
Abstract
Women and girls with bleeding disorders experience abnormal and excessive bleeding that can negatively impact their overall health and quality of life. In this report, we provide an overview of the biology, types, clinical care, and state of the science related to bleeding disorders in girls and women and describe Centers for Disease Control and Prevention (CDC) activities related to (1) surveillance of bleeding disorders in women; (2) scientific review, research, and collaboration to inform health care gaps in identifying and caring for women with bleeding disorders; and (3) development of health promotion and education programs to bring awareness about bleeding disorders to both women and girls in the population at large and various health care providers who care for women. Findings generated from surveillance and research activities inform the development of new public health programs aimed at improving diagnostic and health care services and empowering women with bleeding disorders with the knowledge they need to navigate a complex health care system with the need for specialty care services. Additional work is needed to improve provider awareness and understanding of the unique needs of women and girls with bleeding disorders to achieve appropriate care and treatment and ensure optimal outcomes and quality of life.
Introduction
Inherited bleeding disorders such as von Willebrand disease (VWD), hemophilia, rare clotting factor deficiencies, and platelet disorders affect up to 1% of females in the United States. 1 While inherited bleeding disorders affect both males and females, these conditions pose unique problems for women and girls because of the impact they can have on their reproductive health. Menarche is typically the first major hemostatic challenge. It is estimated that one in five females experience heavy menstrual bleeding (HMB), 2 –4 and among those, up to 24% have a bleeding disorder. 5 Other symptoms that may present in childhood include epistaxis, gum bleeding, easy bruising, and excessive bleeding after surgical or dental procedures. 6
Rarely, joint or muscle bleeding with risk of subsequent mobility impairment or intracranial hemorrhage can occur. During pregnancy and delivery, women with bleeding disorders have a 10 times higher maternal mortality rate 7 and significantly higher incidence of postpartum hemorrhage. 7 Women with VWD are significantly more likely to undergo hysterectomy at an early age due to HMB 8 and to experience hemorrhagic ovarian cysts, endometriosis, endometrial hyperplasia, and polyps. 9,10 The impact is not only physical; bleeding disorders among women have been reported to reduce quality of life, impair routine activities, and result in negative psychosocial outcomes. 4,11,12
In this report, we provide an overview of the state of the science and describe Centers for Disease Control and Prevention (CDC) activities related to (1) surveillance of bleeding disorders in women; (2) scientific review and collaboration to inform health care gaps in identifying and caring for women with bleeding disorders; and (3) development of health promotion and education programs to bring awareness about bleeding disorders to both women and girls in the population at large and various health care providers who care for women. We conclude by discussing remaining gaps and future directions to improve the identification and care of women with bleeding disorders such that excessive bleeding and concomitant long-term sequelae are prevented or minimized and women with bleeding disorders lead full and healthy lives.
Overview of Hemostasis and Inherited Bleeding Disorders in Women
Hemostasis and disorders
A variety of plasma proteins and cellular structures control the process of hemostasis, from the initial formation of a platelet plug at the site of vessel injury to the establishment of a firm fibrin clot to seal the breech, followed by the process of fibrinolysis to break down the clot when it is no longer needed (Fig. 1). Defects in the pathway may be inherited as single-gene disorders and can cause excessive bleeding. These bleeding disorders may be divided into VWD, platelet disorders, coagulation factor deficiencies, fibrinolytic defects, and connective tissue disorders (Table 1). All these disorders may cause excessive bleeding with injury, surgery, and pregnancy delivery; most will lead to HMB in females, which is often the presenting symptom. 13

The blood coagulation mechanism. Each asterisk represents a component known to be deficient or defective in one or more inherited bleeding disorders.
Characteristics of Inherited Bleeding Disorders Affecting Women and Girls
α2-AP, α-2-Antiplasmin; AD, autosomal dominant; AR, autosomal recessive; PAI-1, plasminogen activator inhibitor-1; XR, X-linked recessive.
