
Abstract
Cervical cancer is highly preventable when precancerous lesions are detected early and appropriately managed. However, the complexity of and frequent updates to existing evidence-based clinical guidelines make it challenging for clinicians to stay abreast of the latest recommendations. In addition, limited availability and accessibility to information technology (IT) decision supports make it difficult for groups who are medically underserved to receive screening or receive the appropriate follow-up care. The Centers for Disease Control and Prevention (CDC), Division of Cancer Prevention and Control (DCPC), is leading a multiyear initiative to develop computer-interpretable (“computable”) version of already existing evidence-based guidelines to support clinician awareness and adoption of the most up-to-date cervical cancer screening and management guidelines. DCPC is collaborating with the MITRE Corporation, leading scientists from the National Cancer Institute, and other CDC subject matter experts to translate existing narrative guidelines into computable format and develop clinical decision support tools for integration into health IT systems such as electronic health records with the ultimate goal of improving patient outcomes and decreasing disparities in cervical cancer outcomes among populations that are medically underserved. This initiative meets the challenges and opportunities highlighted by the President's Cancer Panel and the President's Cancer Moonshot 2.0 to nearly eliminate cervical cancer.
Background
Cervical cancer is highly preventable when precancerous lesions are detected early and treated according to the latest evidence-based guidance, but it continues to be a significant public health concern. 1 Each year in the United States, about 13,000 new cervical cancers are diagnosed and >4000 people die from this disease. 2 The number of high-grade cervical precancer cases is estimated to be much higher, with one study indicating it could be close to 200,000 per year. 3 Adherence to evidence-based screening and management guidelines enhances the likelihood that harms are minimized throughout the screening process. 4,5
Clinicians can provide appropriate care by staying abreast of the latest updates to the cervical cancer screening and management (CCSM) guidelines. 6 The existing screening guidelines for cervical cancer, which are written in narrative form, include guidelines for average-risk and high-risk populations. 1,7 The management guidelines were revised to use a risk-based approach and are expected to be evaluated on a regular basis. 5 Applying the management guidelines takes time; it requires clinicians to consider the patient's previous screening results and other relevant medical history. 5
Finding and properly collating this information in the electronic health record (EHR) takes time that could be spent on other aspects of patient care. Primary care clinicians already devote significant time to stay up-to-date with the latest evidence. 8,9 One analysis indicated that keeping current with the volume of medical literature relevant to primary care would require several hundreds of hours every month. 8 By transforming CCSM narrative guidelines into a computable format and making them available as clinical decision support (CDS) tools, guidelines can be integrated with EHR platforms in a vendor-neutral 10,11 manner that can assist clinicians with improving patient outcomes. 12
Cervical Cancer Guidelines at Point of Care
The Centers for Disease Control and Prevention (CDC), Division of Cancer Prevention and Control (DCPC) in partnership with the Health federally funded research and development center (FFRDC), operated by the MITRE Corporation, is leading a multiyear initiative to develop computer-interpretable (“computable”) guidelines to support clinician awareness and adoption of the most up-to-date CCSM guidelines (Fig. 1). Computable guidelines provide a means of creating a computable representation of narrative clinical guidelines. Our initiative aims to address the challenges and opportunities highlighted by the President's Cancer Panel and the President's Cancer Moonshot 2.0 to nearly eliminate cervical cancer by focusing on improved screening and treatment to those of highest risk. 13,14 Trim this sentence to: The CDS tools are designed to help clinicians more efficiently evaluate patient clinical data against CCSM guidance and display patient-specific recommendations. 15
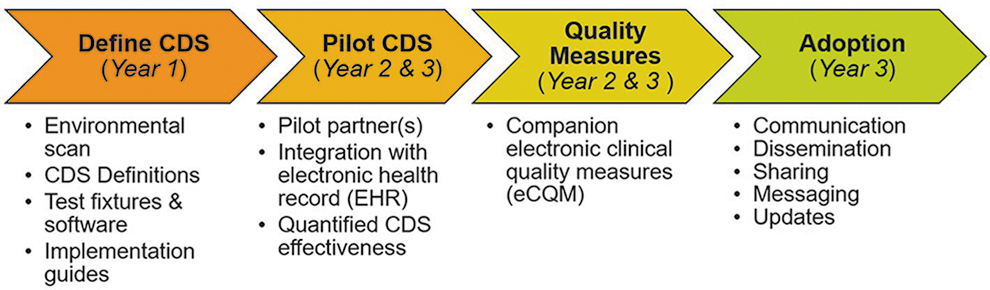
Project timeline. It depicts the project timeline and associated activities for the multiyear CCSM CDS initiative. The team has completed Year 1 activities and is currently in Year 2 of the 3-year effort. Define CDS (Year 1): conduct environmental scan, delineate CDS definitions, test fixtures and software, and produce implementation guide. Pilot CDS (Years 2 and 3): secure pilot partners, integrate with EHR, and evaluate CDS effectiveness. Quality Measures (Years 2 and 3): prototype companion electronic clinical quality measures. Adoption (Year 3): communicate, disseminate, message, and share project updates. CCSM, cervical cancer screening and management; CDS, clinical decision support; EHR, electronic health record.
