
Abstract
Background:
The validated SAMANTA questionnaire allows identification of women with heavy menstrual bleeding (HMB); that is, with excessive menstrual bleeding that interferes with quality of life (QoL). We assessed its value for monitoring HMB treatment in clinical practice.
Material and Methods:
This is a prospective observational study conducted between December 2018 and March 2021 in consecutively recruited women with HMB attending gynecologists' offices who started a hormonal treatment. Sociodemographic characteristics were recorded at enrollment. At baseline and month 12, we assessed the HMB (SAMANTA questionnaire), the global impression of menstrual bleeding severity in patients (PGI-S) and clinicians (CGI-S), and the QoL (SF36). At month 12, we assessed the global impression of menstrual bleeding change in patients (PGI-C) and clinicians (CGI-C). Changes in SAMANTA questionnaire score at month 12 were compared with the presence of amenorrhea and changes in blood loss, menstrual period duration, and PGI-S, PGI-C, CGI-S, and CGI-C.
Results:
The study included 371 women aged 41.2 ± 6.5 years, 87% of whom were using the levonorgestrel intrauterine system. The SAMANTA questionnaire score significantly decreased in 97.3% of women. The decrease was greater in women reporting a reduction in blood loss, shorter menstrual bleeding duration, or a strong improvement in menstrual bleeding severity (PGI-S and CGI-S) or amount (PGI-C and CGI-C) (p < 0.001 for all), but not amenorrhea. SF-36 domains improved significantly; changes being inversely associated with changes in the SAMANTA questionnaire score.
Conclusions:
The SAMANTA questionnaire seems a valuable tool for monitoring hormonal treatment for HMB.
ClinicalTrials.gov identifier NCT03751800.
Introduction
Heavy menstrual bleeding (HMB), which is defined as “excessive menstrual blood loss which interferes with a woman's physical, social, emotional and/or material quality of life (QoL),” 1 is a common gynecological problem in clinical practice. 1 It has been estimated that up to 30% of women of reproductive age suffer from HMB, 2 although the prevalence is difficult to establish given the lack of uniformity across studies with respect to the assessment methods. 3 The prevalence of HMB increases with age, 2 and it is frequently associated with iron deficiency anemia, 4 whose consequences further undermine the woman's QoL. 5
Several quantitative, semiquantitative, and qualitative methods have been developed to assess the amount of menstrual blood loss. 3,6 However, these methods are complex and difficult to use in clinical practice. 3 Moreover, they do not take into account the effect of excessive menstrual bleeding (EMB) on women's QoL. 3,7 In light of this, other questionnaires have been developed to address both the clinical aspect of EMB and its impact on QoL. 3
These include the recently developed SAMANTA questionnaire, an easy-to-use six-item questionnaire for identifying EMB that interferes with QoL. 8 It has shown a sensitivity of 86.7% and a specificity of 89.5% when using a score of ≥100 in the semiquantitative method “Pictorial blood loss assessment chart” as a reference. 9 The SAMANTA questionnaire has shown a strong correlation with the perceived intensity of menstrual bleeding and its impact on activities of daily living as measured by visual analog scales (VAS) and validated QoL measures such as the EuroQoL five dimensions, five levels questionnaire (EQ-5D-5L), and the Psychological General Well-Being Index. 8
The aim of treatment for HMB is to improve both the blood loss and the QoL. 1,10 Given that both are assessed by the SAMANTA questionnaire, we explored the value of this questionnaire as a follow-up tool in women treated for their HMB. For this purpose, we conducted a prospective observational cohort study where we analyzed the sensitivity of the SAMANTA questionnaire to detect changes in HMB after 1 year of treatment in women with benign HMB receiving long-term hormonal treatment according to routine clinical practice.
Material and Methods
Study design
This was an observational, prospective, multicenter, noninterventional cohort study conducted in consecutively recruited women attending gynecologists' offices in Spain. The inclusion criteria included being >18 years and of childbearing age, not intending to become pregnant during the next year, having a diagnosis of HMB or idiopathic menorrhagia according to medical criteria and based on clinical judgment, and having freely chosen a long-term hormonal treatment for HMB licensed in Spain (Mirena® 20 μg levonorgestrel/24 hours intrauterine delivery system [LNG-IUS], Bayer AG; Qlaira®, estradiol valerate/dienogest, Bayer AG; or Progevera®, 10 mg medroxyprogesterone acetate, Pfizer Inc.).
