
Abstract
Background:
Gender equity is a critical issue in academic medicine. Whether there is equitable access to the prestige and resources of endowed professorships merits evaluation. We investigated this question in obstetrics and gynecology, a field that focuses on the health of women and in which women are much better represented than other specialties of medicine.
Materials and Methods:
We compiled a list of the top 25 United States departments of obstetrics and gynecology and contacted department chairs (and used department websites) to obtain lists of faculty and their positions. Scopus, department websites, and National Institutes of Health (NIH) RePORTER were used to collect h-Index, number of publications and citations, graduation year, degrees, gender, and NIH-funding. We conducted a bivariate comparison of endowed professorship attainment by gender using a chi-square test and created a multiple variable regression model.
Results:
Of the 680 obstetrics and gynecology faculty across 23 departments that had endowed chairs, 64 out of 400 women (16%) and 66 out of 280 men (24%) held endowed chairs (p = 0.01). The multivariable model suggested no independent gender difference in attainment of an endowed chair after adjusting for covariates.
Conclusion:
To our knowledge, this study is the first to examine gender as a variable in endowed chair allocation in top obstetrics and gynecology academic departments. Our findings suggest a significant gender difference in the allocation of endowed chairs. That difference is driven by gender differences in academic rank, graduation year, publications, and funding. To promote the intraprofessional equity necessary to optimally advance women's health, further research and intervention are necessary.
Introduction
Gender equity is a critical issue facing academic medicine, a field in which scholarly productivity in the form of publications and research grants is used to make decisions regarding promotion, hiring, tenure, and salary. Unfortunately, even highly capable and motivated women who enter academic medicine appear to lag behind their male peers. For example, in a study of recipients of career development K-awards from the National Institutes of Health (NIH), gender was an independent significant predictor of R01 award attainment even after controlling for K-award type, year of award, funding institute, institution, and specialty. 1 Additionally, women have constituted only a minority of the authors of original research and guest editorials in the most prominent medical journals in the world for decades. 2 –5 Women are also less likely to hold positions of leadership in randomized clinical trials or in specialty societies. 6,7
Correspondingly, a meta-analysis of over 10,000 unique North American academic physicians found that women had significantly lower h-Indexes than men across most specialties and at all academic ranks. 8 Numerous mechanisms have been proposed for these differences, including unconscious bias, gendered societal expectations, sexual harassment, and differences in access to resources and sponsorship for opportunities. 9 –13
These factors underlie the daunting path that women physicians face toward achieving full professorship; it has been shown that women are statistically less likely to reach this career milestone, even when controlling for other factors. 14 Moreover, the gender gap in promotion to more senior ranks of academic medicine has not narrowed over time. 15 This disparity in women being recognized and rewarded for their work may also extend to the ability of women to be selected as endowed chairs in academic departments, which are coveted positions opening doors to elite career opportunities. Endowed chairs not only allow a faculty member to be identified as worthy of distinction through a title but also typically provide income that can support the chair-holder's salary or support their scholarly work. Gender differences in endowed chairs in top-tier U.S. medicine departments exist and persist even after adjusting for differences in specialty, degree, citations, funding, and graduation year. 16
However, this was not found in a parallel analysis in the subspecialty of oncology, where a smaller difference by gender was not statistically significant. 17 In pediatrics, a significant difference existed but was no longer significant on multivariable analysis, suggesting that gender differences in degree, publications, and funding were important explanations for the difference. 18 Further investigation is warranted, particularly in specialties like obstetrics and gynecology, where, like in pediatrics, women now constitute the vast majority of trainees and substantial proportions of the faculty ranks overall—83% of residents and 64% of faculty in recent data from the Association of American Medical Colleges. 19
To prioritize diversity, equity, and inclusion within academic medicine, it is critical to dissolve underlying systemic barriers that contribute to the gender gap in physicians' career trajectories. 20 This is a specific priority of multiple influential professional bodies, including the National Academies of Science, Engineering, and Medicine, which published a recent report with recommendations for addressing these gender barriers. 11 Such recommendations include identifying areas that might promote the ability of women to be agents of positive change within science and medicine. The equitable distribution of endowed chairs is one such area. To gain further insight into the effect of gender on endowed chair faculty positions, specifically in a field where women are much better represented than internal medicine, we conducted a study of the top 25 departments of obstetrics and gynecology in the United States, ranked by NIH funding. We specifically sought to determine whether the allocation of endowed chairs differed by gender and, if so, what other factors might explain that difference.