U.S. data indicate that geographic, racial, and socioeconomic disparities exist for rates of cervical cancer screening, incidence, and mortality. 16 –18 The CDS tools have been created with the goal of increasing the quality of care available for all applicable patients, but especially for those who are medically underserved or are from under-resourced populations who are most likely to receive their care from primary care physicians rather than specialists, often at community health centers, rural settings, and safety net medical centers. 19,20 Primary care physicians may be less up-to-date than specialists on the complex details of how screening and follow-up recommendations vary by prior medical history. 5,8,9 The CDS tools can help equip primary care clinicians at the point of care with appropriate screening and management guidance for their patients.
By putting patient history, clinical guidelines, and care information right at the clinicians' fingertips, decision support reduces the manual workload of monitoring patients who need screening and potential follow-up. To the extent that clinicians working with underserved populations can use these tools effectively, we expect that the tools can improve existing disparities in screening and follow-up care. Most federally qualified health centers already use EHRs. 21,22 For those lacking EHRs, our CDS tools can be used in an offline mode similar to how the ASCCP mobile phone application operates. Designing evidenced-based CDS tools intended to specifically address disparities can be one way to improve equitable health outcomes. 23,24
CDC's Adapting Clinical Guidelines for the Digital Age initiative and the Agency for Healthcare Research and Quality's CDS Connect Platform support the development and implementation of CDS tools that operate across different EHR systems (i.e., tools that are interoperable). 25,26 These initiatives operate on the principle that when narrative and computable clinical practice guidelines are codeveloped, the computable representation reduces duplication of effort across the healthcare ecosystem and diminishes the chances for guideline misinterpretation. 25
As described hereunder in the section on interoperability, computable guidelines can subsequently be leveraged to efficiently develop CDS tools and companion electronic clinical quality measures (eCQMs). eCQMs are tools that help measure and track the quality of healthcare services using data extracted from an EHR. 27 –29
Primary Evidence Base
The CCSM CDS tools have been designed to represent two evidence-based primary guidelines: (1) the 2018 United States Preventive Services Task Force (USPSTF), recommendations for cervical cancer screening, and (2) the 2019 ASCCP Risk-Based Management Consensus Guidelines* for managing abnormal cervical cancer screening results. 1,5 Additional guidelines from medical societies were leveraged to fill gaps for high-risk populations that are not specifically addressed in the primary guidelines, which include patients with opportunistic infections, abnormal vaginal bleeding, and certain immunocompromised conditions. 7,30 –32
Although other evidence-based cervical cancer screening guidelines exist in the United States, the CDS tools are aligned with the USPSTF recommendations; differences include age thresholds and preferred screening methods.
33
The CCSM CDS tools were aligned with the USPSTF guidelines because the USPSTF guidelines are used: In the Patient Protection and Affordable Care Act as a source of recommended clinical preventive services for which most health insurance plans must provide in-network coverage without cost-sharing,
34
–36
As the basis for the cervical cancer screening quality measures used in the Centers for Medicare & Medicaid Services (CMS) quality reporting program, the Health Resources and Services Administration Uniform Data System and the National Committee for Quality Assurance (NCQA) Healthcare Effectiveness Data and Information Set (HEDIS),
27
–29,37
and For reimbursement by National Breast and Cervical Cancer Early Detection Program.
38,39
As for management guidelines, the CDS is aligned with ASCCP's risk-based management guidelines, which is the only evidence-based source available.
The science behind cervical cancer screening continues to evolve as human papilloma virus (HPV) vaccination coverage increases and further evidence of the value of primary HPV testing. 5 The CCSM computable guidelines and CDS tools are designed with adaptability in mind, so they are easier to update in the future.