The exclusion criteria included presenting contraindications or warnings for the use of long-term hormonal treatment prescribed for HMB per the summary of product characteristics, amenorrhea or menopause, degenerative diseases with an impact on daily life or psychiatric disorders preventing the patient from making decisions and following instructions, history of malignancy, receiving contraceptive hormonal therapy, using a copper intrauterine device or being on hormone replacement therapy, taking concomitant medication with a potential effect on bleeding pattern, being pregnant or having given birth within the previous 6 months, or participating in an investigational program with interventions outside routine clinical practice. Women had to be able to understand the information provided.
Women were consecutively recruited during routine clinical practice. The study was conducted in two visits: the baseline visit and the 12-month final visit. The protocol was approved by the institutional review boards of all the participating hospitals, was approved by the Spanish Agency of Medicines and Medical Devices (AEMPS), and was conducted in compliance with the Declaration of Helsinki and the International Conference on Harmonization—Good Clinical Practice (ICH-GCP) guidelines. Written informed consent was obtained from all participants before entering the study.
Variables collected
Information collected at baseline included data on demography (age, place of birth, literacy level, and working status), gynecologic history (parity and previous contraceptive method used), menstrual bleeding during the last three periods (mean bleeding days and the amount of blood loss, subjectively graded as “very abundant,” “abundant,” “normal,” or “scarce”), and treatment started for HMB. Adverse events were recorded throughout the study. For women discontinuing the study, reasons for discontinuation were also collected.
Assessments at baseline included the SAMANTA questionnaire, patient and clinician global impression of menstrual bleeding severity (PGI-S and CGI-S, respectively), and QoL. The SAMANTA questionnaire is a six-item questionnaire that gathers information on the duration and quantity of menstrual bleeding, the bother and inconvenience caused by heavy blood loss, and the impact on daily activities.
It comprises the following questions: (1) Do you experience menstrual bleeding for >7 days per month? (2) Do you experience ≥3 days of heavier menstrual bleeding during your menstrual period? (3) In general, does menstruation bother you due to its abundance? (4) During any of these heavier menstrual bleeding days, do you spot your clothes at night; or would you spot them if you did not use double protection/did not change your clothes during the night? (5) During these heavier menstrual days, are you worried about staining the chair, sofa, etc.? (6) In general, during these heavier menstrual bleeding days, do you avoid, as far as possible, some activities, trips, or leisure-time plans because you frequently need to change your tampon or sanitary towel?
Affirmative answers to items 1 and 3 are assigned a score of 3 points each, while items 2, 4, 5, and 6 are assigned 1 point each. Negative answers are scored 0. The total score ranges from 0 to 10, with a score of ≥3 points being indicative of HMB. Currently, it is only validated in Spanish. 8 The PGI-S and CGI-S consisted of the same question (How would you rate the severity of menstrual bleeding in the last 3 months?) posed to the patient and the clinician (according to his/her judgment). The possible answers were severe, moderate, mild, or normal. The QoL was assessed by means of the Spanish validated version of the Short Form Health Survey Questionnaire (SF 36) v.2 instrument. 11
Assessments at the final visit (month 12) included the SAMANTA questionnaire, PGI-S and CGI-S, patient and clinician global impression of changes in the menstrual bleeding pattern (PGI-C and CGI-C, respectively), and QoL. PGI-C was assessed by asking the women and clinicians “Compared to the period before starting treatment for HMB, has the quantity of menstrual bleeding increased, remained the same, or decreased?”
The clinicians also explored the history of the menstrual bleeding pattern. For this purpose, the women were asked about the presence of amenorrhea in the last 3 months (yes/no). In women not experiencing amenorrhea, the mean duration of menstrual bleeding and the amount of blood loss (as in baseline) during the same period were investigated.
The SAMANTA questionnaire was also used in women having a nonmandatory interim follow-up visit 4–12 weeks after starting treatment.
Endpoints
The primary endpoint was sensitivity to change in the SAMANTA questionnaire. This was assessed by comparing the change from baseline in the SAMANTA questionnaire score and (i) the change in other HMB-related clinical measurements such as presence of amenorrhea, intensity of blood loss, and duration of menstrual period; and (ii) the change in patient and clinician global assessments (PGI-S, PGI-C, CGI-S, and CGI-C). The secondary endpoint was to assess the correlation between changes in SAMANTA questionnaire scores and changes in women's QoL as measured with SF36v.2 at month 12 of treatment or at premature discontinuation.
