
Abstract
Opioid use disorder (OUD) poses a significant public health concern impacting maternal and infant outcomes. In 2018, the Centers for Disease Control and Prevention (CDC) partnered with the Association of State and Territorial Health Officials (ASTHO) to develop the Opioid use disorder, Maternal outcomes, and Neonatal abstinence syndrome Initiative Learning Community (OMNI LC) to identify and disseminate best practices and strategies for implementing systems-level changes in state health departments to address OUD affecting pregnant and postpartum persons and infants prenatally exposed to opioids. In 2019, the OMNI LC incorporated a field placement approach that assigned temporary field placement staff in five select OMNI LC states to provide important linkages, facilitate information sharing, and strengthen capacity among state and local health departments and other partners supporting maternal and child health communities affected by the opioid crisis. Using an implementation science framework, the field placement approach was assessed using five implementation outcome measures: appropriateness, acceptability, implementation cost, sustainability, and feasibility. Written responses from the participating OMNI LC states on these implementation outcome measures were analyzed to (1) highlight key strategies used by field placement staff, (2) assess the implementation of the OMNI LC field placement approach within the context of implementation science, and (3) identify implementation barriers. This report describes the implementation of a temporary field placement approach and suggests that this approach could be replicated to enhance state and local capacity to respond to the opioid crisis or other high-consequence events.
Introduction
Opioid use disorder during pregnancy and neonatal abstinence syndrome
Opioid use disorder (OUD)
Estimated rates of NAS increased from 4.0 per 1000 hospital births in 2010 to 7.3 per 1000 hospital births in 2017. 1 The recent increase of NAS has been primarily from prenatal opioid exposure alone or in combination with other substances, and thus is sometimes referred to as neonatal opioid withdrawal syndrome. 2 In this article, neonatal withdrawal will be referred to as NAS.
In 2018, the Centers for Disease Control and Prevention (CDC)'s National Center for Chronic Disease Prevention and Health Promotion (NCCDPHP), in partnership with the National Center on Birth Defects and Developmental Disabilities (NCBDDD), the Center for State, Tribal, Local, and Territorial Support, and the National Center for Injury Prevention and Control (NCIPC), collaborated with the Association of State and Territorial Health Officials (ASTHO) to establish the Opioid use disorder, Maternal outcomes, and Neonatal abstinence syndrome Initiative Learning Community (OMNI LC). 3
The main objective of the OMNI LC was to identify and disseminate best practices and strategies for implementing systems-level changes in state health departments to address OUD affecting pregnant and postpartum persons and infants prenatally exposed to opioids. In 2019, CDC and ASTHO added a field placement approach (also referred to as the Local Enhancement Project 4 ) to the OMNI LC designed to create stronger partnerships and linkages between state and local health departments and community partners; facilitate information sharing of best practices; and strengthen public health capacity at the state and local levels. This approach included assigning temporary field placement staff (e.g., locally based public health professionals) in selected OMNI LC state and local health departments.
We used an implementation science framework developed by Proctor et al. 5 to assess the implementation of the OMNI LC field placement approach to enhance state and local capacity. We selected five of the eight implementation outcomes in the Proctor framework that were most pertinent to our assessment of the field placement approach. These included appropriateness, acceptability, implementation cost, sustainability, and feasibility. 5
The purpose of this report is to (1) highlight key strategies used by field placement staff, (2) assess the implementation of the OMNI LC field placement approach to enhance state and local capacity within the context of select implementation outcome measures, and (3) identify implementation barriers. Findings may inform future use of temporary field placement approaches to enhance state and local capacity to respond to the opioid crisis or other high-consequence events.
Background
Using a temporary field placement approach to enhance capacity
Use of temporary field placement staff to support OMNI LC activities is similar to previous efforts utilized by federal agencies and other organizations to address local needs and enhance capacity for public health emergencies, such as the Zika and Ebola outbreaks. 6 –8 For example, in 2014, CDC launched a temporary epidemiology field assignee program to assist and strengthen state and local capacity for public health preparedness to respond to the Ebola risk in the United States. 6
In response to the 2016–2018 Zika outbreak, CDC rapidly implemented the Zika Local Health Department Initiative (LHDI), which included a temporary field placement approach, to increase response capacity in health departments to improve Zika-related pregnancy and birth defects surveillance, enhance clinical and community education and outreach, and increase referral to services for families affected by the Zika virus. 8
Given the potential of temporary field placement approaches to enhance state and local capacity in high-consequence events, CDC collaborated with ASTHO to develop this field placement opportunity, which was modeled after the previously mentioned Zika LHDI. Select OMNI LC state teams were provided temporary field staff to advance key priorities and strategies in local settings that addressed the needs of pregnant and postpartum persons with OUD and infants prenatally exposed to opioids and other substances.
