
Abstract
Objective:
Little is known about women's confidence in their breast cancer screening. We sought to characterize breast cancer screening confidence by imaging modality and clinically assessed breast density.
Materials and Methods:
We undertook a cross-sectional survey of women ages 40–74 years who received digital mammography (DM), digital breast tomosynthesis (DBT), and/or breast magnetic resonance imaging (MRI) with a normal screening exam in the prior year. The main outcome was women's confidence (Very, Somewhat, A little, Not at all) in their breast cancer screening detecting any cancer. Multivariable logistic regression identified correlates of being very confident in breast cancer screening by screening modality group: Group 1) DM vs. DBT and Group 2) DM or DBT alone vs. with supplemental MRI.
Results:
Overall, 2329 of 7439 (31.3%) invitees participated, with 30%–61% being very confident in their screening across modality and density subgroups. Having dense versus nondense breasts was associated with lower odds of being very confident (Group 1: odds ratio [OR]: 0.58; 95% confidence interval [CI]: 0.46–0.79; Group 2: OR: 0.56; 95% CI: 0.40–0.79). There were no differences by modality within Group 1, but for Group 2, women undergoing MRI had higher odds of being very confident (OR: 1.69; 95% CI: 1.21–2.37). Other correlates of greater screening confidence were as follows: Group 1—being offered a screening test choice and cost not influencing modality received, and Group 2—decision satisfaction and worry.
Conclusions:
Women with dense breasts had lower screening confidence regardless of screening modality and those undergoing MRI had higher confidence regardless of density. The importance of informing women about screening options is underscored by observed associations between screening choice, decision satisfaction, and screening confidence.
Introduction
Breast density reporting laws have been enacted in most states in the United States and a pending Food and Drug Administration rule will require reporting of breast density nationally. 1,2 While details of the breast density reporting regulations are not yet known, implementing national reporting may prompt women with mammographically dense breasts to question what screening strategy can best detect early-stage breast cancer in their breasts.
Currently, the United States has neither a national breast cancer screening program nor national breast density reporting regulations in place. In the absence of a national program, breast cancer screening in the United States is largely guided by primary care clinicians who rely on clinical practice guidelines from a number of groups including the US Preventive Services Task Force (USPSTF), the American Cancer Society, the American College of Radiology and Society for Breast Imaging. 3 –5 USPSTF recommends that average-risk women initiate breast cancer screening with mammography at age 50 years and that they screen every 2 years; women are encouraged to engage in shared decision-making with their health care providers to decide if they should initiate screening earlier than age 50. 5 Other guidelines recommend earlier screening initiation and annual screening—either ongoing or for at least several years. 3,4
Breast density legislation is implemented at the state level with substantial variation in the laws from state to state. 6 Some states require notification to only women with dense breasts, whereas others require that all women be notified of their density. Likewise, some states mandate that insurance reimburse for supplemental imaging, while others do not. Thus, an individual's experience of having dense breasts in the United States currently varies based on where they live. 7,8
US women are generally enthusiastic about the effectiveness of breast cancer screening. 9 However, increased breast density awareness, particularly among individuals with mammographically dense breasts, could undermine their confidence in breast cancer screening. An evidence review undertaken in June of 2018 reported an increase in use of supplemental imaging following implementation of breast density notification. 10 However, a more recent systematic review (through June 2020) highlighted the key role for health care providers in guiding consideration of supplemental imaging and reported a great deal of variation regarding how breast density information affected women's cognitive, psychological, and behavioral outcomes. 11
To further the understanding of women's thoughts on screening, we undertook a study to assess women's confidence in different breast cancer screening modalities taking into account breast density. We hypothesized that individuals undergoing screening with digital breast tomosynthesis (DBT) compared with digital mammography (DM) alone and those undergoing supplemental magnetic resonance imaging (MRI) compared with mammography alone would have greater confidence that their breast cancer screening will find any cancer that is in their breasts. Furthermore, we hypothesized that women with dense breasts would have lower confidence in their breast cancer screening than women with nondense breasts. We designed our study to focus on women's clinical breast density rather than on perceived breast density because when pending breast density notification is implemented in the United States it will be based on clinical density.
