
Abstract
Background:
Women with a history of preterm delivery (PTD) have significantly increased risk of experiencing cardiovascular disease (CVD) later in life. However, the risk of long-term recurrence of CVD in this population remains unknown.
Materials and Methods:
The study was based on a cohort of Victorian women who had a singleton birth between 1999 and 2008. The primary outcome was a CVD event resulting in an Emergency Department visit/hospitalization or death. Women who do not have a PTD during the study period were adopted as the comparator. The Andersen and Gill model, which generalizes the Cox proportional hazards regression model, was used for the analysis of recurrent CVD, while adjusting for covariates, including indigenous status.
Results:
After excluding cases not meeting the inclusion criteria, 34,128 Victoria women who had a history of PTD and 374,538 women who had deliveries at terms were analyzed. A history of PTD was shown to be associated with significantly increased risk of recurrent CVD, while adjusting for all covariates, including indigenous status, with an adjusted hazard ratio (aHR) of 1.70 (95% confidence interval [CI]: 1.54–1.86, p < 0.0001). Aboriginal and Torres Strait Islander women had substantially increased risk of experiencing recurrent CVD after birth over their lifetime (aHR: 3.22, 95% CI: 2.39–4.35, p < 0.0001).
Conclusions:
Recognizing PTD as a nontraditional risk factor of CVD may play a role in the formulation of care plans for primary and secondary CVD prevention in women with such a history.
Introduction
Preterm birth (preterm delivery or PTD), a serious pregnancy complication, is associated with substantial perinatal morbidity and mortality affecting 5%–18% of deliveries worldwide. 1,2 In 2016, the rate of PTD in Australia was 8.6%. 3 Emerging evidence has demonstrated that link between history of PTD and future maternal risk of developing cardiovascular disease (CVD), analogous to other pregnancy-related complications like preeclampsia and gestational diabetes. A systematic review that synthesized evidence from 10 cohort studies related to spontaneous PTD and the risk of CVD revealed that women with a history of spontaneous PTD have a significantly increased risk of CVD (hazard ratio [HR]: 2.01, 95% confidence interval [CI]: 1.52–2.65). 4 Such risk is further increased with the reduction in gestation weeks at birth.
Remarkable declines in the mortality associated with heart disease have been achieved for both men and women over the past three decades; however, improvements for younger women (<55 years) have stagnated. 5 Traditional CVD risk factors combined with their differential impact in women and the emerging nontraditional risk factors unique to or more prevalent in women contribute to a new understanding of mechanisms leading to these worsening outcomes for women. Recognizing the unique CVD risk profiles in women, the American Heart Association's clinical guidelines for preventing CVD in women recommend a woman's history of PTD to be considered when assessing their CVD risk. 6,7
The economic burden of CVD attributed to women with a history of PTD has been quantified to assist with resource allocation and policy decision-making. It was estimated that over the next 50 years, 66% of women with a history of PTD would experience a CVD event and incur A$11 billion costs to the Australian health care system. The projection in this study emphasized the significance of recognizing PTD as a CVD risk factor and of primary CVD prevention programs that alter the risk of CVD. 8
A state-level, population-based longitudinal study (1994–2011) of women in New South Wales (NSW), Australia, was conducted to examine the relationship of PTD and maternal CVD risk. It was found that the association between PTD and future incidence of maternal CVD was not dependent on maternal smoking history during pregnancy. 9 However, this study did not adjust for indigenous status, despite the fact that CVD risk is inherently higher than among nonindigenous people. 10 Further, the long-term recurrence of CVD in women with a history of PTD remains unknown. Identifying the risk of de novo and recurrent CVD risk in this population could highlight the importance of both primary (i.e., people at risk of CVD) and secondary prevention (i.e., people with established CVD) in improving health outcomes for young women.
Materials and Methods
Study population and data sources
The study was based on a cohort of Victorian women who had a singleton birth between 1999 and 2008 to allow a minimum of 10-year follow-up for each woman (up until December 31, 2019). Women who died before the commencement of follow-up had a CVD event before or during their first birth, or had a CVD event within the same year of birth were also excluded. The first birth during the study period was used as the index birth for all women (with and without PTD).