Materials and Methods
We used the Blue Ridge Institute for Medical Research website 21 to compile a list of the top 25 departments of obstetrics and gynecology in the United States, ranked by departmental NIH funding. We then contacted the chair of each of these departments via e-mail with a request for an up-to-date list of faculty at the associate and full professor levels, in addition to a list of their current endowed chair faculty. Those who did not respond were contacted a second time. Three departments declined to provide the requested information and four did not respond despite receiving e-mails from a well-known former department chair, so we considered these seven to have declined to provide the information. For departments that provided data (18/25), we relied on the faculty lists they provided to identify faculty members for this analysis. In the cases when our request was declined (28%; 7/25), we leveraged department websites to collect this information as described previously. 16
Following the acquisition of these faculty names, two independent researchers used Scopus to collect readily available variables that we theoretically prespecified: the h-Index, number of publications, and number of publication citations for each faculty member, as well as department websites to collect faculty medical school graduation year, degrees held, and gender. We used faculty pronouns found on websites as indicators for the faculty's gender. Using the NIH RePORT Expenditures and Results (NIH RePORTER), we collected data on the total amount of NIH funding received to date by each faculty member. Both independent researchers completed a second round of data collection for a subset of the other researcher's data collection to ensure consistency in coding.
We first described the distribution of endowed chairs among 735 faculty members at the 25 institutions and described those faculty by gender, degree, and rank. The remainder of the analyses focused only on faculty at the 23 institutions where there was at least one endowed chair (because the complete absence of endowed chairs was likely an institutional policy or practice reflecting lack of opportunity for any faculty at those institutions to hold an endowed chair position). We further excluded 14 individual faculty members whose professional degrees were CNM, DNP, or other because this represented a dissimilar and small population of faculty, we also excluded these professors from calculation of the association of professor characteristics with having an endowed professorship. After describing the remaining 680 faculty at 23 institutions who constituted the analytic sample for characteristics associated with endowed professorship, we performed a bivariate comparison of attainment of endowed professorship by gender, using the chi-square test statistic.
Next, we created multiple variable regression models using all of the readily available, prespecified, theoretically selected professor characteristics to explain having an endowed chair. Because the metrics of publication output and quality (number of publications, number of citations, and h-Index) are highly correlated, we constructed models separately using all other professor characteristics and only one metric of publication output. Estimates were compared across models for the other professor characteristics, and the overall goodness of fit was compared using Akaike's Information Criteria (AIC) to identify the metric of publication output and quality that was the most appropriate. The model with the lowest AIC value was considered the best fitting.
The University of Michigan Institutional Review Board deemed the study exempt.
Results
We identified 735 obstetrics and gynecology faculty across the 25 leading academic programs. Figure 1 displays the percentage of women among full and associate professor faculty in each department, as well as the percentage of full and associate professor faculty in each department who hold endowed professorships. As shown in Figure 1, 2 of the 25 institutions had absolutely no endowed professorships.