Disorders of primary hemostasis include VWD and platelet disorders; these disorders impair the formation of the initial platelet plug and cause excessive bleeding from the skin, mucous membranes, and uterus. VWD is caused by a deficiency or defect of von Willebrand factor (VWF), a plasma protein required for normal platelet function and maintenance of normal levels of clotting factor VIII. There are three major subtypes of VWD. Type 1 VWD, the most frequent form, is characterized by a deficiency of VWF; type 2 is characterized by a functional defect in VWF; and type 3, the rarest and most severe form, is characterized by no or very low levels of VWF production.
Types 1 and 2 VWD affect both men and women over multiple generations due to their autosomal dominant inheritance patterns. Females account for a disproportionately high number of patients seen for treatment for VWD because of the challenges they face due to HMB. Platelet disorders may affect platelet number (thrombocytopenia) or platelet function, or both. Diagnosis of platelet function defects is challenging as the necessary laboratory tests are not widely available. 14
Disorders of secondary hemostasis include hemophilia and other factor deficiency disorders; these disorders affect the formation of the fibrin clot and may cause mucocutaneous and soft tissue bleeding, as well as bleeding from invasive procedures. Hemophilia includes hemophilia A (classic hemophilia, deficiency of clotting factor VIII) and hemophilia B (Christmas disease, deficiency of clotting factor IX). Both types of hemophilia have an X-linked inheritance pattern and thus primarily affect males. However, recent data show that close to one in five patients with mild hemophilia are female. 15
These girls and women may be overlooked because their male relatives are often more severely affected. Nonetheless, even women with hemophilia who have only mildly low levels of circulating clotting factor have been found to have increased risk for traumatic joint bleeding, bleeding after tooth extraction or surgery, and anemia attributed to menstrual blood loss. 16 Moreover, certain women with hemophilia may be severely affected, producing very little clotting factor and significant bleeding because of the X chromosome inactivation pattern established during the embryonic period. 17
Most clotting factor deficiencies, other than hemophilia and VWD, show autosomal recessive inheritance, requiring that both parents have a defect in the same gene and are, thus, very rare in the population-at-large. These disorders are more common in areas with consanguineous matings. 18 Exceptions are factor XI deficiency, seen more often in those of Ashkenazi Jewish ancestry, and some fibrinogen defects, which may be autosomal dominant. 19
Fibrinolysis is the breakdown of the clot when it is no longer needed. In fibrinolytic defects, the clot forms but breaks down too rapidly, leading to delayed bleeding. Fibrinolytic disorders may lead to increased risk of fetal loss or premature delivery. Fibrinolytic disorders are not detectable with routine tests. 20
Finally, connective tissue disorders involving collagen, usually forms of Ehlers–Danlos syndrome, may also lead to excessive bleeding due to blood vessel fragility and poor reactivity of subendothelial collagen with platelets and VWF. They may also affect placenta formation and stability. 21
Clinical care
Women and girls with all types of bleeding disorders require individualized treatment based on their diagnosed type and subtype of disorder, severity, bleeding phenotype, and clinical context. In addition to the bleeding symptoms recognized in males, females have specific reproductive system bleeding often requiring different approaches. Treatment is a constant balance to prevent bleeding but not overtreat and cause a potential life-threatening venous thromboembolism.
Treatment products include desmopressin, antifibrinolytics, plasma-derived and recombinant factor concentrates, blood products, and hormonal birth control. Treatment can be given prophylactically to prevent bleeding episodes or episodically to treat bleeding episodes when they occur. For some rare disorders, specific treatment products are not available and only fresh frozen plasma or cryoprecipitate can be used. 18
It is important that women with bleeding disorders be cared for at specialized treatment centers by those knowledgeable about the treatment options available. Females diagnosed with a bleeding disorder should have appropriate access to comprehensive care including the following: expertise in bleeding disorders, multidisciplinary clinics including obstetrician–gynecologists (OB-GYNs) for HMB and other gynecologic conditions, genetic testing for diagnostic purposes and family planning, and availability of appropriate treatment products. 22 Affected women should receive preconceptual counseling on their risk of transmitting their specific bleeding disorder.