Four datasets were linked for the study: (1) the Victorian Perinatal Data Collection (VPDC) (birth data 1999–2008)—a population-based surveillance system that collects comprehensive information on the health of mothers and babies, including obstetric conditions, procedures, and outcomes, neonatal morbidity, and congenital anomalies relating to every birth in Victoria; (2) the Victorian Death Index (VDI) (1993–2019), which includes all deaths in Victoria by cause of death and is administered by the Victorian Registrar of Births, Deaths, and Marriages (Department of Justice); (3) the Victorian Admitted Episodes Dataset (1993–2019), which comprises demographic, clinical, and administrative details of every admitted episode of care in Victorian public and private hospitals, coded according to the International Classification of Diseases, 10th revision, Australian Modification (ICD-10-AM) 7th Edition; and (4) the Victorian Emergency Minimum Dataset (2000–2019), which contains administrative and clinical data that detail all presentations to all Victorian public hospital Emergency Departments.
Records across the four datasets were linked both cross-sectionally (e.g., birth to hospital records) and longitudinally to the mothers' subsequent hospitalization or death records to create complete obstetric and medical histories. The linkage was undertaken by the Research Service and Data Integration team under Victorian Data Linkages, which is a state node of the Population Health Research Network.
Exposure variable (PTD)
Gestational age was based on the best clinical estimate using ultrasound examination or the last menstruation period extracted from the VPDC. Preterm birth was defined as any birth before 37 completed gestational weeks and was categorized according to severity (late [35–36 weeks]; moderate [33–34 weeks]; and extreme [20–32 weeks]). 11 Spontaneous (including preterm premature rupture of membranes) and indicated (including caesarean delivery) PTD were separately documented. Women with at least one PTD (≥1) were identified and included in the following analysis. Multiple PTD (women with more than one PTD during the study period) were recorded.
Data pertaining to age, race/ethnicity, maternal country of birth, and other pregnancy complications (e.g., gestational diabetes and hypertension), method of birth, number of births and pregnancies, and birth weight of the infant were identified from birth data.
Women who did not have a history of PTD during the study period were adopted as the comparator.
Outcome of interest
The primary outcome was defined as a recurrence of a CVD event, including Emergency Department (ED) visit/hospitalization or death from any CVD (not in the same year of the index birth). A hospitalization/ED visit for CVD was identified using diagnosis and procedure fields in the hospital records (ICD-10-AM codes: I20–I25 or revascularization procedure), the coronary heart disease (CHD) subgroup—myocardial infarction (ICD-10-AM codes: I21, I22, and I25.2), cerebrovascular events (ICD-10-AM codes: I60–I66; I67.0–I67.2; I67.4–I67.9; I68.1, I68.2, I68.8, I69, G46, G45.0-G45.2, G45.4, G45.8, and G45.9), congestive heart failure (ICD-10-AM code: I50), and atrial fibrillation (ICD-10-AM code: I48), while deaths from CVD as the underlying cause were ascertained from the VDI.
Major subtypes of CVD (i.e., stroke, transient ischemic attack (TIA), and CHD) were adopted as the secondary outcomes. Baseline demographic and clinical characteristics of women who ever had or never had a PTD were compared using t-test and Chi-square statistics.
Covariates
Covariates were derived from birth and hospital data, including labor type (spontaneous or indicated), obstetric complications (pregestational diabetes or gestational diabetes, preexisting and gestational hypertension), demographic characteristics (maternal age at the birth, country of birth, race/ethnicity, and indigenous background).
Statistical analysis
Recurrent time-to-event analysis
The data were set up using the Andersen and Gill model, which generalizes the Cox proportional hazards model that is formulated in terms of increments in the number of events along the time line. 12 The Anderson and Gill model assumes the correlation between subsequent event times for a given person can be accounted for by the past event, which suggests that the time increments between events are conditionally uncorrelated given the covariates.