OMNI LC activities and focus areas
Fifteen state teams participated in the OMNI LC from 2018 to 2021 (Cohort 1: Alaska, Florida, Illinois, Kentucky, Ohio, Nevada, Pennsylvania, Rhode Island, Vermont, Tennessee, Washington, and West Virginia; Cohort 2: Indiana, New York, and Wyoming). The OMNI LC activities included the development of state action plans, planned virtual learning sessions and technical assistance, collaboration and information sharing across OMNI LC states, and the use of temporary field placement staff in select OMNI LC states. Details on the development and implementation of the OMNI LC are reported elsewhere. 3
To inform key activities and strategies for the OMNI LC, ASTHO and CDC identified and defined six focus areas for systems improvement: provider awareness and training; access to and coordination of quality services; data, monitoring, and evaluation; ethical, legal, and social considerations; financing and coverage; and consumer awareness (See Table 1 for focus area definitions). Stakeholder partnerships were also identified as a cross-cutting strategy used to support implementation of activities in each focus area.
Focus Areas and Examples of Key Strategies Addressed with Support from Field Placement Staff, OMNI LC 2019–2020
Kroelinger et al. 15
Definition of consumer awareness not published—information here is based on an internal document.
A strategy is defined as a method or technique used to enhance the adoption, implementation, and sustainability of a program, practice, or policy. Strategies should identify/define discrete components operationally, including who enacts the strategy (actor); actions, steps, or processes, using active verb statements (action); and the target of the strategy (action target). (
NAS, neonatal abstinence syndrome; OMNI LC, Opioid use disorder, Maternal outcomes, and Neonatal abstinence syndrome Initiative Learning Community; OUD, opioid use disorder; POSC, plans of safe care; PQC, perinatal quality collaborative; SBIRT, screening, brief intervention, and referral to treatment.
For the OMNI LC field placement approach, the scope of work for each temporary field placement varied by state and was linked to OMNI LC state action plan priorities or strategies that addressed at least two key OMNI LC focus areas: (1) provider awareness and training and (2) access to and coordination of quality services. All field placement staff also addressed the cross-cutting strategy of stakeholder partnerships by working to enhance collaboration and engagement with relevant groups at the state and local levels (Fig. 1).
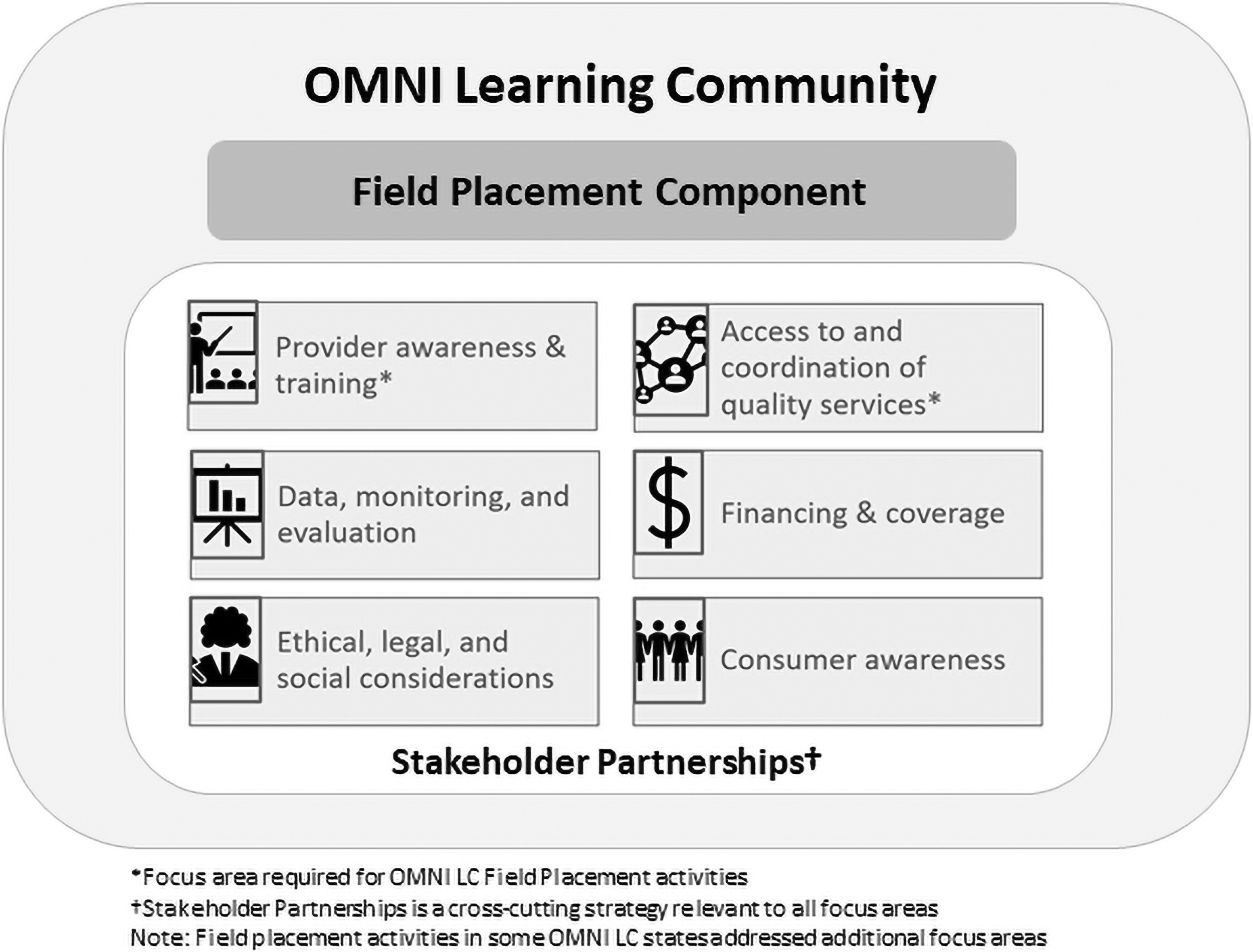
OMNI learning community focus areas. OMNI, Opioid use disorder, Maternal outcomes, and Neonatal abstinence syndrome Initiative.
OMNI LC field placement process