Sample size calculation
The sample was calculated with the aim of achieving enough precision in the estimation of a change in SAMANTA questionnaire score from baseline to the final visit. A sample size of 452 women was needed to estimate a 95% confidence interval (CI) with a precision of 0.12, assuming a typical deviation of 1.2 and a dropout rate of 15%.
Statistical analysis
Qualitative variables were analyzed as the number of cases and percentages, and quantitative variables as mean and standard deviation (SD), or median and quartiles Q1 and Q3. Normality was tested with the Kolmogorov–Smirnov test. From month 0 to month 12, changes in the SAMANTA questionnaire scores were categorized as “improvement” and “worsening” when a negative or positive change was observed, respectively.
Changes in the amount of menstrual bleeding according to the PGI-S and CGI-S during this period were categorized as “no change,” “mild/moderate/strong improvement” (for an increase of 1, 2, or 3 points, respectively), or “mild/moderate/strong worsening” (for a decrease of 1, 2, or 3 points, respectively). These seven levels were further classified into the following three categories: “no change,” “improvement,” or “worsening.” Qualitative variables were compared using the chi-square test or Fisher's exact test, as appropriate.
Quantitative variables were compared using parametric (t-Student's or analysis of variance [ANOVA]) or nonparametric (Mann–Whitney or Kruskal–Wallis) tests, as appropriate. The values from the three visits were compared using one-way ANOVA with repeated analysis for quantitative variables and the McNemar–Bowker test for qualitative variables.
Comparison of the mean SAMANTA questionnaire scores with qualitative variables was performed with the Wilcoxon signed-rank test, Wilcoxon–Mann–Whitney, or Kruskal–Wallis (nonparametric) tests, as appropriate. Pearson's correlation coefficients were used to analyze this association with quantitative variables (change in the duration of menstrual bleeding). No imputation of missing data was done. The analyses were performed with the software package SAS version 9.4 (SAS Institute Inc., Cary, NC, USA). A two-sided p < 0.05 was considered significant.
Results
Between December 12, 2018 and May 18, 2021, 469 participants from 37 centers in Spain were enrolled in the study. Of these, 422 completed the baseline visit and constituted the safety population. Of these, in 371 women the information to assess the primary endpoint was available at the final visit, and constituted the analysis population (Fig. 1). Due to the COVID-19 pandemic, 16 (4.3%) women had their final visit after >15 months.
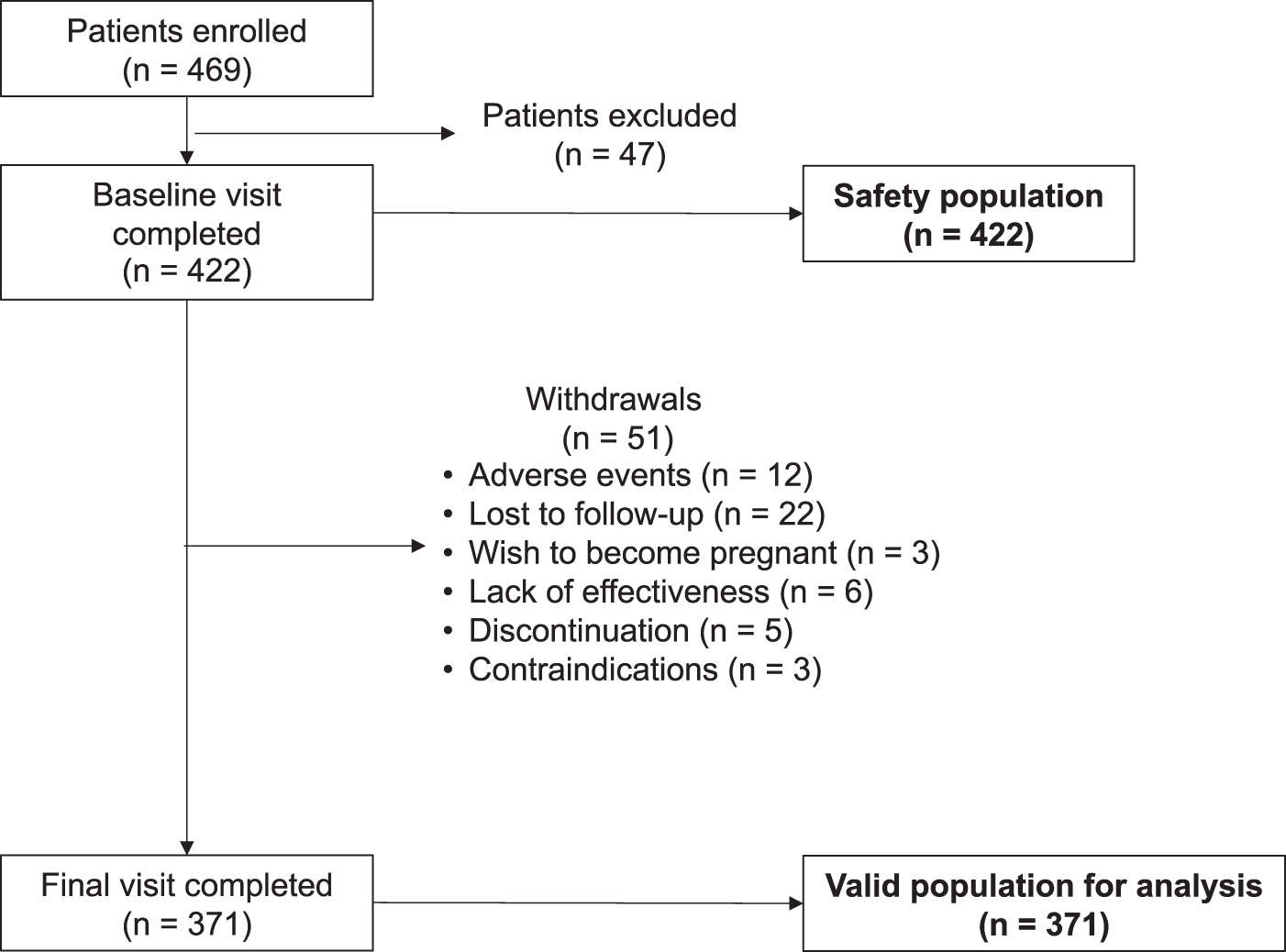
Participants' flow chart.