Coordination of care between hematology and obstetrics is needed for safe delivery of potentially affected infants, who may have cephalohematoma or intracranial hemorrhage, particularly if instruments are used to facilitate delivery.
Clinical management of females with bleeding disorders remains challenging, as there is wide variability in individual patient bleeding phenotypes, clinical practice by providers, and a lack of evidence basis to guide provider decision-making. In 2021, new international guidelines for diagnosis and management of VWD in males and females were published through collaboration of both clinical and community-based organizations from the U.S. and worldwide 1,23 with the goal of supporting patients, hematology and non-hematology clinicians, and health care professionals during the VWD diagnostic process and disorder management.
Updated international guidelines for the management of hemophilia were published in 2020 and include consensus-based recommendations for the identification and management of female genetic carriers of hemophilia with and without bleeding symptoms. 24 Although the recent guidelines for hemophilia and VWD are based on limited studies and evidence, they provide practical recommendations and address specific challenges faced by women with bleeding disorders. There are currently no U.S. or international guidelines for specific treatment of women with other bleeding disorders, although recent reviews address treatment of clotting factor deficiencies, 18 platelet function disorders, 10,25 and fibrinolytic defects. 20
CDC Surveillance Program for Bleeding Disorders
Overview
Since 1998, CDC has supported ongoing surveillance of persons with diagnosed bleeding disorders who receive care at federally supported hemophilia treatment centers (HTCs) across the U.S. This clinical network currently includes 145 HTCs.
In 1998, CDC, in collaboration with the U.S. Hemophilia Treatment Center Network (USHTCN) and the member HTCs, established its first bleeding disorders surveillance program, the Universal Data Collection (UDC) system, with the goals of (1) monitoring human immunodeficiency virus (HIV) and bloodborne viral hepatitis in persons with hemophilia and (2) tracking the prevalence of and trends in complications associated with hemophilia and other bleeding disorders. In response to a marked increase in the proportion of women receiving care in HTCs during the 1990s and 2000s, 26 CDC developed a supplemental UDC module in 2009 to collect female-specific data, including menstrual bleeding and reproductive outcomes. 27
In 2012, CDC, in collaboration with the American Thrombosis and Hemostasis Network (ATHN) and the USHTCN, developed and launched the next iteration of the surveillance system, known as the Community Counts Public Health Surveillance of Bleeding Disorders project (Community Counts). 28 Community Counts expanded data collection to include more in-depth tracking of complications associated with bleeding disorders and other health indices (e.g., chronic health conditions and health care utilization) in persons living with a bleeding disorder. This expanded data collection included some female-specific outcomes, such as use of prophylaxis treatment for menstrual bleeding and history of a hysterectomy.
The current Community Counts surveillance program includes three components: (1) the HTC Population Profile, which collects basic information on the entire population of persons with bleeding disorders who received care at any HTC during each year; (2) the Registry for Bleeding Disorders Surveillance (the Registry), which includes more in-depth data collection on a subset of patients at each HTC who agree to participate in the Registry; and (3) the Mortality Reporting component, in which HTCs submit data on the characteristics of decedents and causes of death. The history of the CDC bleeding disorders surveillance program has been recently reviewed. 29
Prevalence and epidemiology of bleeding disorders in women
Since CDC first launched Community Counts, the number of females being treated at HTCs has increased markedly. Data from the Community Counts HTC Population Profile indicate an 47.3% increase in females with bleeding disorders in 9 years, from 6,169 in 2012 to 9,088 females in 2020; moreover, the proportion of persons receiving care for bleeding disorders who were female increased 17% from 28.8% female in 2012 to 33.6% female in 2020 (Fig. 2).