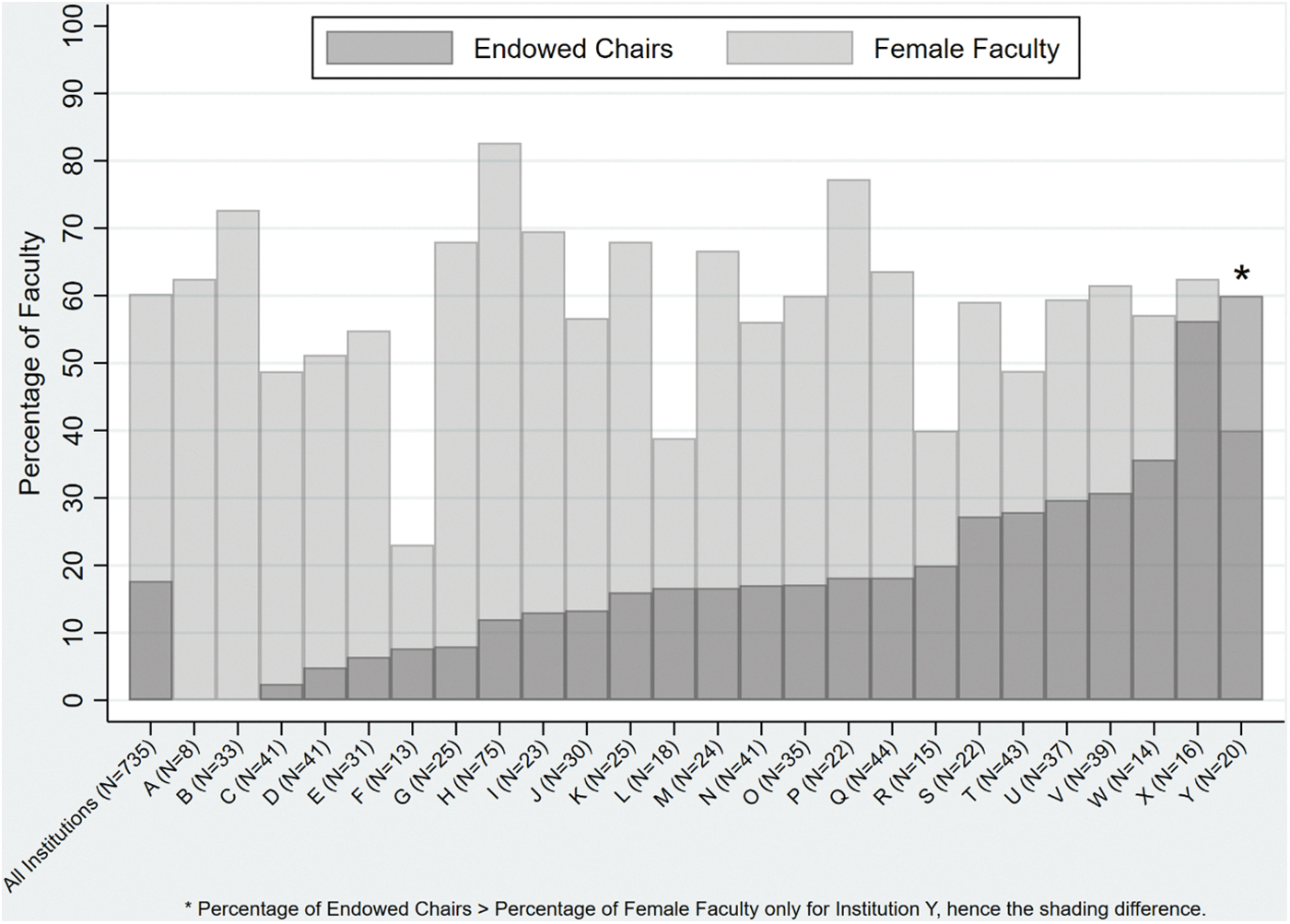
Percentage of full and associate professor faculty who are women and who hold endowed chairs in 25 top obstetrics/gynecology departments. For each of the 25 top obstetrics and gynecology programs (and for all programs combined), this bar chart depicts the proportion of all full and associate professor faculty who are women and the proportion of all full and associate professor faculty who hold endowed chairs.