For a subject, each event has one observation within the dataset. The first observation covers the time span from the time of the first PTD until the time of the first CVD event and then the second observation spans the time from the first event to the end of follow-up or the time of the next event. The follow-up started on the date of the index birth and ended on December 31, 2019, or on the date of death.
PTD was also coded according to the severity of PTD to explore the “dose–response” of PTD on the maternal risk of CVD. The total number of PTDs over the follow-up period was also examined. To construct the multivariate model, Chi-square test was used to investigate the difference in categorical variables, and t-test was employed to ascertain the difference in continuous variables between women with and without CVD, followed by univariate analysis using Cox proportional hazard models to identify significant covariates. Interaction terms were examined in the multivariable Cox proportional hazard models for statistical interaction between maternal age and history of PTD, and indigenous status and history of PTD. If the interaction term was not significant in modifying the results of the model without such a term, it was then excluded from the multivariable Cox proportional hazard model.
Further, a subgroup analysis was undertaken in women with spontaneous PTD (in contrast to medically indicated PTD). Models were adjusted for the same covariates in the subgroup analysis, and p-values will be calculated, with p < 0.05 considered significant. Stata SE 16.0 software (StataCorp., 2019, Stata Statistical Software: Release 16, College Station, TX: StataCorp LLC) was used for all analyses.
Time to first CVD event analysis
The Cox proportional hazard model adjusted for the same covariates was employed to analyze the time to the first CVD and/or time to CVD caused death. HR for the maternal first occurrence of any CVD by the history of PTD (Y/N) was reported. Moreover, time to the subtype of CVD (i.e., secondary outcomes), which comprises first events of CVD subgroup (i.e., time to first CHD, time to first TIA, and time to first stroke where a sufficient number of events allows for such analysis), was examined sequentially using the same analytic model.
Results
Study population