Methods
Study design
We undertook a cross-sectional survey through six Breast Cancer Surveillance Consortium (BCSC) 12 registries to assess women's confidence in their recent breast cancer screening. The survey was designed to understand women's most recent breast cancer screening experiences and to compare responses by modality and clinically assessed breast density. There were two modality-specific comparator groups: Group 1: DM versus DBT and Group 2: either DM or DBT (i.e., mammography alone) versus DM or DBT with screening MRI.
Setting
Surveys were conducted between December 2017 and January 2020 through six BCSC registries in five states.
Study population
We sampled women aged 40–74 years who had undergone breast cancer screening with a negative assessment (Breast Imaging-Reporting and Data System [BI-RADS] initial assessment 13 of 1 or 2) within the prior year from the Carolina Mammography Registry, New Hampshire Mammography Network, Kaiser Permanente Washington Registry, Sacramento Area Breast Imaging Registry, San Francisco Mammography Registry, and Vermont Breast Cancer Surveillance System. Women with a personal history of breast cancer or without a known BI-RADS breast density 13 within the prior 5 years were ineligible. To enhance representation and control for potential confounding, eligible women were further selected for invitation within each registry using frequency matching within groups. For Group 1, frequency matching used strata defined by breast density (dense and nondense), age (40–49, 50–65, and 65–74 years), and race/ethnicity (American Indian/Alaska Native, Asian/Native Hawaiian or other Pacific Islander, black or African American, Hispanic, white, other/unknown) with strata defined by registry-specific sample distributions.
For Group 2, all women undergoing screening MRI were invited and invitations to women who underwent mammography alone (DM or DBT) were frequency matched by age, density (4 BI-RADS categories), first degree family history (yes, no, missing), self-reported biopsy history (yes, no, missing), and time since prior mammogram (first, 9–32 months, 32 or more months, missing).
Invitations for survey participation were sent by each BCSC registry by mail. Incentives included a $2 bill in the invitation letter (used by five of the six registries) and/or a chance to win a $100 gift card (one winner per registry). 14 Participants accessed the online survey through an internet link using a unique identifier and access code included in the invitation; paper surveys were provided for invitees who requested them or were included with the initial invitation for invitees in locations where internet accessibility was known to be limited. Up to three reminder postcards were sent to nonresponders. Each registry received local institutional review board approval. 14
Data sources/survey
Following a series of focus groups, we developed and prioritized survey content with input from both patient partners and a patient advisory board. 15 Survey items are briefly described (see Supplementary Appendix for details).
Participant characteristics
We collected sociodemographic characteristics, health status, and breast cancer risk factors, which allowed the BCSC 5-year breast cancer risk to be estimated. 16 Participants reported their perceived breast cancer risk, screening frequency, attitudes, and cancer worry using the Lerman Cancer Worry Scale. 17
Screening confidence
Participants' overall confidence in their own breast cancer screening was assessed as follows: “Overall, how confident are you that your breast cancer screening will find breast cancer if you have cancer in your breasts?” (very confident, somewhat confident, a little confident, not at all confident). A high level of confidence was defined as those who reported being “very confident” in their screening. To assess modality-specific screening confidence, we asked about agreement with the following statement for mammography, ultrasound, and breast MRI separately: “I feel confident that if I have breast cancer, [specific modality] will find it.”
Screening decision-making
Participants were asked if they had a choice about which screening test(s) they received at their most recent screening. Those who affirmed having a choice indicated the modalities offered. Everyone was asked how much out-of-pocket costs for the screening tests influenced the type of test(s) they received. Everyone was also asked to think back to their last breast cancer screen and to indicate their level of agreement with several statements regarding sources of screening information. To assess breast cancer screening decision-making, we used the Satisfaction With Decision scale (SWD), 18 which ranges from 1 (lowest satisfaction) to 5 (highest satisfaction) based on scored agreement across six items.
Statistical analyses
Analyses were undertaken separately for each comparator group (Group 1: DM vs. DBT and Group 2: DM or DBT alone vs. supplemental MRI). To address potential selection bias associated with survey response, we compared the characteristics of survey responders versus nonresponders. We used logistic regression to estimate stabilized propensity scores 19 for the probability of survey response within each comparator group. All other analyses incorporated inverse probability weights from the stabilized propensity scores to balance characteristics between responders versus nonresponders. We compared participant characteristics and survey outcomes by modality and by BI-RADS breast density as recorded at the most recent screening examination (nondense = a:fatty or b:scattered density, dense = c:heterogeneously dense or d:extremely dense). 20 We used chi square tests for categorical variables and t-tests for continuous variables.