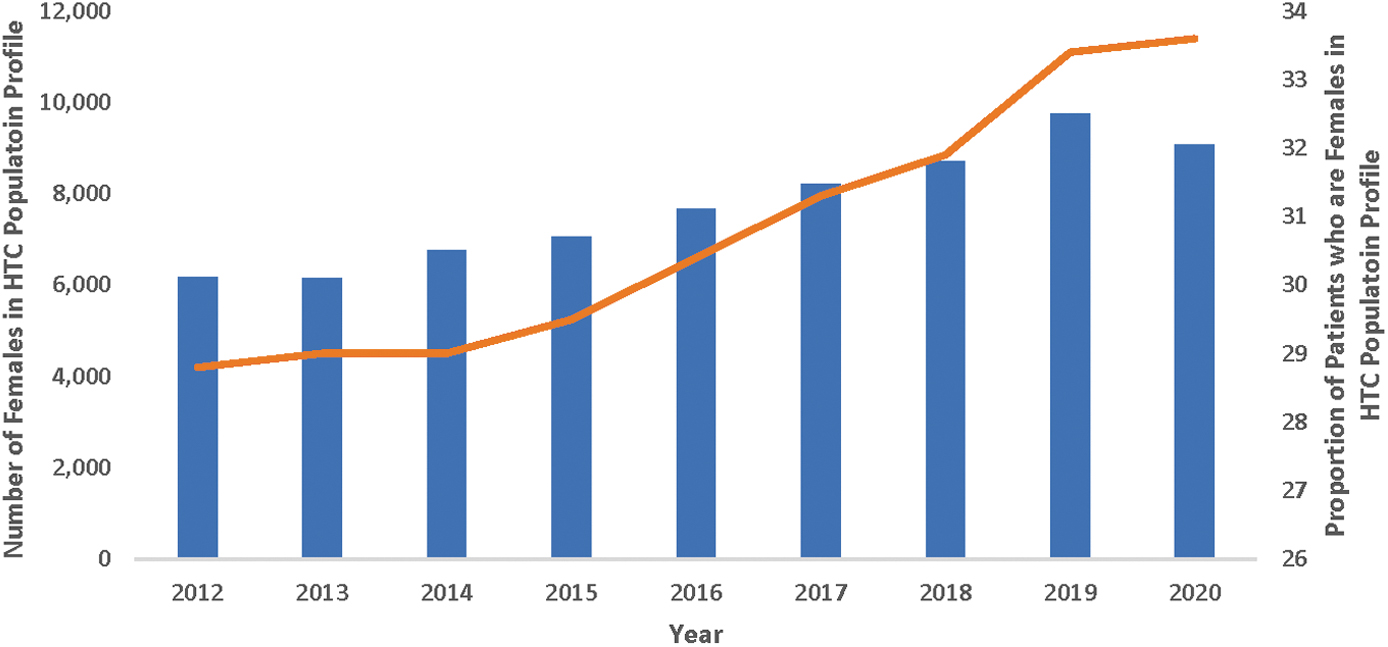
Number of females with diagnosed bleeding disorders (bars) and proportion of females among all patients (line) in the Community Counts HTC Population Profile by year from January 2012 through December 2020. HTC, Hemophilia Treatment Center. Color images are available online.
Table 2 provides further details on females diagnosed with bleeding disorders based on the methods described in recent publications and reported from January 2012 through March 2021. 14,15,30 Overall, during the entire time period, 41.8% of persons receiving care for bleeding disorders were women; however, there was substantial variation by type of disorder. As expected, a small minority of patients with hemophilia were female (7.9%). However, for every other disorder, most patients seen at HTCs were female, ranging from 54.0% for other factor deficiencies to 73.6% for connective tissue disorders and fibrinolytic disorders.
Number of Total Patients and Proportions of Female Patients Diagnosed with Bleeding Disorders Reported to the Community Counts Hemophilia Treatment Center Population Profile from January 2012 Through March 2021
Data extracted from the Community Counts HTC Population Profile (
Categories were combined to prevent derivation of cell counts of ≤5 by subtraction to protect patient confidentiality.
