).
A majority of respondents (77.4%; n = 127) reported using telemedicine in their clinical practice. OB/GYN were largely neutral regarding the statement, “Telemedicine has increased my ability to assess patients for suicide risk,” with 60.3% neither agreeing nor disagreeing. Regarding the same statement, 6.8% strongly disagreed, 16.8% disagreed, 11.2% agreed, and only 5.0% strongly agreed.
Attitudes and beliefs
Respondents reported their beliefs about suicide and barriers that impede suicide risk assessment in their clinical practice. These responses are displayed in Tables 2 and 3.
Provider Beliefs and Attitudes Regarding Suicide
CE, continuing education.
Perceived Barriers to Suicide Screening
Knowledge
Less than half (43.5%) reported having taken any education hours in the past 12 months related to women's mental health (mean = 2.3 hours, standard deviation [SD] = 4.9 hours). About one-fifth (19.2%) had taken education hours specifically regarding suicide (mean = 0.62, SD = 2.03). Table 4 depicts the percent of providers who indicated that various factors are associated with increased suicide risk.
Percent of Providers Who Reported Various Factors Are Associated with Increased Suicide Risk
IPV, intimate partner violence.
Personal experience with suicide
About half of respondents (56.5%) reported personal experience with a family member or friend who died by suicide, and 16.2% reported they had a patient die by suicide. Twenty individuals had experience of both friend/family and patient suicide, resulting in 102 (61.1%) unique respondents with any personal experience with a death by suicide (patient, friend, family).
The medians of the Likert scores of screening frequency for nonpregnant/nonpostpartum women, postpartum, and perimenopausal women did not differ between providers who have personal or patient experience with suicide, compared with those without such experiences. Providers with personal or patient experience with suicide reported more frequently screening pregnant patients for depression (p = 0.04) and other mental health conditions (p = 0.02) compared with providers without personal/patient experience. With regard to the actions taken to address suicide risk, providers with and without personal/patient experience of suicide did not differ in frequency of interventions used for pregnant patients. OB/GYNs with personal/patient experience reported more frequent use of safety planning with postpartum patients (p = 0.01).
Conclusions
Suicide continues to be a leading cause of death in the United States, 1 and women's health care providers, such as OB/GYNs, are in a unique position to screen and mitigate suicide risk. 30,31 Reassuringly, most providers agreed that suicide screening is within their scope and believe there are steps they can take to prevent suicide. Although the majority of respondents endorsed screening pregnant and postpartum patients for suicide, there are still many who do not frequently screen these patients for suicide. Furthermore, the proportion of OB/GYNs conducting suicide screening for patients who are not pregnant or postpartum is low. Our results suggest that universal suicide risk screening is uncommon in OB/GYN settings. National organizations currently recommend screening targeted patient populations 48 or universal screening in specific settings. 49,50 Universal screening in OB/GYN settings may be of benefit to enable providers to detect hidden risk and prevent missed opportunities. 51 Expanding universal screening beyond acute or mental health settings should be considered. 52 –54
The most commonly endorsed suicide risk screening tool was the EPDS, 43 which is consistent with providers reporting commonly screening postpartum women for suicide. This study did not evaluate the underlying motivations to conduct screening in this group of patients specifically, although it is likely, in part, due to a renewed focus on maternal mortality, 55 –57 as well as policies and education about suicide risk in postpartum patients. 48 The existence of a brief and validated tool for use in postpartum samples, such as the EPDS, may also have promoted screening. Similar brief, self-reported, validated, and low-cost measures may be needed for other groups, or there may be a need for increased marketing, distribution, and awareness of existing screening tools. 58 Exploring the factors drive screening practices is an essential question for future research.
Brief and self-report tools may be more easily implemented than those suicide risk assessment tools that require clinician administration, given that a majority of respondents identified time constraints as a barrier to conducting risk assessment in their current practice. Asking patients directly about past and current suicide ideation and behavior may be a simple and low-burden method to initiate risk assessment and identify individuals who warrant further assessment or referral. In fact, the most common intervention when a patient is identified as potentially at risk is a referral to a mental health clinician; thus, OB/GYNs may be comfortable with a model of brief screening or asking about past and present suicide thoughts and behaviors and referring to more specialized services.
Referrals to mental health providers, however, may be impeded by limited mental health resources, particularly for women with public insurance. 59,60 Access to mental health resources was the most commonly identified barrier to suicide risk assessment in this and other studies, 40 and the ongoing shortage of mental health providers in the face of increasing demand for services has been labeled a public health crisis. 61 The very real difficulty in making referrals for patients who need mental health care for suicidality cannot be overemphasized. Thus, partnerships within communities, colocated mental health services, or integrated mental health clinicians may provide opportunities for growth in supporting women's access to mental health and suicide prevention resources.
In the absence of these resources, further training on lethal means' safety and safety planning with those at increased risk may enhance both the frequency and quality of these conversations, which are done by about one-third to one-half of respondents. Furthermore, resources, including gun locks or call center numbers, such as that National Suicide Prevention Lifeline (1-800-273-8255; will soon be available via “9-8-8”), 62 may be beneficial additions to OB/GYN practice.