The linkage data were provided by Victorian Data Linkage Centre on March 10, 2020. In total, there were 409,046 women with a history of singleton births in Victoria between 1999 and 2008. After excluding cases not meeting the inclusion criteria, 34,128 women who had a history of one or more PTD and 374,538 women who did not have any PTD during the study period (Fig. 1) formed the dataset for the analysis. The median age of women at the index birth was 31 years in both PTD and term birth cohorts. The majority of women only had a single birth over the study period. Generally, over 75% of the women were born in Australia, and 1.4% or 0.7% of women in both cohorts were Aboriginal or Torres Islanders (Table 1).
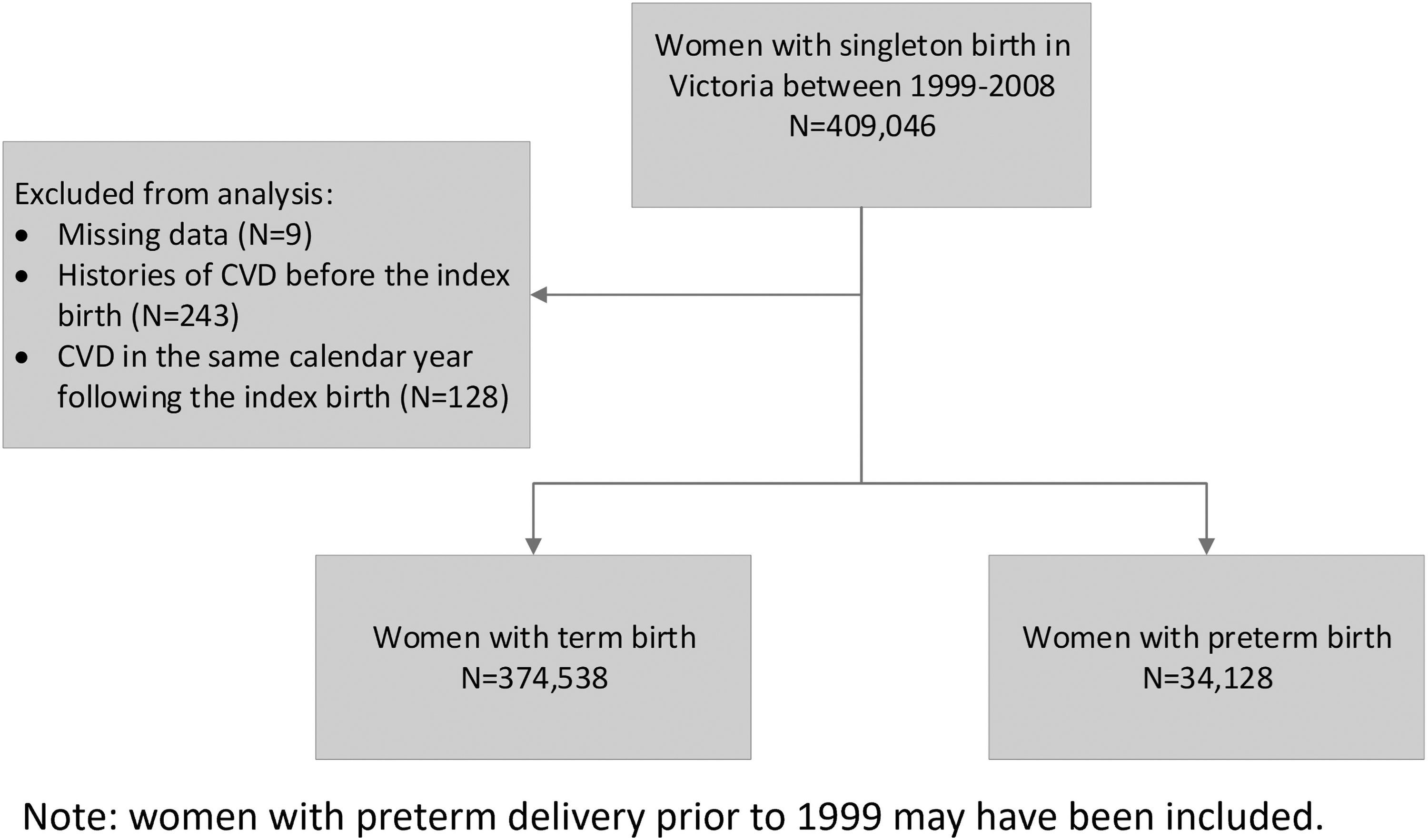
Flowchart of selection of women for the analysis. CVD, cardiovascular disease.
Baseline Characteristics of Indigenous and Nonindigenous Australian Women
Bold values indicate significant of p < 0.00001.
Indicates the between-group difference is significant (p < 0.05).
One women with an unspecified method of birth in the PTD group and three women with an unspecified method of birth in the term delivery group.
IQR, interquartile range; NZ, New Zealand; PTD, preterm delivery; SD, standard deviation.
Of the 34,128 women with a history of PTD, the median gestational age was 35 weeks (interquartile range [IQR]: 33–36 weeks). Around 43.7% of PTDs were spontaneous and 40.5% had a caesarean delivery. The mean birth weight of preterm newborns was 2,316 g (standard deviation [SD]: 796). In comparison, for 374,538 women with term deliveries, the median gestation age was 40 weeks (IQR 39–40 weeks); only 35.8% of them had spontaneous labor, 26.6% delivered the baby by caesarean, and the mean birth weight of term infants was 3 446 g (SD: 477). The maternal and pregnancy characteristics for the index birth are summarized in Table 1.
Of the pregnancy-related comorbidities, there were 6.3% and 4.6% having gestational diabetes, and 12.4% and 3.1% experiencing gestational hypertension in preterm and term, respectively. The characteristics of the study population are summarized in Table 1.
Recurrent CVD
Of the minimal 10-year follow-up (the maximal follow-up was 20 years), 4.4% and 2.25% of women from the preterm birth and term birth cohorts experienced recurrent CVD. The median time to the first recurrent CVD was 1.3 (IQR: 0.1–6.3) versus 1.5 (IQR: 0.1–7.8) years in the PTD and term delivery women.