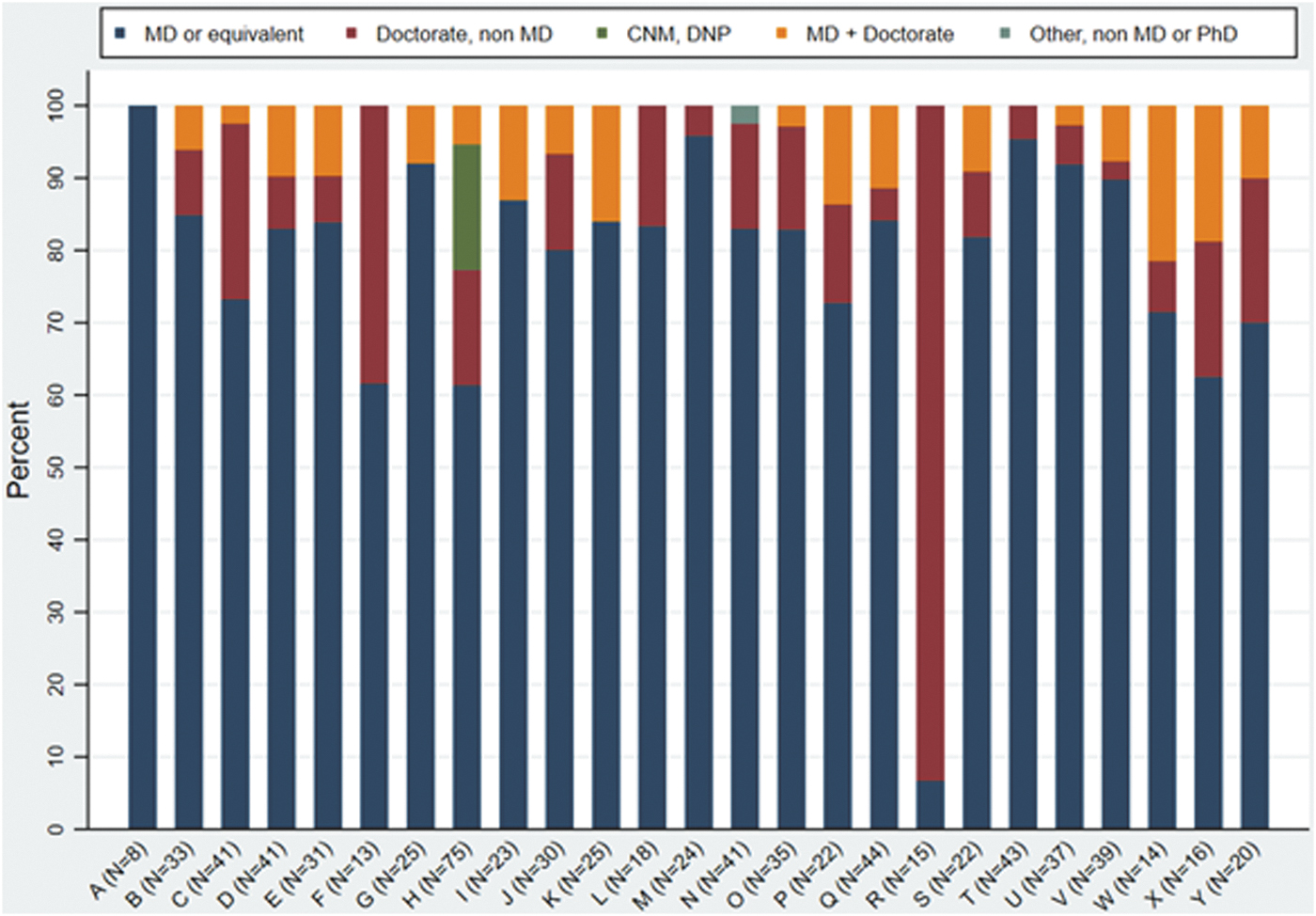
Percent of faculty by degree among full and associate professors at 25 top obstetrics and gynecology programs (N = 735). For each of the 25 top obstetrics and gynecology programs, this stacked bar chart depicts the percentage of full and associate professors with the following degrees: MD (or equivalent), Doctorate (non-MD), CNM/DNP, MD+Doctorate, or Other (non-MD or PhD). Program labels and ordering are identical to Figure 1.
Figure 2 displays the distribution of type of degree for the faculty members by institution. Only one institution (Institution H) had obstetrics and gynecology faculty with the terminal degree of CNM or DNP (N = 13 professors), and one institution (Institution N) had a single professor with an ‘Other’ degree.