Environmental Scan
The CDC-led team conducted an environmental scan to inform the translation of the CCSM guidelines into a computable representation as well as to guide the development of the CDS tools and companion eCQMs. 40 The environmental scan included the components shown in Figure 2 and considered CCSM guidelines, CCSM CDS tools currently in use, existing clinical workflows, patient needs and preferences, and which aspects of patient care could best be enhanced by CDS. The team conducted interviews with >20 expert groups and performed a literature review of >90 primary sources consisting of guidelines, standards, evidence-based research, and publicly available software.

Environmental scan components. The environmental scan included the eight components shown in Figure 2 and considered CCSM guidelines, CCSM CDS tools currently in use, existing clinical workflows, patient needs and preferences, and aspects of patient care that could best be enhanced by CDS: Evidence Review: Authoritative evidence for screening and management guidelines; Current Clinical Practices: Common ways CCSM are done today, and how the guidelines are currently followed in clinical practice; Patient Experiences: Experiences with respect to women's cervical health, and how can the patient experience be improved with CDS; EHR and Related Capabilities: CDS capabilities supported by EHRs today and any specific support for cervical cancer; Anatomic Pathology and LIS: Content and format of test results (e.g., Pap, HPV, and biopsy) as well as how LISs can integrate with EHRs; Information Standards: Interoperability standards for representing health information, pathology results, CDS and potential gaps; Quality Measures: Quality measures for screening or management of cervical cancer. HPV, human papilloma virus; LIS, Laboratory Information Systems.
Findings from the environmental scan showed opportunities to (1) increase awareness and understanding of the most recent CCSM guidelines, (2) support the workflows of clinicians and pathologists, and (3) address inequities in patient care. 40 Additional needs identified in the scan, particularly from the patient perspective, include the ability to facilitate shared decision-making and solicit patient preferences. 40 Patient preferences might include screening test type and screening interval, pregnancy considerations, and communication materials that consider primary language and learning style. Taking patient preferences into account is critical when developing CDS since it has been indicated that this can help establish patient trust. 41
Challenges
The primary medical informatics challenge the team identified from the environmental scan was that application of the ASCCP management guidelines requires access to cervical cytology, histology, and related pathology data to determine a patient's risk of precancer or cancer. 5 Cervical cytology pathology reports typically include only narrative text and are difficult to use with the National Cancer Institute risk tables that are at the core of the updated ASCCP management guidelines. 42,43 In an Anatomical Pathology and Laboratory Information System (AP-LIS), final diagnosis fields may be stored digitally as plain text and not encoded with any information that is easy for a computer algorithm to understand. 44,45 This can hinder efforts to build robust CDS tools that generate cervical precancer risk estimates based on patient data in the EHR.
Although some organizations have used Natural Language Processing (NLP) to automatically interpret pathology reports, the results are not easily generalizable across other health information technology (IT) systems because of local nonstandardized nomenclature used in pathology reports. 46,47 The current option available to most clinicians involves manually interpreting the pathology reports that are sent from the AP-LIS to EHRs. The extracted information can then be entered into a mobile phone application, which provides recommendations outside of the EHR. 48 If structured and discrete pathology data (i.e., diagnosis values come from a known and finite list) were readily available, then that information could be leveraged by CDS tools implemented from within the EHR.
This would be made possible through improved standards for capturing and transmitting the kinds of pathology data, which are known to be important for CCSM. 49 The College of American Pathologists maintains a set of electronic cancer checklists that are used to capture structured data for cancer reporting and staging 42,50 ; an analogous electronic checklist for cervical precancer is proposed to enable wider use of CCSM CDS tools and is one of the major long-term actions coming out of the environmental scan. 40
Although a cervical precancer checklist is not in wide use today, there are several short-term solutions available for those looking to apply the updated CCSM guidelines. As mentioned earlier, some organizations have developed NLP algorithms for automatically interpreting their pathology reports. 46,47 For these organizations, the CCSM CDS tools described in this article have been designed to interface directly with NLP. 15
For organizations without their own NLP capabilities, a structured data capture (SDC) form is included in the CCSM CDS so that clinicians can take the information they manually extract from pathology reports and manually enter it into the EHR. 15 Although manual entry is not ideal, an advantage with the CCSM CDS SDC form is that the information entered will be recorded and remain in the EHR eliminating the need for multiple entries. This would allow for efficiencies to be gained on subsequent follow-up visits with the same patient.