Respondents were largely knowledgeable about suicide and suicide risk factors; however, knowledge gaps were present among this sample of OB/GYNs. Less than half correctly agreed that women are more likely to engage in suicide behaviors than men. Half neither agreed nor disagreed that rural suicide rates were higher than urban rates, which is the case. In fact, in 2018, the suicide rate for females in the most rural counties was 1.6 times greater than the rate in the most urban counties, 63 highlighting the need to consider geographic factors when assessing suicide risk for women. Furthermore, a majority disagreed that the most common means by which to die by suicide for women across all ages is firearms; however, in 2019, firearms were the most common means of suicide for women. 1 The prevalence of firearm use in suicide among women is critical information to disseminate, as it will allow for accurate and effective discussions of lethal means' safety, particularly in rural areas where the presence of gun store is associated with suicide rates. 64
Finally, few indicated that menopausal hormone replacement therapy may confer suicide risk. Research on menopausal hormonal therapy's impact on mental health and suicidality is mixed. While some studies suggest that hormone replacement therapy can improve mood among depressed women, this may only be true for perimenopausal and not postmenopausal women, 65 and one study recently reported that menopausal hormone therapy was associated with more than a two-fold increased risk of death by suicide, even after controlling for psychiatric diagnoses and psychiatric medications. 27 Further research on the association between menopausal hormone therapy and suicide risk is indicated.
Half reported inadequate mental health training was a barrier to suicide screening, and a majority reported their clinical practice would benefit from education hours related to women's mental health or suicide, yet fewer than half of respondents reported having participating in any training related to women's mental health in the past 12 months, and less than one in five had any training in suicide in women during that same period. It is unclear whether these trainings are not readily available or providers are not participating, but there is clearly a need for more training, and our survey participants indicated significant interest in these types of education. Medical schools and residency programs could consider adding women's mental health and suicide components to their training, and the evaluation of the current state of medical training and what is adequate training is a worthy future research endeavor. Professional organizations should offer, and health care organizations may consider mandating, continuing medical education on these important topics.
Of particular import is training on office-based interventions that can be performed by OB/GYNs, such as using the C-SSRS, 47 conducting safety planning, and discussing lethal means' safety. Adding these skills to OB/GYNs' repertoire will expand intervention options beyond the current common practice of referring to a specialist, which may take patients months to access.
Previous research has demonstrated that suicide screening may be more likely among providers who have had a suicidal patient. 37 Personal experience—through self, friend, or family—has also been shown to be associated with different mental health clinical practices among OB/GYNs. 66 –69 A majority of our sample had experience with suicide through the death of a family member, friend, and/or patient. While providers with personal or patient experience with suicide were more likely to frequently screen pregnant patients for depression and prescribe psychotropic medication for nonpregnant/nonpostpartum women, there were no statistically significant differences in screening or use of the other interventions to reduce suicide risk among other patient groups. Furthermore, there are still many knowledge and practice gaps identified, and it is not universally implemented.
This article is not without limitations. Most notably, this is a largely White female sample with personal experience of suicide death. There may be selection bias given that such a large proportion of respondents had personal experience with suicide; it is possible that individuals with personal experience were more likely to respond to the survey and their attitudes and clinical practice may not be representative of other providers. Beyond this, the sample was also from a group of individuals who have agreed to be surveyed and participate in research; it is possible that this group of OB/GYNs differ from other providers with regard to knowledge, clinical practice, or beliefs. The median age of 53 likely reflects practice patterns of clinicians who completed their training two decades ago, and may be less reflective of the education currently provided in medical schools and residency. Assessment of current medical school and residency training would be an important next step.
Studying only OB/GYN providers omitted other significant groups of women's health providers such as certified nurse midwives and other advanced practice providers, or Family Medicine providers, who may have different screening practices, and are an area for future research. Our study also did not investigate disparities in suicide screening by OB/GYNs, which is an important next step given that studies have demonstrated racial and ethnic disparities in identification of mental health problems and suicide risk. 70 –72 Finally, it is possible that respondents provided socially desirable answers; however, the anonymous nature of the survey was intended to mitigate these concerns.
Despite these limitations, this study fills a gap in the literature and is an important first step to understanding suicide prevention and informing education efforts among one group of women's health providers. Women's health providers have the opportunity to screen and identify those who may be at risk, and escalate appropriately and quickly to the appropriate resources. Women's health providers also have the opportunity to destigmatize suicidal ideation, identify women at increased risk, conduct lethal means' safety discussion, and connect patients to resources. Further educational opportunities, the creation and dissemination of brief screening tools, and distribution of resources such as gun locks and crisis line numbers are likely key to enhancing this aspect of women's health care and saving women's lives.
Implications for practice and/or policy
OB/GYNs are in a prime position to prevent suicide among women, as well as its many consequences for women, children, and families. Our study addresses the gap in the literature regarding OB/GYNs' knowledge, attitudes, and practice regarding suicide risk assessment and management. Those who influence the development of policies and clinical practice guidelines may consider the implementation of universal screening; however, our results indicate OB/GYNs would particularly benefit from clear policies encouraging suicide screening for women who are not pregnant and postpartum. Respondents indicated a need for additional training, and our study highlighted needs that continuing education credit hours could address.
Continuing education credit hours can include information regarding suicide behaviors specific to women over the course of the reproductive lifecycle, the greater frequency of and morbidity associated with women's self-directed violence, the significant morbidity that may accompany this, geographic (i.e., rural/urban) differences, and the role of firearms in women's suicide. Furthermore, specific training regarding discussion of patients' access to firearms in safety planning and lethal means' discussions may promote the distribution of gunlocks, where available, and enhance the effectiveness of these prevention efforts, ultimately saving lives.
Footnotes
Authors' Contributions
All persons who meet authorship criteria are listed as authors, and all authors certify that they have participated sufficiently in the work to take public responsibility for the content, including participation in the concept, design, analysis, writing, or revision of the article. Furthermore, each author certifies that this material or similar material has not been and will not be submitted to or published in any other publication.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This work was supported by the Health Resources and Services Administration [Grant UA6MC3160].