This left a final analytical sample size of 680 faculty members (full professors and associate professors, all holding MD/equivalent or PhD degrees) from 23 institutions for evaluation of characteristics associated with endowed professorship. Of the 680 professors (400 women and 280 men), 130 (19%) held endowed chairs. Of these, 64 women (16%) and 66 men (24%) held endowed chairs (p = 0.01).
Table 1 presents the sample characteristics of the professors in total and stratified by those with and without endowed chair and finally within those groups stratified by gender. It demonstrates that the most common degree type among all professors (80.7%) and among endowed chairs (75.4%) was an MD without additional doctorate. Among these MDs without additional doctoral degrees, of those with endowed chairs, the majority (53.1%) were men and a minority (46.9%) were women. By contrast, among MDs without additional doctoral degrees who did not hold endowed chairs, a substantial majority (63.9%) are women and a smaller minority (36.1%) were men.
Faculty Characteristics Stratified by Attainment of Endowed Chair and Further Stratified by Gender
Metrics of publication output and quality were presented using cut point at the approximate quartile values for categorization.
NIH, National Institutes of Health.
As shown in Figure 3, the multivariable model suggests that there was no independent gender difference in attainment of an endowed chair that remained after adjusting for the measured covariates. The data do suggest that faculty with a non-MD doctorate were significantly less likely to have endowed chairs, as were those professors with an academic rank of Associate Professor. Those in the highest quartiles of number of publications and those in the highest funding quartile were significantly more likely to have an endowed professorship. Attainment of an endowed professorship was not significantly related to the decade the faculty graduated.
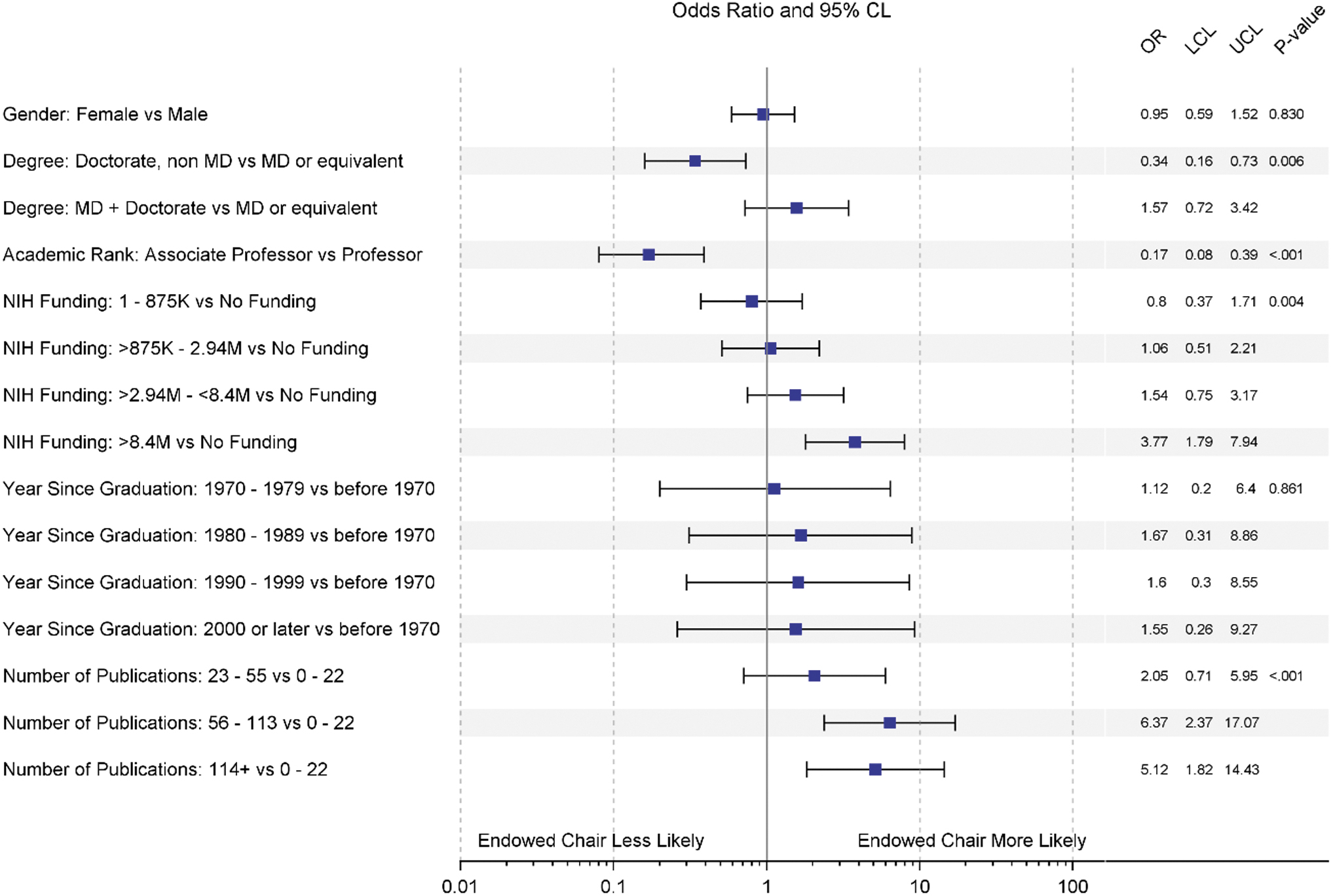
Forest plot of multivariable model of holding an endowed chair among full and associate professors in 23 top obstetrics and gynecology programs. This figure depicts the associations observed in a multiple variable logistic regression model in which holding an endowed chair was the dependent variable.
Discussion
This study is the first to our knowledge to examine gender as a variable in the allocation of endowed chair positions in top academic departments of obstetrics and gynecology, and it expands on the burgeoning research on this topic across medical specialties. 16 –18 As in a prior study conducted in internal medicine, a field with a lower representation of women, and in pediatrics, where women are better represented overall, women were also significantly less likely to hold endowed chairs than men in this sample of faculty in obstetrics and gynecology on bivariate analysis. Nearly one in four men in this sample held an endowed professorship, as compared with one in six women.