We used multivariable logistic regression to identify correlates of high screening confidence (1 = very confident vs. all other responses), adjusting for frequency-matched confounders. All models included interactions with breast density to test for effect modification. Model selection used the stepwise method as implemented in SAS Release 9.4 (SAS Institute, Cary, NC, USA), which sequentially entered the most significant variable with p < 0.10 and then after each entered variable, removed variables that did not maintain significance at p < 0.05. Density, screening modality, and BCSC 5-year risk were forced in the model.
Results
A total of 2329/7439 (31.3%) women participated (Group 1: 1528/5408 = 28.2%: Group 2: 801/2031 = 39.4%). For both groups, participants differed from nonparticipants by age, registry, and race, but did not differ by breast density (see Supplementary Table S1). Overall, 87.3% completed the surveys online, and the remainder completed paper surveys.
Participant characteristics
Several differences in participant characteristics by modality remained with density strata after weighting (Table 1). For example, for Group 1, women who received DM versus DBT were more likely to be older and on Medicare. BCSC 5-year risk did not differ by modality within density categories for Group 1 or Group 2. However, risk perceptions did differ for both groups. Those who underwent MRI more frequently reported being at a higher-than-average risk of breast cancer than women who had mammography alone. Most participants (68%–100%) reported undergoing screening annually, but screening frequency differed by modality regardless of density. Women who received DBT versus DM or MRI versus mammography alone tended to be screened more frequently.
Participant's Characteristics by Comparator Group, Density, and Modality
Percentages reflect weighting to adjust for respondent characteristics.
Mammography is DM or DBT alone; breast MRI includes women who also had DM or DBT.BCSC, Breast Cancer Surveillance Consortium; DBT, digital breast tomosynthesis; DM, digital mammography; MRI, magnetic resonance imaging.
Many participants (41%–73%) reported having a prior abnormal mammogram that required additional breast imaging (Table 2). There were no significant differences in this experience by modality for women with nondense breasts. For Group 1 and Group 2 women with dense breasts, a prior abnormal mammogram experience was more common for those who most recently had a DBT in Group 1 (DBT 57% vs. DM 48%, p = 0.014) or who underwent MRI in Group 2 (MRI 90% vs. mammography 84%, p = 0.086).
Screening Experiences and Perceptions by Comparator Group, Density, and Modality +
Mammography is DM or DBT alone; Breast MRI includes women who also had DM or DBT.
SD, standard deviation.
Percents reflect weighting to adjust for respondent characteristics.
Most participants (>80%) responded that “Finding breast cancer early saves lives” either all or most of the time (Table 2) and that “Finding breast cancer early means less treatment.” Fewer participants (∼20%) reported hearing of slow growing cancers that might not cause a problem, yet the vast majority (over 78%) indicated they would want testing for such a slow-growing cancer.
Being very confident in breast cancer screening did not vary by modality for Group 1, but did vary by density (dense; 31%–34% very confident vs. nondense; 45%–46% very confident) (Table 2). For Group 2, the percent of participants who strongly agreed that regular screening was important and who reported being very confident in their screening was significantly higher for those who underwent MRI versus mammography alone regardless of density. Despite higher confidence in their screening, Group 2 women who underwent MRI reported greater breast cancer worry.
When modality-specific confidence was addressed, differences by screening modality received were only observed for Group 2 and MRI-specific confidence. Hence, Figure 1 depicts agreement with modality-specific confidence by density alone for mammography, ultrasound, and MRI (Group 1). Participants with nondense breasts tended to express greater confidence in screening than those with dense breasts and confidence in ultrasound tended to be lower than for mammography or MRI, but these differences were not statistically significant. Among Group 2 participants, significantly stronger confidence in MRI was noted for those who underwent MRI regardless of density than for those who underwent mammography alone.