Of 911 women in the PTD cohort who had CVD, 15.1% had a second CVD event, 6.1% had a third, and 4.6% experienced more than five CVD events during the entire follow-up period. The majority of CVD events was CHD (N = 729), followed by cerebrovascular disease (including both stroke and TIA, N = 498), heart failure (N = 174), and atrial fibrillation (N = 102). In comparison, among 5,888 women in the term delivery cohort who experienced CVD, 15.3% had a second event, 4.9% had a third, and 2.2% had more than five events during the same time, with CHD being the dominant type too (N = 3,740) (Table 2).
Characteristics of the Cardiovascular Events
CHD, coronary heart disease; CI, confidence interval; CVD, cardiovascular disease; IQR, interquartile range; MI, myocardial infarct; TIA, transient ischemic attack.
The survival analysis for the recurrent CVD revealed that a history of PTD is associated with a significantly increased risk of recurrent CVD, while adjusting for all covariates, including indigenous status, with an adjusted hazard ratio (aHR) of 1.70 (95% CI: 1.54–1.86, p < 0.0001). The aHR (1.72, 95% CI: 1.56–1.88, p < 0.0001) further increased when women's indigenous status was not adjusted for (Supplementary Table S1). Moreover, Aboriginal and Torres Strait Islander women had a substantially increased risk of experiencing recurrent CVD after birth over their lifetime (aHR: 3.22, 95% CI: 2.39–4.35, p < 0.0001). Pre-existing hypertension and diabetes, and pregnancy-related complications (i.e., gestational diabetes and hypertension) also positively correlated to the higher occurrence of repeated CVD events (Table 3). Results from univariate Cox proportional hazard model for recurrent CVD are shown in Supplementary Table S9.
Results from Multivariate Cox Proportional Hazard Model for Recurrent Events
Note: With cluster (ID). The model with cluster ID generates the narrower CI for the HR, while the point estimate is very similar. A total of 413,264 observations adjusted for 408,607 clusters by unique ID.
HR, hazard ratio; SE, standard error; Y, yes.
When the PTD was classified according to severity (i.e., ≥35, 33–35, 20–33 weeks), it showed that there was a trend toward increased risk of recurrent CVD with greater severity of PTD (i.e., the earlier the PTD) (Table 4).
Results from Multivariate Cox Proportional Hazard Model for Recurrent Event According to the Severity of Preterm Delivery
Women without preterm delivery history was the reference group. A total of 413,264 observations adjusted for 408,607 clusters by unique ID.
The increasing number of PTDs over the study period was also positively correlated with greater risk of recurrent CVD, suggesting women with ≥3 PTD exposures experienced the highest risk of recurrent CVD (Supplementary Table S2).
In the subgroup analysis restricted to women with spontaneous labor, when controlled for the same set of covariates, the risk of recurrent CVD associated with PTD was slightly reduced, but continued to be significantly higher compared with women without a history of PTD (Supplementary Table S3).
First-ever CVD
The characteristics of first-ever CVD events are shown in Table 2. The median time to the first-ever CVD event was 9.7 (IQR: 6.1–13.7) and 10.9 (IQR: 6.8–14.7) years, respectively, in the PTD and term delivery cohorts. Similarly, women with a history of PTD were more likely to develop CVD early in their life. Adjusting for the same covariates, a history of PTD was correlated with significantly greater risk of first-ever CVD, resulting in an aHR of 1.59 (95% CI: 1.46–1.73, p < 0.0001). Cerebrovascular disease was the main type of CVD event followed by CHD; together these two disease categories accounted for over 83% of all CVD events. All the covariates, including indigenous status, were also associated with an increased risk of having CVD later in maternal life (Table 5). The results by adjusting the labor type are shown in Supplementary Table S4.
Results of Multivariate Cox Proportional Hazard Model for the First-Ever Cardiovascular Event
Results based on 408,760 unique ID.
Time to first-ever CVD by type
Consistent with the aggregated analysis, the time to first-ever CVD event by type also yielded similar results, with all suggesting a history of PTD was associated with increased risk of each type of CVD. Among these, it seems that a history of PTD confers the highest risk for stroke with an estimated aHR of 1.79 (95% CI: 1.53–2.11, p < 0.0001). Of note, indigenous status was not identified as a significant covariate for the increased risk of both stroke and TIA, but remained a significant risk for the first occurrence of CHD (aHR: 3.53, 95% CI: 2.63–4.72, p < 0.0001) (Supplementary Tables S5 to S7).