To identify participating states for the OMNI LC field placement approach, letters of invitation were sent to OMNI LC Cohort 1 states in April 2019. An objective review process for field placement staff applications included a review of state-submitted work plans providing justification for the field placement staff, key proposed activities for the position, plans for engaging community partners, and letters of support from state and/or local health officials.
Qualifications for field placement staff included a graduate-level degree in public health or other health-related field, and experience planning and administering health-related programs. Field placement staff demonstrated skills in using public health data to inform activities, managing multiple projects and priorities, cultivating partnerships, and communicating effectively. Field placement staff provided field-based surge support for up to 1 year. The five states from the OMNI LC selected to participate were Florida, Kentucky, Nevada, Ohio, and Washington.
After site selection, ASTHO collaborated with state teams and CDC to develop a scope of work and job description for each field placement that aligned with their OMNI LC state action plan. Field placement staff were supervised by the respective health departments with guidance and input from ASTHO and CDC. ASTHO and CDC conducted site visits in each state to meet with state health department leaders and staff, community partners, and the newly hired field placement staff.
Site visits included a review of roles and responsibilities and discussion of how the field placement positions aligned with the OMNI LC state action plan goals and other state and local opioid-related efforts. In partnership with CDC, ASTHO provided field placement staff with technical assistance, access to subject matter experts, and connections to other health departments and resources using a capacity building and technical assistance (CB/TA) model 9 focused on systems-level change supporting pregnant and postpartum people with OUD and infants prenatally exposed to opioids and other substances.
Methods
We examined the implementation of the OMNI LC field placement approach to enhance state and local capacity using implementation science outcome measures. 5 Implementation science is the study of methods to promote integration of evidence-based interventions to affect change in health care and public health settings that ultimately improve health outcomes, while also considering how these interventions function within a broader dynamic public health context. 10 Implementation science offers various tools and frameworks 11 that can help identify factors that facilitate or hinder implementation of evidence-based interventions.
Proctor's conceptual framework for implementation outcome measurement was used to systematically document how field placement staff implemented proposed activities and contributed to OMNI LC efforts within assigned states. According to Proctor et al., 5 implementation outcomes are the effects of deliberate actions to implement interventions or services and can be indicators of implementation processes or implementation success.