Another option for organizations without automated NLP interpretation of pathology data would be to work with their laboratory providers to implement the SMART Health Cards Framework. 51 Originally developed as part of the Vaccine Credential Initiative, a SMART Health Card is a digital or paper version of vaccination history or laboratory test results. 51,52 It typically takes the form of a Quick Response code and could be issued to the patient in lieu of or in addition to the traditional laboratory result narrative. A potential advantage of SMART Health Cards is that they can store structured and discrete information in a standard way that many EHRs can already process and understand. In addition, patients can carry with them and communicate their own data. 51,52
Interoperability
The CCSM CDS is expressed in a computer-interpretable format using health IT interoperability standards that helps address many of the challenges identified in the environmental scan. 15,53 Also important is for computable guidelines and CDS tools to be interoperable across different EHR platforms and Health IT systems. 11 The interoperability standards described in this section are used to define both the modular structure of the CCSM CDS as well as the computer logic needed to provide customized recommendations for each patient. Health IT systems that support these interoperability standards can more easily incorporate the CCSM CDS, especially when compared with developing their own capabilities from scratch. 53
Fast Healthcare Interoperability Resources (FHIR) is an international IT standard for representing and exchanging healthcare information electronically; it has been used to define the modular structure of the CCSM CDS. 54 FHIR provides general data structures or “resources” for representing a variety of clinical and healthcare-related data. 55 Example resource types include Condition and Observation, which can be used to represent clinical diagnoses and laboratory test results, respectively. 56,57 FHIR resources are, by design, general in nature so that they can support most real-world use cases. There are FHIR resources available for representing all the types of data required by the CCSM guidelines. 55
Clinical Quality Language (CQL) is a computer programming language focused on the expression of clinical quality concepts. 10 CQL has been used to define the computer logic of the CCSM CDS for several reasons. 53 First, it has been designed for authoring CDS logic and for interfacing directly with FHIR; this is an advantage over other more general-purpose programming languages, which, by definition, have not been designed to author CDS or to interface with FHIR. This is not to say FHIR-based CDS logic cannot be written using a general-purpose programming language, just that it can potentially be done more easily and naturally with CQL. An additional advantage is that CQL incorporates more natural language than other computer programming languages, meaning CDS logical expressions written with CQL may be more accessible to less technical audiences. Finally, much of the logic defined for the CDS can be reused for companion eCQMs, which may lead to increased efficiencies when the two are being codeveloped.
FHIR allows resources to be customized for specific applications; these customizations can themselves be standardized using FHIR extensions, profiles, and implementation guides. 58 The customizability and flexibility of FHIR are two of the reasons why it has been growing in popularity despite being a new standard. The use of FHIR in the United States is expected to grow because of these features and because it is the defined standard for the application programming interface (API) required by the 21st Century Cures Act Interoperability Final Rule. 59 The CCSM CDS models patient data with FHIR consistent with the Final Rule, which could ease the implementation burden for organizations whose EHRs comply with the 21st Century Cures Act.
CDS Design
The CDC-led team has developed CDS tools that have been designed to make it easier for clinicians to stay informed of evolving CCSM guidelines. 60 This is accomplished by leveraging patient data in the EHR and by linking it to appropriate CCSM recommendations. Data from the EHR is assumed to be accessed via a FHIR API (see the previous section) and recommendations are presented to clinicians from within an informational dashboard. To provide the necessary context, the CCSM dashboard also contains a summary of pertinent patient data, such as relevant 60
laboratory and pathology results (e.g., cervical cytology and histology, HPV tests),
medical history (e.g., cervical cancer or precancer and immunosuppression),
procedures (e.g., hysterectomy with or without removal of the cervix, colposcopy, and biopsies),
medications (e.g., immunosuppressive medications or treatment), and
demographics (e.g., age, gender, date of birth, race, ethnicity, and preferred language).
The CCSM CDS tools contain logic that determines for each patient: (1) what information should be displayed in the dashboard, (2) how that information should be displayed, (3) when screening is due, (4) what type of screening is indicated based on the patient's history, and (5) for the patient with abnormal screening results, whether they should undergo surveillance, colposcopy, or treatment. 60
Although the CCSM CDS tools are already freely available as open-source software, 50 their design is still evolving and will be further refined through several upcoming clinical pilots. Other options for potential future iterations include implementing patient-facing features, such as use of SMART 51 Health Cards (see “Challenges” section), patient printouts that explain their medical history in the context of their cervical precancer risk, references to online educational materials, and reminders for upcoming screening tests through the patient portal. An illustration of the conceptual workflow for the CDS is shown in Figure 3 .