Baseline characteristics
The mean age of the participants was 41.2 ± 6.5 years. Most of them (81.2%) were Spanish, had higher education (78.2% high school or university degree), and had paid work (83.8%). Two hundred ninety-one (78.4%) were parous, 216 (58.2%) of whom had more than one child (Table 1).
Sociodemographic Characteristics and Gynecological History of Participants
Missing values: a n = 3 (0.8%).
n = 13 (3.5%).
n = 13 (3.5%).
Multiple-choice question. Percentages of use are based on the 234 women using any contraceptive method. Male and female condoms were added to a single category. There were two patients who had selected two contraceptive methods previous to IUD. One of them selected male condom and natural contraceptive method, and the other patient selected male and female condoms.
IUD, intrauterine device; SD, standard deviation.
The median (Q1; Q3) SAMANTA questionnaire score was 8 (7; 10). Most participants (60.9%) reported having very abundant menstrual bleeding with a median (Q1; Q3) duration of 7 (6; 8) days. Around half of the women (53.4%) reported having severe HMB according to PGI-S. This percentage was 32.3 according to CGI-S (Table 2).
Changes from Baseline in the SAMANTA Questionnaire, Clinical Measurements of Menstrual Blood Loss, and Patients' and Clinicians' Assessments of Heavy Menstrual Bleeding Severity Throughout the Study
A score ≥3 in the SAMANTA questionnaire is indicative of heavy menstrual bleeding.
One-way ANOVA with repeated analyses.
McNemar's test based on 286 subjects.
Fisher's test.
Chi-square test.
Wilcoxon Signed-Rank test.
ANOVA, analysis of variance; CGI-S, global impression of menstrual bleeding severity in clinicians; HMB, heavy menstrual bleeding; PGI-S, global impression of menstrual bleeding severity in patients.
Most women (86.5%, n = 321) were using Mirena, 12% (n = 43) received Qlaira, and 1.9% (n = 7) received Progevera.
Final assessments
An interim follow-up visit was reported in 286 (77.1%) women. The percentage of women with a SAMANTA questionnaire score of ≥3 decreased from 100 to 45.8 at this interim visit and to 21 at month 12 (p < 0.001), independently of the treatment used for HMB. At month 12, the SAMANTA questionnaire score had improved in 97.3% of the women according to this questionnaire (p < 0.001; Table 2).
At month 12, 138 (37.2%) women presented amenorrhea. The percentage of women experiencing normal or reduced blood loss increased significantly (29.2 and 60.5, respectively; p < 0.001; Table 2). The SAMANTA questionnaire score improved significantly in 78.4% of the women, with 25.6% of the women showing a strong improvement (Table 2). Duration of menstrual bleeding decreased significantly to a median (Q1; Q3) of 2 (0; 4) days.