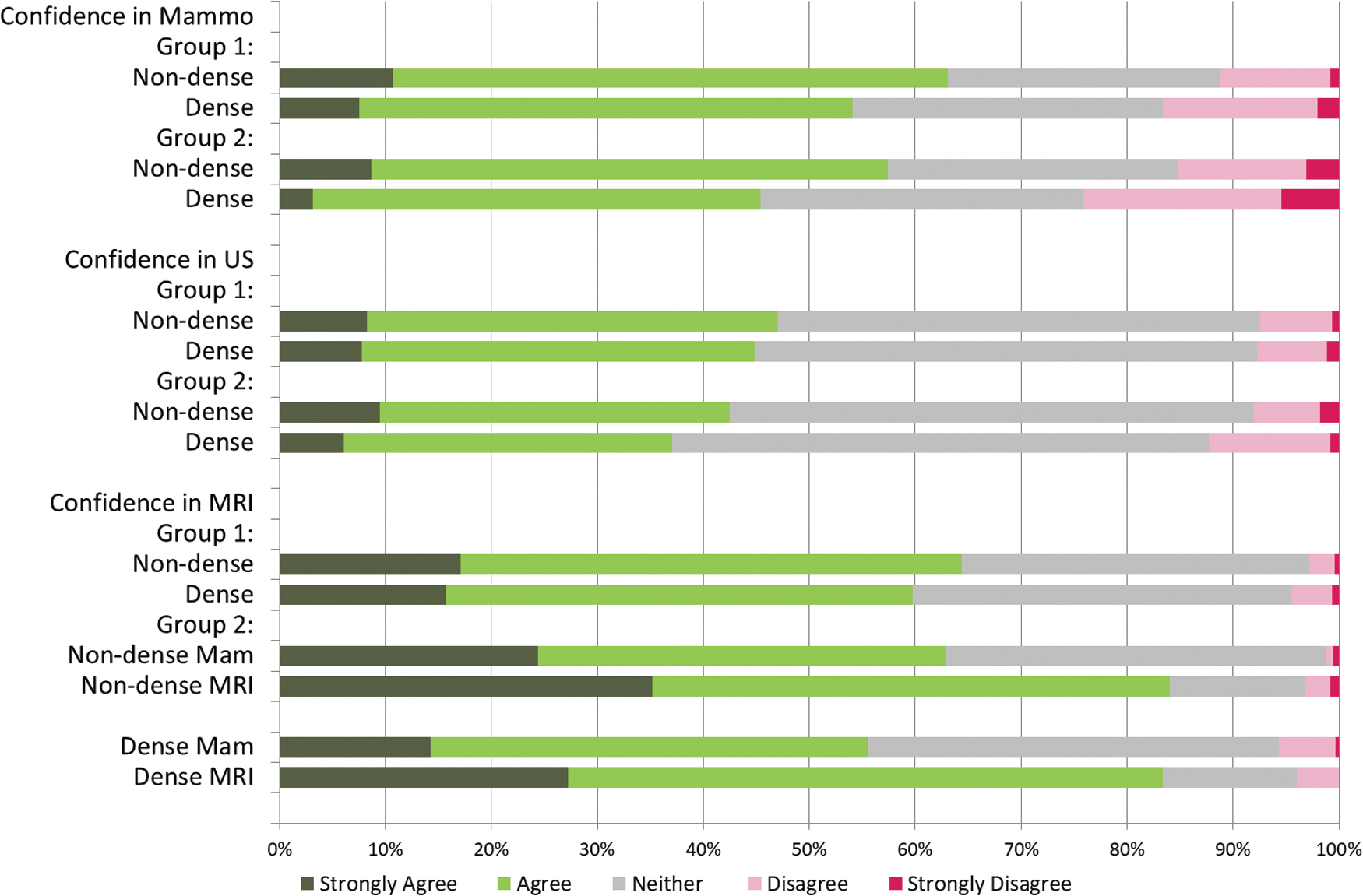
Agreement with modality-specific confidence that breast cancer will be found by group and density.
Screening modality decision-making
Between 21% and 56% of individuals reported having a choice of screening test (Table 3). Within each group, those who underwent DBT (vs. DM), or supplemental MRI (vs. mammography alone) more frequently reported having had a screening test choice. Few individuals (2%–11%) reported having their screening test choice influenced by out-of-pocket costs (Table 3). For Group 1, those undergoing DM alone were more likely to report cost being an influence versus those undergoing DBT (nondense: DM 8% vs. 4% DBT, p = 0.021; dense: DM 11% vs. DBT 6%, p = 0.012). For Group 2, out-of-pocket costs were not a significant factor.