Conceptual clinical workflow with CDS working in conjunction with EHR. It illustrates the workflow and interaction with the CCSM CDS in clinical setting: Patient information flow is shown in green. The Patient Health Portal represents patient-facing interactions with their health data, and could utilize web access, a mobile app, or messaging services. Clinician information flow is shown in blue. The clinician interacts with the CDS service, which queries the EHR server for patient data. Screening and treatment providers are shown in brown. These represent laboratory services, cancer specialists, surgeons, or other specialized care providers. The results of all health actions are recorded in the EHR server. These results can further inform the CDS service, other clinicians, and the patient health portal.
Clinical Pilots
The CCSM CDS is an effort to represent clinical guidelines in a shareable, structured, and computable format to facilitate meaningful improvements in the number of patients screened and treated for cervical precancer. This includes addressing current gaps in screening uptake and timely follow-up care among populations that are often medically underserved. 12 In the next phase of this effort, the team plans to pilot the CDS for CCSM in three clinical settings to test the feasibility of the CDS under real-world conditions. The purpose of the pilot is to ensure that the CDS as developed can be integrated with health IT systems and perform as expected. A select set of data can be collected pre- and postimplementation to help assess CDS usability and any observable differences in the types and rates of screening and management decisions.
To participate, prospective pilot partners are expected to support the technical integration of the CCSM CDS for a 6- to 8-month pilot. They must support specific health IT standards, such as FHIR, to facilitate integration. They are also expected to engage with the CDS development team to inform aspects of the CDS design and usability before a pilot go-live date. Clinicians at each of the three pilot sites intend to use the CCSM CDS with a diverse (e.g., race, ethnicity, and income) patient population that could benefit from the CDS. Selected pilot partners will represent a range of clinical settings, including safety net providers, community health centers, and potentially lower-resourced settings that care for uninsured and underinsured patient populations.
Conclusion
The multiyear initiative sponsored by the CDC's DCPC in partnership with the MITRE Health FFRDC and experts in cervical cancer guidelines and computable guidelines/CDS rises to the challenge presented in the President's Cancer Panel report 13 by creating IT that is intended to promote appropriate cancer risk assessment and screening. 61 By creating CDS tools expected to be effective, we are helping to nearly eliminate cervical cancer through a focus on more equitable screening and follow-up, specifically as part of President Biden's Cancer Moonshot revival. 14 The primary goals for this effort can be summarized as follows:
Develop an advanced CCSM CDS capability that is interoperable, shareable, and adaptable and make them accessible to community health centers and safety net providers who care for medically underserved populations.
Facilitate improvements in the number of individuals appropriately and equitably screened and treated for cervical precancer, paying particular attention to gaps in screening uptake and follow-up care for populations that are medically underserved.
Provide advanced cognitive support for clinicians, particularly primary care clinicians, to help them more easily apply up-to-date screening guidance and risk-based approach for managing abnormal results.
Promote use of computable guidelines and CDS as a means to close the equity gaps that exist in CCSM. 13
Inform and engage patients in shared decision-making.
Enable new insights for public health reporting and research.
Propose and pilot CDS tools that help with handling unstructured pathology data.
The CCSM CDS tools are intended as a pilot study for representing clinical guidelines in a structured and computable format. If every provider had the assistance of enhanced CCSM capabilities, it could make meaningful improvements in the number of individuals screened and treated for precancer. 35,46 Timely screening and follow-up could improve diagnosis, treatment, and follow-up management of cervical precancers (∼200,000 cases per year), reduce the number of individuals diagnosed with cervical cancer each year (>13,000 cases per year) and the number of deaths from this preventable malignancy (>4000 deaths per year). 2,3
Footnotes
Disclaimer
The term “computable guidelines” is industry language used to describe the translation of narrative clinical guidelines into computable form. These computable guidelines are based on existing guidelines and do not represent new formal guidance developed through CDC's own evidence-based process. The findings and conclusions in this report are those of the authors and do not necessarily represent the official position of the Centers for Disease Control and Prevention or the National Cancer Institute.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
The MITRE Healthcare Federally Funded Research and Development Center (FFRDC) receives support under Centers for Disease Control and Prevention (CDC) Cervical Cancer Computable Guidelines Contract No. 75FCMC18D0047, Project No. 37208168. The Health FFRDC is sponsored by the CMS on behalf of the Department of Health and Human Services (HHS). The Health FFRDC serves as an objective advisor to all HHS organizations and other federal agencies with HHS missions. MITRE works closely with CDC for long-term development needs, including in the area of electronic health interoperability are integration.