We developed a series of assessment questions administered for field placement staff and direct supervisors at the end of the field placement assignment to measure the implementation of the field placement approach focused on five implementation outcomes: appropriateness, acceptability, implementation cost, sustainability, and feasibility. Proctor's implementation outcome definitions along with a description of their relevance to the implementation of the field placement approach are provided in Table 2.
Examples of Implementation Outcome Measures for the OMNI LC Field Placement Approach, OMNI LC 2019–2020
Based on definitions of implementation outcomes provided by Proctor et al. 5
Implementation outcome measures were determined by analyzing content within data sources provided by field placement states that aligned with the definition of each implementation outcome.
“Feasibility” was an implementation outcome informed by the four other implementation outcomes.
ASTHO, Association of State and Territorial Health Officials.
Written responses to the assessment questions served as a key data source for the analysis of implementation outcome measures. To provide additional context, these responses were complemented by field placement final reports submitted to ASTHO and ASTHO's final project summary submitted to CDC. Feasibility was assessed based on the culmination of information gathered for the other four implementation outcomes.
An initial group of reviewers transferred excerpted assessment responses into an Excel spreadsheet organized by implementation outcome measure and further coded these qualitative data to (1) highlight key focus areas and strategies used by field placement staff, (2) assess the field placement approach within the context of the implementation outcome measures of interest, and (3) identify implementation barriers. These findings were validated by a separate group of reviewers and differences were resolved through consensus-based discussion.
Results
Key focus areas and strategies used
State health departments and ASTHO collaborated with field placement staff to implement activities within the focus areas of provider awareness and training and access to and coordination of quality services while also facilitating stakeholder partnerships. Table 1 provides examples of key strategies by OMNI LC focus area implemented by the five field placement states. Field placement staff from each of the five states implemented at least one strategy focused on provider awareness and training, which included training opportunities and collaborative activities among networks of health care providers.
State and local partners engaged field placement staff to develop resources and coordinate training opportunities for health care providers on topics such as OUD and pregnancy; NAS; screening, brief intervention, and referral to treatment (SBIRT) 12 ; and plans of safe care (POSC). 13 Perinatal quality collaboratives (PQCs), which are state-based networks of multidisciplinary providers that implement quality improvement science using rapid cycle data analysis to improve the health of mothers and infants, 14 have been identified as a key strategy and facilitator that advanced OMNI LC efforts. 15 Two of the states utilized field placement staff to partner with state PQCs to raise awareness about OMNI LC training opportunities and disseminate educational information and resources.
Field placement staff also contributed to advances in other OMNI LC focus areas, including access to and coordination of quality services; ethical, legal, and social considerations; and consumer awareness. Beginning in March 2020, stay-at-home orders due to the coronavirus disease 2019 (COVID-19) pandemic hindered efforts to engage community partners, which limited the ability of some field placement staff to address strategies related to the access to and coordination of quality services focus area. Field placement staff in two states were able to address this focus area by virtually convening health care providers and other community-level partners.
Virtual meetings were used as platforms to assess community-level challenges in care coordination for mothers with OUD and their infants before, during, and after delivery. Content discussed during convening sessions included the identification of POSC-related challenges, system-level barriers, and best practices to inform state-level action to improve care coordination at the local level.
Three of the five states considered implicit bias and stigma as priority issues for the ethical, legal, and social considerations focus area and field placement staff were able to incorporate these topics into focused training resources and webinars for various health care professional audiences. One state identified a need for the focus area of consumer awareness and the field placement staff was able to develop a video resource for women with OUD encouraging them to seek treatment.
Implementation outcome measures
We completed an assessment of the field placement approach within the context of five implementation outcome measures by analyzing content provided by the field placement states from the previously stated data sources. Findings for each implementation outcome measure are provided here along with examples that support implementation of the field placement approach in five OMNI LC field placement states as presented in Table 2.
Appropriateness
Appropriateness is the perceived fit, relevance, or compatibility of an innovation to address a particular problem. 5 This implementation outcome was assessed based on insights from field placement states on how the field placement approach fits within a health department to address maternal OUD-related priorities. All five field placement states indicated that this approach was compatible with their need for skilled locally based field staff to address key issues affecting pregnant and postpartum people with OUD and infants prenatally exposed to opioids and other substances. State teams noted that this approach allowed for efficient hiring of dedicated staff (i.e., the field placement) to focus on facilitating state to local linkages and addressing community needs for maternal OUD and NAS, which was key to advancing state OMNI LC goals.