On multivariable analysis, MDs, full professors, those in the highest quartiles of number of publications, and those in the highest funding quartile were significantly more likely to have an endowed professorship. However, no significant gender difference was observed after adjustment for other variables, suggesting that the gender difference in holding an endowed chair in this sample was explained by gender differences in the other variables measured and included in the model. This diverges from previous work conducted on internal medicine faculty, where the gender difference was not fully explained by other measured variables, 16 and is more similar to the findings among pediatrics faculty. 18 These findings together help to illuminate the mechanisms that underlie differences in women's attainment of prestigious positions and how they may differ across disciplines.
Obstetrics and gynecology has transformed substantially over the past few decades in terms of the number of women going into the field. In 1970, 7% were women, but women are now the vast majority of trainees and the majority of practicing physicians in this specialty. 19,22,23 It is possible this shift in gender representation has helped to improve challenges faced by women in the specialty, reducing the impact of factors other than those measured in this study in driving the difference in attainment of endowed chair positions. However, it is important to recognize that a gender difference in attainment of endowed professorship did exist even in this field in which women now constitute the majority.
The differences in publication, funding, and rank that contributed to driving this difference should be recognized to not simply be meritocratic criteria but also reflections of the impact of ongoing structural, unconscious, and conscious biases that differentially affect women, even in fields like this one where they have achieved substantial representation overall. Still, it is heartening to see that women constituted increasing proportions of endowed chairs among faculty with more recent years of graduation; ongoing monitoring and research will be important to evaluate whether the gender gap observed in this study improves as older generations retire.
It is interesting to consider these findings in the context of a 2016 study, which indicated that obstetrics and gynecology shows a lack of progression of women to departmental leadership. 24 Whether that difference would also be wholly explained by differences in factors like publication rates, grant funding, rank, and year of graduation would be valuable to explore. Ultimately, to ensure gender equity in influential positions such as endowed chair positions and department chair positions, attention must be given to upholding women faculty's support early in the academic pipeline.