Screening Decision Making and Perceptions of Information Provided by Comparator Group, Density, and Modality +
Mammography is DM or DBT alone; breast MRI includes women who also had DM or DBT.
SD, standard deviation.
Percents reflect weighting to adjust for respondent characteristics.
Agreement that health care providers fully explained the screening tests available to them differed by modality only for those with dense breasts in Group 1. In contrast, for Group 2, there were no differences by density, but there were marked differences by modality with those undergoing supplemental MRI reporting much higher agreement that screening tests available were fully explained (Strongly agree/Agree: nondense: mammography 20% vs. MRI 67%; dense: mammography 25% vs. MRI 69%). While most (>75%) agreed that their health care providers spoke about how often they should be screened, the percent who agreed that their provider explained both potential harms and benefits was much lower (26%–33% for Group 1 and 24%–57% for Group 2).
Satisfaction with decision scores was comparable in Group 1 across modalities and density (Table 3). In contrast, for Group 2, these scores where higher for those undergoing MRI versus mammography alone regardless of breast density (means satisfaction with decision score: nondense: mammography 3.8 vs. MRI 4.5, p < 0.0001; dense: mammography 3.8 vs. MRI 4.3, p < 0.0001).
Correlates of screening confidence
Correlates of being very confident in their breast cancer screening differed between comparator groups (Table 4). For Group 1, being offered a choice of screening tests was associated with higher odds of being very confident (adjusted odds ratio [OR]: 1.3, 95% confidence interval [CI]: 1.02–1.67); whereas cost having an influence on the screening test was associated with lower odds of being very confident (adjusted OR: 0.57, 95% CI: 0.46–0.74). Similarly, having dense breasts was associated with lower odds of being very confident (adjusted OR: 0.58, 95% CI: 0.46–0.74). However, there were no significant differences by modality and interactions between modality and density were not statistically significant.
Odds Ratios and Confidence Intervals for Women Being Very Confident In Their Breast Cancer Screening
CI, confidence interval; OR, odds ratio.
For Group 2, while being offered a choice of tests and costs influencing screening test were correlates in unadjusted analyses, they were not significant in adjusted analyses (Table 4). Density was associated with lower odds of screening confidence (adjusted OR: 0.56, 95% CI: 0.4–0.79), while undergoing screening MRI was associated with higher odds of screening confidence (adjusted OR: 1.69, 95% CI: 1.21–2.37). Interactions between density and modality were not statistically significant.
For both Groups 1 and 2, lower cancer worry was associated with higher odds of screening confidence as was higher satisfaction with decision-making. Adjusted ORs associated with these factors were of similar magnitude across the groups.
Discussion
Our survey showed that women with dense breasts had lower screening confidence than women with nondense breasts regardless of the screening modality they underwent. These findings have important implications for health care providers who must consider how best to counsel women on breast cancer screening as breast density reporting regulations are slated to be enacted nationally in the United States. 1,2 With these regulations, the need for decision support tools is expected to increase, prompted by a greater desire for information about breast cancer screening options, particularly among women with dense breasts. While many decision aids address mammography initiation and frequency, very few address screening for women with dense breasts. 21,22
Despite the growing recognition that supplemental screening to augment mammography is an appropriate consideration among women at high risk of mammography screening failure, 23 current clinical guidelines do not address supplemental screening and there is a general lack of decision support for counseling women who may be at high risk of screening failures. 5,22 Indeed, our qualitative work in preparation for the survey underscored how much confusion women have regarding breast density. 15 Thus, counseling women with dense breasts on screening options may be difficult.