In terms of proportionate distribution of disorders among female patients who received care at HTCs, VWD was by far the most common disorder, accounting for 61.5% of females seen at HTCs for a bleeding disorder. Platelet disorders (storage pool disease, hereditary thrombocytopenia, Glanzmann thrombasthenia, Hermansky–Pudlak syndrome, Bernard–Soulier syndrome, platelet release defects, Gray platelet syndrome, and others) and other clotting factor deficiencies (factors I, II, V, VII, X, XI, XIII, and V and VIII combined) accounted for 18.6% and 10.6%, respectively, and connective tissue and fibrinolytic disorders together accounted for 2%.
Ongoing data collection through the Community Counts Registry provides an opportunity to monitor treatment, complications, and outcomes over time among women with bleeding disorders. Table 3 shows the number and proportion of female patients seen at HTCs who are enrolled in the more comprehensive data collection effort of the Registry. Altogether, 3,943 women and girls were reported to the Registry through March 2021. The vast majority had VWD, which aligns with the total number of women treated at HTCs (and thus included in the HTC Population Profile).
Comparison of the Number of Females with Each Type of Bleeding Disorder Enrolled in the Community Counts Registry for Bleeding Disorders Surveillance (CC Registry) from December 2013 through March 2021 (unpublished) to the Numbers of Female Patients Attending U.S. Hemophilia Treatment Centers as Reported to the Community Counts Hemophilia Treatment Center Population Profile from January 2012 Through March 2021
Data extracted from the Community Counts HTC Population Profile (
Categories were combined to prevent derivation of cell counts of ≤5 by subtraction to protect patient confidentiality.
CC Registry, Community Counts Registry for Bleeding Disorders Surveillance; HTC PP, Hemophilia Treatment Center Population Profile.
However, the condition with the largest proportionate representation in the Registry was hemophilia; 20.2% of females with hemophilia reported in the HTC Population Profile are represented in the Registry compared with 15.8% for VWD and 7.3%–12.8% for the other disorders. This is not surprising given that the primary impetus for the development of CDCs bleeding disorder surveillance program was to track HIV and other bloodborne pathogens in persons with hemophilia, and one of the driving forces behind the redesign of the surveillance program in 2012 was to provide more detailed tracking of hemophilia treatment complications. Although a minority of women and girls with bleeding disorders participate in the Registry, the sample is nonetheless sufficient for in-depth longitudinal tracking of many complications.
CDC Research Studies to Describe Gaps in Identification, Diagnosis, and Care Delivery
Over the past few decades, CDC scientists have led or collaborated in many important studies related to the identification and health care needs of women with bleeding disorders. Several CDC studies in the early 2000s demonstrated that HMB is often a hallmark feature for women with bleeding disorders, particularly VWD. In their study of the experiences of U.S. women with VWD, Kirtava et al. 8 documented that HMB was the most reported symptom. Dilley et al. 31 conducted a case–control study and reported that women with HMB were three times more likely to have a bleeding disorder as were women without HMB.
A later study that examined women with unexplained HMB who were referred to multiple U.S. clinical sites found that nearly three quarters had a laboratory abnormality indicative of a bleeding disorder, including platelet function defects, VWD, and non-VWD coagulation defects. 32 Study participants with laboratory abnormalities were eligible for a crossover treatment study, which demonstrated that both intranasal desmopressin and tranexamic acid treatments reduced menstrual blood loss and improved quality of life for women with HMB. 33
Not only has CDC research been essential to documenting the importance of screening women with HMB for bleeding disorders, a screening tool to help OB-GYNs and other primary care providers identify women with HMB who could benefit from laboratory evaluation for bleeding disorders was developed 34,35 and validated 36 in CDC-sponsored studies.