Also important to consider are the characteristics of donors and their role in directing donations. Perni et al recently showed that at one large academic cancer center, male faculty oncologists were more likely to receive philanthropic donations than their female colleagues. 25 This difference was no longer significant after adjustment for productivity and rank. Ensuring equity in allocation of philanthropic support, including endowed chairs, requires careful consideration of institutions' approaches to development more generally. Individuals from systematically marginalized and excluded groups are less likely to be donors, and academic medical centers must be careful not to allow this fact to amplify disparities in services that benefit members of those groups or disparities in the professional career outcomes of members of those groups. 26
Limitations of this study include that data on faculty identifying as genderqueer or nonbinary was not captured from online resources, and departmental websites were relied upon to collect a portion of the data, although it is unclear if the websites are fully up to date. Furthermore, the sample was limited to the top 25 departments of obstetrics and gynecology in the United States. There were also differences in the allocation of endowed chair positions by degree type, with certain institutions such as Institution N and Institution R filling these positions with PhD-prepared faculty rather than those with a medical degree. The sample size was insufficient to subdivide into subgroups of this sort.
Certain information was not available to us, including funding from sources other than the NIH, information about total endowed chairs at each institution, timing of individual chair appointments, processes for selecting chairs, and how endowment funds are actually used by chair holders. Future research should attempt to collect this information, which would be illuminating. Additional directions for future research include further investigation of the distribution of endowed chair positions, such as studies of racial differences in chair allocations 27 and gender differences in specialties yet to be examined through academic research on the topic.
In summary, this study adds to the literature seeking to understand why women remain underrepresented in positions of influence and authority in academic medicine. Investigation within specialties in which women are highly represented in numbers but nevertheless remain underrepresented in leadership positions is especially important. Abundant evidence suggests that inclusion of women in the medical profession improves the important outcome of women's health. 28,29 Ensuring that women have equal access to resources and opportunities like those afforded by endowed professorships is essential. Efforts are necessary to focus on transparency regarding how potential recipients of endowed chair positions are selected and introduced to donors. 25 Finally, because this study suggests that differences in academic rank, funding, and publications help explain gender differences in holding the privileges that come from an endowed chair in top obstetrics and gynecology programs, attention should be directed at mechanisms that may affect women's ability to achieve promotions, publications, and funding in that field.
These include innovation, evaluation, and dissemination of creative interventions intended to address unconscious bias and overt harassment, as well as initiatives to address structural barriers, such as the need to facilitate combining careers in medicine with motherhood through on-site lactation facilities and childcare. Creative efforts to promote equity continue to be necessary even in fields like obstetrics and gynecology, where women constitute the majority of the faculty workforce.
Footnotes
Authors' Contributions
All authors made substantial contributions to the conception or design of the work; or the acquisition, analysis, or interpretation of data for the work; and all authors contributed to drafting the work or revising it critically for important intellectual content; and all authors gave final approval of the version to be published; and all authors agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Author Disclosure Statement
R.J. has stock options as compensation for her advisory board role in Equity Quotient, a company that evaluates culture in health care companies; she has received personal fees from the NIH as a special government employee (in her role as a member of the Advisory Committee for Research on Women's Health), the Greenwall Foundation, and the Doris Duke Charitable Foundation. She has received grants for unrelated work from the NIH, the Doris Duke Foundation, the Greenwall Foundation, the Komen Foundation, and Blue Cross Blue Shield of Michigan for the Michigan Radiation Oncology Quality Consortium. She had a contract to conduct an investigator-initiated study with Genentech. She has served as an expert witness for Sherinian and Hasso, Dressman Benzinger LaVelle, and Kleinbard LLC. Authors C.B., C.B.R., K.A.G., and T.R.B.J. have no conflicts to report. Outside of this work, C.M. is supported by several grants, including the National Institutes of Mental Health (R01MH112420), Genentech Charitable Giving (G-80078), the Doris Duke Charitable Foundation (Grant 2015211), Weston Haven Foundation, United Health Group, and the California Health Care Foundation.
Funding Information
This study was not funded.