Overall survival
A history of PTD confers an increased risk of overall mortality resulting in an aHR of 1.94 (95% CI: 1.74–2.16, p < 0.0001). Aboriginal and Torres Strait Islander women also had a higher risk of mortality after birth (aHR: 2.90, 95% CI: 2.17–3.89, p < 0.0001); comorbidity with diabetes before the index birth was associated with significant risk of overall mortality (aHR: 2.68, 95% CI: 1.98–3.63, p < 0.0001) (Supplementary Table S8). The Kaplan–Meier curves for the overall survival by delivery status (term vs. preterm) and by indigenous status are presented in Figures 2 and 3, both indicating significant between-group differences (log-rank test, p < 0.0001).
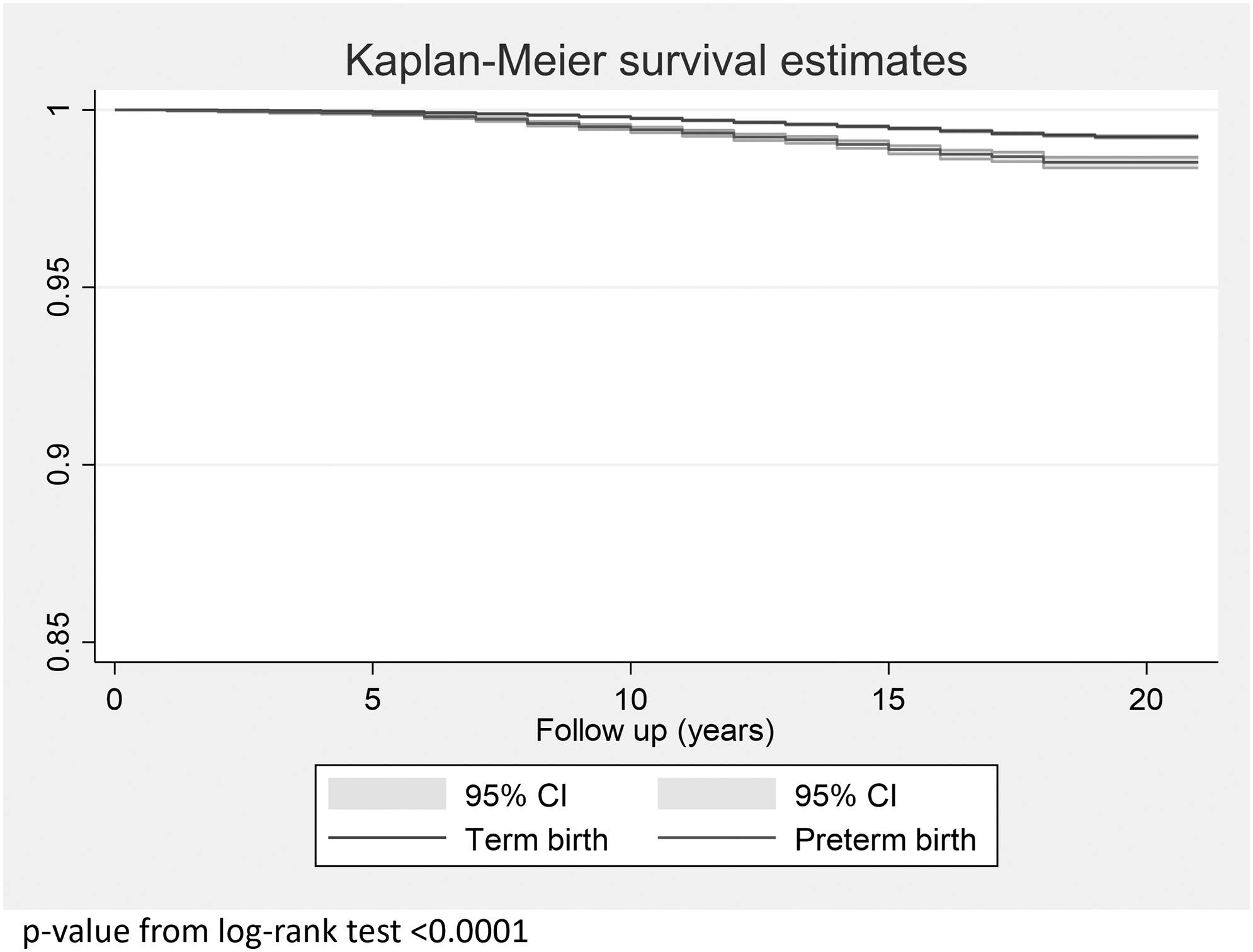
Kaplan–Meier survival curve for overall survival. CI, confidence interval.