Other CDC studies have demonstrated that women with bleeding disorders commonly experience lengthy delays from onset of bleeding symptoms to diagnostic assessment and diagnosis. A 2004 study documented on average a 16-year delay (range 0–39 years) between onset of abnormal bleeding symptoms and diagnosis. 37 A subsequent study, using data from the supplemental female module of the UDC surveillance program, reported that more than 70% of adult women eventually diagnosed with a bleeding disorder had experienced a delay from onset of symptoms to diagnosis with a median delay of 10 years. 38 The percentage of female adolescents with a diagnostic delay was lower but still more than 50%, with a median delay of 4 years.
Underrecognition of bleeding disorders and delays in diagnosis may lead to the exacerbation of complications, reduced quality of life, and unnecessary surgical treatment, such as hysterectomies. Females with HMB due to a bleeding disorder may initially present to an OB-GYN or other primary care provider for care. The American Congress for Obstetricians and Gynecologists developed three committee opinions to facilitate screening, referral, and management of bleeding disorders. 39 –41 Despite this guidance, CDC-sponsored surveys during the past two decades report significant gaps in many OB-GYNs' understanding of the risks and impacts of bleeding disorders in women.
For example, only 4% of OB-GYNs who responded to a 2002 survey in Georgia considered VWD as a possible cause of HMB; these physicians also estimated that only about 1% of women with HMB might have VWD. 42 The true rate was at least 10%. 31 An updated survey in 2012 43 showed increased awareness of VWD as a differential diagnosis; however, more than 50% still underestimated its prevalence in women, and more would consider the diagnosis among adolescents (77%) than among reproductive-age adults (39%). These data align with other studies that have reported that irrespective of hemostatic events and HMB, females are often not referred to hematologists for diagnosis. 44
Women's difficulty accessing care is compounded by the complexity of diagnostic laboratory testing for females, in which results are often more difficult to interpret for females than males because some test results may be altered by female hormones. CDC laboratory studies in women with HMB provided empiric evidence of the degree of variation of certain coagulation proteins according to a woman's race, blood type, and time during menstrual cycle when blood is drawn; these studies indicate that the sensitivity of diagnostic VWD laboratory tests in women may be differential according to Black versus White race, type O blood type versus other blood types, and timing of tests. 45,46
Additional barriers to timely identification and care for bleeding disorders in females relate to their lived experiences. While CDC has not undertaken research in this area, we note here several pivotal studies of women's self-reported barriers to care. In various studies, women reported that their symptoms made them feel isolated and stigmatized 47 and that they have perceived discrimination and sometimes bullying from health care providers because of their gender, with their symptoms not taken seriously. 11,12,47 An American Academy of Pediatrics Committee study found that only 4 of 10 women experiencing HMB sought care for it. 48
Moreover, because participants often understood their own bleeding in the context of their female family members' experiences (i.e., they were not always able to differentiate between normal and abnormal bleeding symptoms themselves), 11 the potential effects of a dismissive attitude by a health care provider might be particularly detrimental to receipt of a timely diagnosis. A recent publication notes historical and ongoing sexism in the management of bleeding disorders due in part to societal stigmatization of menstruation, which further perpetuates underrecognition, underdiagnosis, and undertreatment of HMB. 49
In summary, there is an unacceptable delay in recognition and diagnosis of bleeding disorders in women, highlighting the need for early screening and referral by primary care providers and increased provider awareness to improve the identification and management of women with bleeding disorders.
CDC Health Promotion Programs to Increase Awareness and Early Identification of Bleeding Disorders in Girls and Women
The CDC currently funds and collaborates with the National Hemophilia Foundation (NHF) and the Hemophilia Federation of America (HFA) to develop and implement health promotion and prevention programs for women and girls with bleeding disorders. The desired outcomes for these programs are for undiagnosed females to recognize their bleeding symptoms and seek care; for health care providers to identify females with signs and symptoms of a bleeding disorder and refer them to hematologists for diagnostic testing; and for hematologists to appropriately diagnose and provide treatment to reduce morbidity and improve quality of life.