Regardless of breast density, we found that women who underwent screening breast MRI reported higher screening confidence than did frequency-matched women who underwent mammography alone. Although there is growing interest in use of breast MRI among women with dense breasts, particularly with the advent of abbreviated MRI and recently published screening studies from Europe and the United States, 24 –26 screening breast MRI is not recommended in average-risk women. Currently, only a subset of women at elevated lifetime risk, prior chest radiation, and mutation carriers are recommended for screening breast MRI. 5 However, recent legislation in Pennsylvania requires insurance coverage for breast MRI among women with extremely dense breasts. 27
Our evaluation of factors associated with screening confidence revealed that individuals who had a choice of screening tests or for whom cost was not a factor in their test choice were more likely to report being very confident in their breast cancer screening. Yet, our survey highlighted that only 20%–32% of individuals undergoing mammography alone agreed that their health care provider fully explained the different types of screening tests available to them. Regardless of whether health care providers remain up-to-date on screening options provided at local radiology facilities, discussion of screening benefits and harms is warranted. However, only 26%–33% who underwent DM or DBT alone agreed that their providers explained both the potential harms and benefits of breast cancer screening. Despite this, more than 75% of participants agreed that their health care provider discussed how often they should be screened, which may also entail consideration of benefits and harms. The fact that screening frequency was more commonly discussed than screening harms and benefits may reflect the breast cancer screening guidelines of the last two decades, which have focused mostly on frequency and when to initiate screening. 28
Lastly, our finding of lower screening confidence among individuals who reported that cost influenced their screening underscores how financial barriers that hamper equitable access to screening modalities may undermine screening. We previously documented differential access to DBT early in its dissemination. 29 While only a small fraction (2%–11%) reported out-of-pocket costs having an influence in the screening test they received, the fact that these percentages were higher among those in Group 1 who underwent DM rather than DBT suggests that participants may have elected to undergo DM due to the higher cost of accessing DBT.
Our study has both strengths and limitations. First, our analysis focused on BI-RADS density at the last screening examination rather than on women's perceived breast density. We view this as a strength because BI-RADS density will be the basis for pending national notification and a separate report from this survey addressed the accuracy of women's breast density knowledge. 8 Second, participation in our survey was likely influenced by concerns about breast cancer. While our analyses used statistical adjustments for survey participation, some differences remained. We found that women who underwent DBT in Group 1 or MRI in Group 2 tended to have higher cancer worry. Third, we report on participants' confidence in their breast cancer screening, but do not know how this will translate into future actual screening behaviors. Finally, our findings are specific to breast cancer screening as practiced in the United States. US screening practices differ substantially from those in Europe where formal breast cancer screening programs have been implemented. 30,31
Conclusions
Our survey adds to the body of research showing that breast density affects women's perceptions of breast cancer screening and underscores that there is room for improving communication and decision support around breast cancer screening, particularly for women with dense breasts. Observed associations between screening choice, decision satisfaction, and screening confidence highlight the importance of informing women regarding breast cancer screening options. Accessible information and tools that support health care providers and individual women in discussions of breast cancer screening and breast density are needed.
Footnotes
Acknowledgments
We thank the participating women, mammography facilities, and radiologists for the data they have provided for this study. You can learn more about the BCSC at:
Authors' Contributions
All authors contributed to the conception or design of the work; or the acquisition, analysis, or interpretation of data; drafting or revising the work critically; final approval of the version for submission; all have agreed to be accountable for all aspects of the work.
Disclaimer
All statements in this report, including its findings and conclusions, are solely those of the authors and do not necessarily represent the views of the Patient-Centered Outcomes Research Institute (PCORI), its Board of Governors or Methodology Committee, nor those of the National Cancer Institute or the National Institutes of Health.
Author Disclosure Statement
Dr. Kerlikowske reports being a nonpaid consultant for GRAIL for STRIVE study. Dr. Miglioretti reports royalties from Elsevier. Dr. Buist reports honorarium for her position on the Data Safety and Monitoring Board for WISDOM Study. The authors declare no other conflicts of interest.
Funding Information
Research reported in this work was funded through a Patient-Centered Outcomes Research Institute (PCORI) Program Award (PCS-1504-30370). Data collection for this research was additionally supported by the Breast Cancer Surveillance Consortium (BCSC) with funding from the National Cancer Institute (P01CA154292, U54CA163303), the UC Davis Clinical and Translational Science Center, the UC Davis Comprehensive Cancer Center, and the Placer County Breast Cancer Foundation. The collection of cancer and vital status data for BCSC registries was supported, in part, by several state public health departments and cancer registries throughout the United States. For a full description of these sources, please see:
Supplementary Material
Supplementary Table S1
Supplementary Appendix
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.