Kaplan–Meier survival curve for the overall survival by indigenous status.
Discussion
CVD can occur more than once in a person's lifetime. However, so far, all the analyses concerning the association between history of PTD and maternal risk of CVD have only focused on the time to the first CVD event, largely overlooking subsequent events. Ascertaining the increased risk of the first-ever CVD in this population carries significant implications for CVD primary prevention, while deciphering the relationship of PTD with recurrent CVD also offers potential for secondary prevention of CVD.
The results from this large population-based study showed that women with a history of PTD are associated with significantly increased risk of recurrent CVD, with an aHR of 1.70 (95% CI: 1.54–1.86, p < 0.0001) adjusted for indigenous status, labor type, pregnancy-related complications, and pre-existing comorbidities. In addition, a history of PTD also confers an increased risk of overall mortality resulting in an aHR of 1.94 (95% CI: 1.74–2.16, p < 0.0001).
CVD is a primary cause of morbidity and mortality in Aboriginal and Torres Strait Islander people. Despite large reductions in age-standardized CVD mortality (40%) over the past few decades, CVD still accounts for ∼25% of Aboriginal and Torres Strat Islander deaths overall and 21% of all life years lost due to premature death. Indigenous persons are more likely to experience CVD earlier, about 10–20 years, than nonindigenous Australians. Our study was the first to include this cohort and to adjust for it in the survival analysis to estimate the increased risk of CVD in relation to the history of PTD.
Consistent with previous studies, our study found that indigenous young women had substantially increased risk of recurrent CVD, first-ever CVD, and all-cause mortality, compared to their nonindigenous counterparts in Australia. However, the current clinical recommendations for assessing the CVD risk in indigenous women do not detail consideration of nontraditional CVD risk factors, including the history of PTD. 10 Therefore, the results from this study again support the consideration of PTD in assessing the risk of CVD in indigenous young women.
The results from this study are well aligned with previous cohort studies that examined the association between PTD and de novo CVD. 13 A systematic review examined the relationship between spontaneous PTD and future maternal risk of CVD; it revealed that the PTD was linked to increased risk of overall CVD (HR: 2.01, 95% CI: 1.52–2.65), 4 stroke (HR: 1.71, 95% CI: 1.53–1.91), and ischemic heart disease (HR: 1.38, 95% CI: 1.38–1.57). An Israel-based study with more than a 10-year follow-up also reported that PTD contributed to greater risk of CVD-related hospitalizations (HR: 1.4, 95% CI: 1.2–1.6). 14
An Australian study from a single state-level data (NSW) using data from 1994 to 2011 (median follow-up 7.5 years, IQR: 3.0–13.0 years) found that PTD was correlated with an increased risk of all CVDs, reporting an HR of 1.78 (95% CI: 1.61–1.96). 9 Our study also showed that medically indicated PTD is associated with a higher risk of later maternal recurrent CVD compared to spontaneous PTD, which is consistent with the study that focused on the first-time CVD. 15 Of women with a history of medically indicated PTD in our study population, they are more likely to be older, be comorbid with hypertension and/or diabetes, and experience pregnancy-related complications (all with p < 0.0001).