All field placement staff were well positioned to immediately engage with key partners to advance state OMNI LC priorities. For example, field placement staff in two states leveraged PQCs to identify and communicate with key partners and facilitate connections; one of the field placement staff played an instrumental role in standing up a newly formed state PQC. Information from the field placement assessment responses and state final reports suggests the field placement approach was an appropriate mechanism to advance OMNI LC efforts.
Acceptability
The acceptability of an intervention is the perception among implementation stakeholders that a given innovation is agreeable, palatable, or satisfactory. 5 This implementation outcome was assessed based on the ability of the field placement staff to engage with stakeholders to inform key OMNI LC activities. Insights from assessment question responses provided by the five field placement staff and direct supervisors indicated that field placement staff were able to connect with and learn from key partners during assignments.
Two field placement staff were able to gather insights from local communities on critical local issues and needs, which resulted in the creation of various resources, such as health care provider trainings and the escalation of local priorities for state-level action. In collaboration with ASTHO, each OMNI LC state team also integrated the temporary field placement within the health department, demonstrating acceptability of the field placement approach within existing state and local infrastructures.
Implementation cost
Cost is defined as the cost impact of an implementation effort. 5 All five states reported utilizing resources (i.e., technical assistance, financial support for field placement staff, or a particular activity to support implementation efforts) to carry out activities suggesting that availability and flexibility of resources are an important element in implementing this field placement approach.
For example, several states mentioned that dedicated staff support and the flexibility of financial support for switching trainings to virtual meeting platforms were critical to implementing key activities as states were required to shift efforts to virtual formats. Also, field placement states acknowledged the importance of the technical assistance and support provided by ASTHO, which included activities such as facilitating connections with relevant partners, developing meeting agendas, providing facilitation services for events, and conducting audience evaluations for webinars and trainings.
Sustainability
Sustainability is defined as the extent to which a newly implemented treatment is maintained or institutionalized within a service setting's ongoing stable operations. 5 This implementation outcome was assessed based on how the field placement approach and activities were maintained or institutionalized within a health department's ongoing stable operations. As the OMNI LC field placement assignments came to an end, field placement states identified ways to continue and sustain the work of field placement staff beyond the assignment timeframe. Three out of five states described strategies to maintain or institutionalize field placement activities within the health department's ongoing operations.
Consistent across all three were the ongoing collaborations with key partners to continue the work of the field placement staff, such as partnerships and activities within the state PQC, increasing consumer awareness of POSC through state child welfare agency efforts, and ongoing support to connect hospitals with appropriate resources for referral and treatment of pregnant and postpartum people with OUD. Two of the three states were also able to secure permanent positions for the field placement staff within organizations working closely with state and local health departments.
Feasibility
Feasibility is defined as the extent to which a new treatment, or an innovation, can be successfully used or carried out within a given agency or setting. 5 This implementation outcome was assessed by reviewing information on the four other implementation outcomes to determine how the field placement approach was implemented within a health department.
Based on our assessment, the field placement approach was an appropriate fit and an acceptable mechanism for enhancing local capacity, implementation cost was appropriately utilized by each state team, and some field placement activities were sustained through ongoing partnerships with key stakeholders and the creation of permanent positions for field placements through partner organizations. Findings reported on these four implementation outcomes demonstrate that implementation of the field placement approach helped advance OMNI LC efforts.
Implementation barriers
When assessing implementation barriers across the state teams, the main challenge cited was the impact of changing priorities due to the COVID-19 pandemic. In some states, the pandemic presented a barrier to the implementation of training and collaborative activities at the local level. Field placement staff adapted and developed new strategies such as shifting planned in-person trainings to virtual platforms and, in several cases, moving webinars to training platforms or housing trainings on state websites so participants could readily access resources. In some cases, community-level meetings were put on hold or conducted virtually.
Due to the pandemic, state and local health department staff were assigned to other priorities unrelated to the work of the OMNI LC. Community partners were also affected as they navigated the impact of the pandemic on the populations they served. Despite these challenges, dedicated OMNI LC field placement staff enabled OMNI LC activities to move forward with the flexibility of modifying activities as needed. ASTHO also increased technical assistance support to field placement staff to assist several state teams in moving to virtual platforms and providing ad hoc guidance on programmatic issues. Findings highlighted in this report attest to the skills and flexibility of field placement staff to carry out proposed activities despite challenges due to the pandemic.