The Better You Know campaign ( An online, interactive screening tool was developed to assess whether women and girls with certain bleeding symptoms may be at risk for a bleeding disorder. Print materials (available in English and Spanish) were created for women and girls to provide information about the signs and symptoms of bleeding disorders and to facilitate communication with hematologists and other health care providers. Women with bleeding disorders shared their experiences through videos, talking about their journeys from the onset of their symptoms through their diagnosis and the empowerment they gained from knowing their diagnosis. Both print materials (brochures) and webinars were developed to help health care providers, such as OB-GYNs and primary care providers, understand and assess bleeding symptoms in women and girls, estimate an individual's risk for a bleeding disorder, and coordinate care for women and girls who require care from a hematologist for diagnostic testing.
Better You Know will be expanded to include a program for women and girls at risk for bleeding disorders to support them in receiving a diagnosis and appropriate care for their bleeding symptoms. The new program will provide information and resources to help women and girls as they navigate different health care providers, various clinical assessments and laboratory tests, and insurance barriers during the process of getting a diagnosis, treatment, and care.
The collaborative work between CDC and HFA includes activities to empower and educate women at risk for and women with bleeding disorders. In 2019, discussion groups were held among adult women diagnosed with bleeding disorders to learn about their experiences with symptoms, diagnosis and treatment, and identify perceived gaps in care. Participants identified several similar themes that have been previously published, reinforcing the underrecognition, underdiagnosis, and undertreatment of females with bleeding disorders in the U.S.
In a separate activity, an online learning management module was developed to increase knowledge and awareness among undiagnosed and diagnosed females within the bleeding disorders community. The educational module is accessible via the HFA website (
Future collaborative activities with NHF and HFA include the development of innovative provider training programs for hematologists and OB-GYNs. The provider training program content will be developed based on assessments of the current knowledge, attitudes, and practices with regard to women with bleeding disorders. These training programs should increase the number of women and girls with a bleeding disorder who are referred to a hematologist for diagnosis, as well as the number of diagnosed females who receive treatment that effectively manages their bleeding symptoms and prevents bleeding disorder-related complications.
Conclusions
CDC bleeding disorder programs include a comprehensive surveillance program that actively tracks women and girls with bleeding disorders who receive care at federally supported HTCs throughout the U.S., research to understand the gaps in identification, diagnosis, and care delivery for women and girls with bleeding disorders, and collaboration with community organizations in the development of public health promotion programs and educational strategies to address the gaps in patient and provider awareness of bleeding disorders and facilitate early diagnosis. Ongoing surveillance and research activities encompass bleeding phenotypes, complications, treatments, quality of life, and the quality of care and lived experience of women and girls with bleeding disorders.
Additionally, the findings generated from surveillance and research activities will continue to inform the development of new public health programs aimed at improving diagnostic and health care services and ultimately empowering women with bleeding disorders with the knowledge they need to navigate a complex health care system with the need for numerous types of specialty care. Timely recognition and diagnosis of bleeding disorders are key in ensuring appropriate care and treatment of women and girls. Additionally, building provider awareness and understanding of the unique needs of women and girls will be essential to ensure optimal outcomes and quality of life for women and girls with bleeding disorders.
Footnotes
Acknowledgments
The data reported in this publication were collected through the collaboration of ATHN, CDC, and the USHTCN using ATHN Study Manager. The authors would like to thank ATHN, the USHTCN regional leadership, and clinicians and staff at over 145 hemophilia treatment centers for their efforts in the ongoing implementation of Community Counts. The authors would like to especially thank the patients and families who contributed their information to the project. They also thank the National Hemophilia Foundation and the Hemophilia Federation of America for their collaboration on the development of health promotion, education, and prevention programs through cooperative agreement awards DD000006 and DD000008.
Disclaimer
The contents are those of the author(s) and do not necessarily represent the official views of, nor an endorsement, by CDC/HHS, or the U.S. Government.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
Community Counts (cooperative agreement award DD000020) is supported by CDC/U.S. Department of Health and Human Services (HHS) as a part of a financial assistance award totaling $4,300,000 with 100% funded by CDC/HHS.