The mechanism underlying the relationship between PTD and maternal CVD has not been clearly illuminated. The primary mechanisms may involve inflammation, infection, and vascular disease. 16 –18 The main theory is that PTD is related to future maternal CVD through some shared biological antecedents or inflammatory processes resulting in the formation of atherosclerosis. 16,19
Inflammation is one of the key factors in the development of atherosclerosis, from the initial lesion to the progression resulting in thrombotic complications. 20 Indeed, the traditional cardiovascular risk factors of hypertension and diabetes are more prevalent in women with a history of preterm birth. 21,22 The characteristics of our study population also uncovered the similar pattern showing that women with a history of PTD are more likely to have pre-existing diabetes and hypertension. When examining the risk of developing CVD in women with a history of PTD, these two pre-existing comorbidities were controlled for, which attenuated the HR ratio to a certain extent.
Our study not only affirmed the increased risk of first-ever CVD associated with a history of PTD but also revealed that PTD contributed to the increased recurrence of CVD events and the short time interval of the first recurrent event (median time of 1.3 years for women with a history of PTD). These findings bear significant implications for clinical practice: the recognition of history of PTD as an independent CVD risk factor improves the awareness of CVD risk profiles and facilitates a more comprehensive formulation of the management plan for both primary and secondary preventions.
This study has two key strengths: first, it is based on a large population-based administrative linkage dataset spanning over 20 years. Through the data linkage across four administrative datasets, all women residing in Victoria, who delivered an infant during the period 1998 to 2008 were included and the minimal follow-up was 10 years. It identified all women with a history of preterm birth for analysis, thus providing a more complete ascertainment of exposure and more reliable estimate of the associations. Second, the Cox proportional hazard regression analysis was adjusted for potential confounders related to CVD including indigenous status, labor type, pre-existing comorbidities, and pregnancy-related complications.
However, this study is not without limitations. First of all, the datasets were only linked for Victoria. In case of women relocating to another state or country during the study period, the follow-up events may have not been captured in the analysis. Second, the occurrence of CVD events outside of the hospital setting was not included (e.g., when a woman was treated only in the primary care setting). However, there is no evidence to suggest there would be significant differences in CVD ascertainment in both term and preterm delivery cohorts. Finally, other traditional CVD risk factors, including blood pressure, lipoprotein, and body mass index, were not captured in this dataset. However, there is no evidence to establish women with a history of PTD are more likely to be positive to these risk factors.
Conclusions
This study found that PTD is an independent risk factor for recurrent CVD events over a minimal 10-year follow-up in women with a history of PTD. Adjusting for women's indigenous status attenuates the increased risk of recurrent CVD to some extent. Recognizing PTD as a nontraditional risk factor of CVD may potentially play a role in the formulation of care plans for both primary and secondary CVD prevention in women with such a history. Future study to quantify the magnitude of PTD in modifying the CVD risk profile and ascertaining the effectiveness of lifestyle interventions in lessening the risk of CVD in this population is required.
Footnotes
Ethics Statement
This study was reviewed and approved by Deakin University Human Research Ethics Committee (2018-048).
Acknowledgments
Authors would like to acknowledge the Centre for Victorian Data Linkage, Department of Health and Human Services for the support to this work. Authors are grateful to the Consultative Council on Obstetric and Pediatric Mortality and Morbidity (CCOPMM) for providing access to the de-identified data used for this research project and for the assistance of the staff at the Consultative Council's Unit, Safer Care Victoria. The conclusions, findings, opinions, and views or recommendations expressed in this article are strictly those of the authors. They do not necessary reflect those of CCOPMM.
Authors' Contributions
L.G. and M.M. conceived the study. L.G. and S.J.B. undertook the analysis. L.G. drafted the article. M.M. and S.J.B. provided important intellectual inputs for the revision.
Author Disclosure Statement
All authors confirm there is nothing to declare.
Funding Information
No funding was received for this study.
Supplementary Material
Supplementary Table S1
Supplementary Table S2
Supplementary Table S3
Supplementary Table S4
Supplementary Table S5
Supplementary Table S6
Supplementary Table S7
Supplementary Table S8
Supplementary Table S9
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.