When asked about ways to improve the field placement approach, states noted that a longer timeframe for field placement support beyond 1 year could have offset delays related to administrative and pandemic-specific challenges, such as reassignments. There were also some delays in obtaining state and local approvals for various field placement activities. However, the assessment revealed that the hiring process through ASTHO allowed states to quickly orient field placement staff and begin to work on assigned OMNI LC activities. Despite shifting priorities and delays, the field placement positions were still able to focus on OMNI LC activities and continue advancing OMNI LC action plan goals.
Key Lessons Learned
Dedicated staff to support OMNI LC efforts
State teams reported that the addition of OMNI LC temporary field placement staff allowed them to quickly implement activities and focus on OMNI LC goals. Field placement staff were able to establish relationships and continue engagement of community partners at the state and local levels, develop and disseminate resources, offer webinars and training opportunities, and support other activities that aligned with OMNI LC state action plans. The pandemic highlighted the need for dedicated staff to provide continuity in state and local efforts to address opioid-related maternal and infant outcomes.
Technical assistance and support
Ongoing technical assistance was provided by ASTHO with support from CDC. ASTHO provided continuous support to build connections between field placement staff with stakeholders and other OMNI LC state teams, connected state teams with subject matter experts as speakers for various events, advised on content for meetings and focus groups, and assisted with meeting facilitation and post-training evaluations for state teams. ASTHO's expertise and connection to national and state resources enabled state teams to implement their OMNI LC action plan goals. Despite reassignments of local supervisors to pandemic-related activities, ASTHO staff were able to provide ongoing supervision and support for field placement staff as needed to ensure continued engagement of each state and advise on project deliverables and project management.
ASTHO also facilitated information and resource sharing among the five field placement staff and other states engaged in similar activities by hosting regular video and phone calls, which were instrumental in building relationships between field placement staff throughout the project period. Overall, ASTHO's CB/TA model and framework of ongoing technical assistance 9 directly contributed to the implementation of the OMNI LC field placement approach.
Limitations
Findings from this report were subject to at least four limitations. First, the qualitative responses collected reflect state team activities as reported by field placement staff and local supervisors participating in the OMNI LC field placement approach and do not represent all work done by OMNI LC state teams or other state opioid-related efforts. Second, qualitative data reported through written responses were subject to interpretation by the initial group of reviewers; however, an analysis protocol and consensus-based decision-making process, which included a separate group of reviewers, helped reduce overinterpretation of reported information.
Third, perceptions of key partners about the field placement approach and its impact on community-level OUD efforts were not gathered, which could have provided additional insights into the field placement approach. Lastly, the findings reported on the OMNI LC field placement approach are not generalizable to all states but do provide valuable information for future efforts requiring field-based surge support.
Conclusion
This report assessed a field placement approach using an implementation science framework to document strategies and implementation outcome measures. Using Proctor's implementation outcome measures, our assessment of five implementation outcomes—appropriateness, acceptability, implementation cost, sustainability, and feasibility—supports the implementation of the field placement approach in five states to advance OMNI LC efforts.
Dedicated staff allowed state teams to implement strategies and focus on OMNI LC goals despite challenges due to the pandemic. ASTHO played a key role in onboarding field placement staff, providing ongoing technical assistance, and supporting the field placement approach of the OMNI LC. This report describes implementation of a temporary field placement approach used to address opioid-related issues affecting maternal and child health populations and suggests that this approach could be replicated to enhance state and local capacity to respond to the opioid crisis or other high-consequence events.
Footnotes
Disclaimer
The findings and conclusions in this report are those of the authors and do not necessarily represent the official position of the Centers for Disease Control and Prevention.
Acknowledgments
The authors thank those who contributed to this work: participating OMNI LC state teams: Florida, Kentucky, Nevada, Ohio, and Washington; Florida Department of Health, Kentucky Department of Public Health, Nevada Division of Public and Behavioral Health and the Southern Nevada Health District, Ohio Department of Health, and Washington State Department of Health; field placement staff: Lori Reeves (FL), Monica Clouse (KY), Abra Greenberg (OH), Jennifer Somdahl (NV), and Navind Oodit (WA); and the ASTHO leadership team. Acknowledgments are also extended to Meghan Frey, Hadley Hickner, and Margaret Honein, Centers for Disease Control and Prevention; Alisa Joy Velonis and Molly McGown, University of Illinois at Chicago faculty and evaluation team; and the Opioid Response Coordinating Unit (ORCU), National Center on Injury Prevention and Control, Centers for Disease Control and Prevention, for supporting this work.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
Partial funding of this activity was provided by CDC-RFAOT18–1802 and CDC-RFA-OT18–1804.