According to PGI-S, the percentage of women with light or normal menstrual bleeding significantly increased to 57.1 and 25.6, respectively (p < 0.001). The severity of menstrual bleeding improved in 82.7% of the women, with 60.6% experiencing a strong or moderate improvement. According to CGI-S, the percentage of women with light or normal menstrual bleeding significantly increased to 60.9 and 23.5, respectively (p < 0.001). The severity of menstrual bleeding improved in 84.6% of the women, with 45.7% experiencing a strong or moderate improvement. The amount of bleeding significantly decreased in 86.5% and 86.8% according to PGI-C and CGI-C, respectively (Table 2).
Primary endpoint
At month 12, the reduction in the SAMANTA questionnaire scores was significantly greater in women either reporting a reduction of blood loss (Table 3 and Fig. 2), a shorter duration of menstrual bleeding (Table 3), or a strong improvement in menstrual bleeding severity as assessed by PGI-S and CGI-S (Table 3 and Fig. 3), or a decrease in blood loss according to PGI-C and CGI-C (Table 3; p < 0.001 for all). No relationship was found with the presence of amenorrhea at this time point (Table 3).
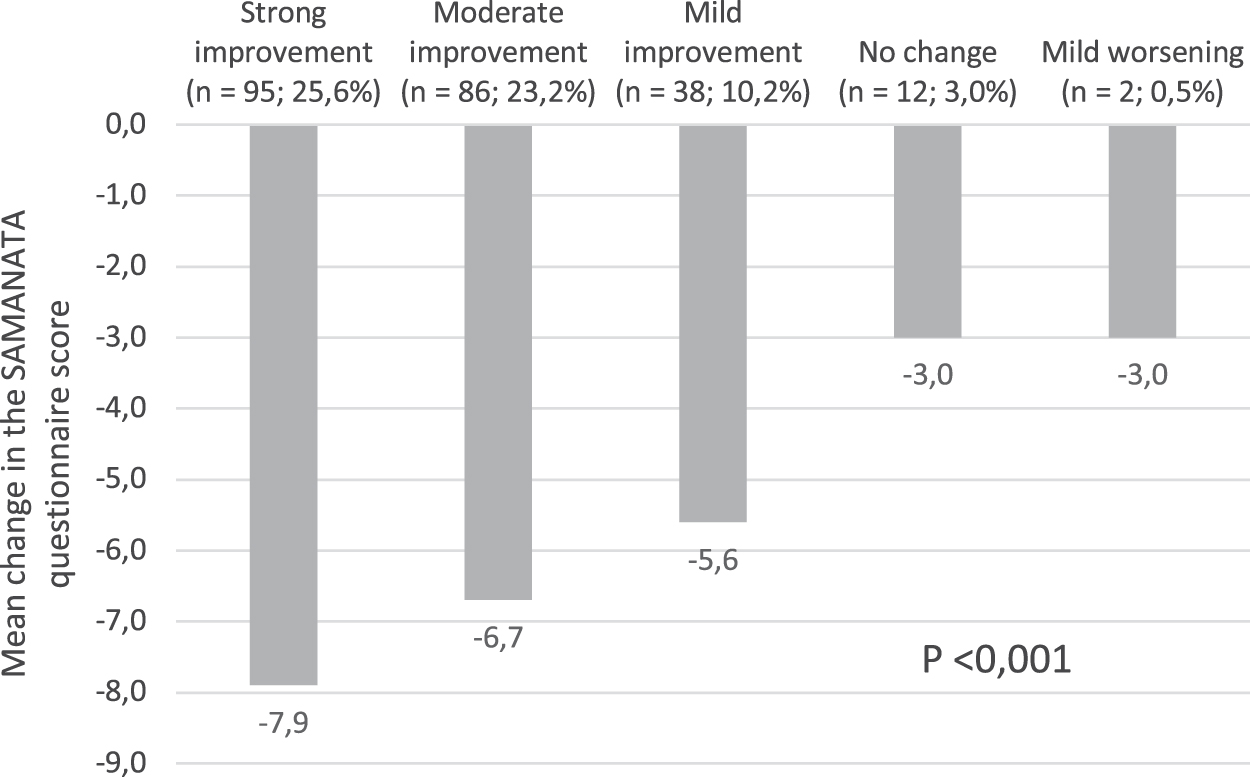
Mean changes in the SAMANTA questionnaire score according to changes in menstrual blood loss (seven levels) after 1 year of treatment.
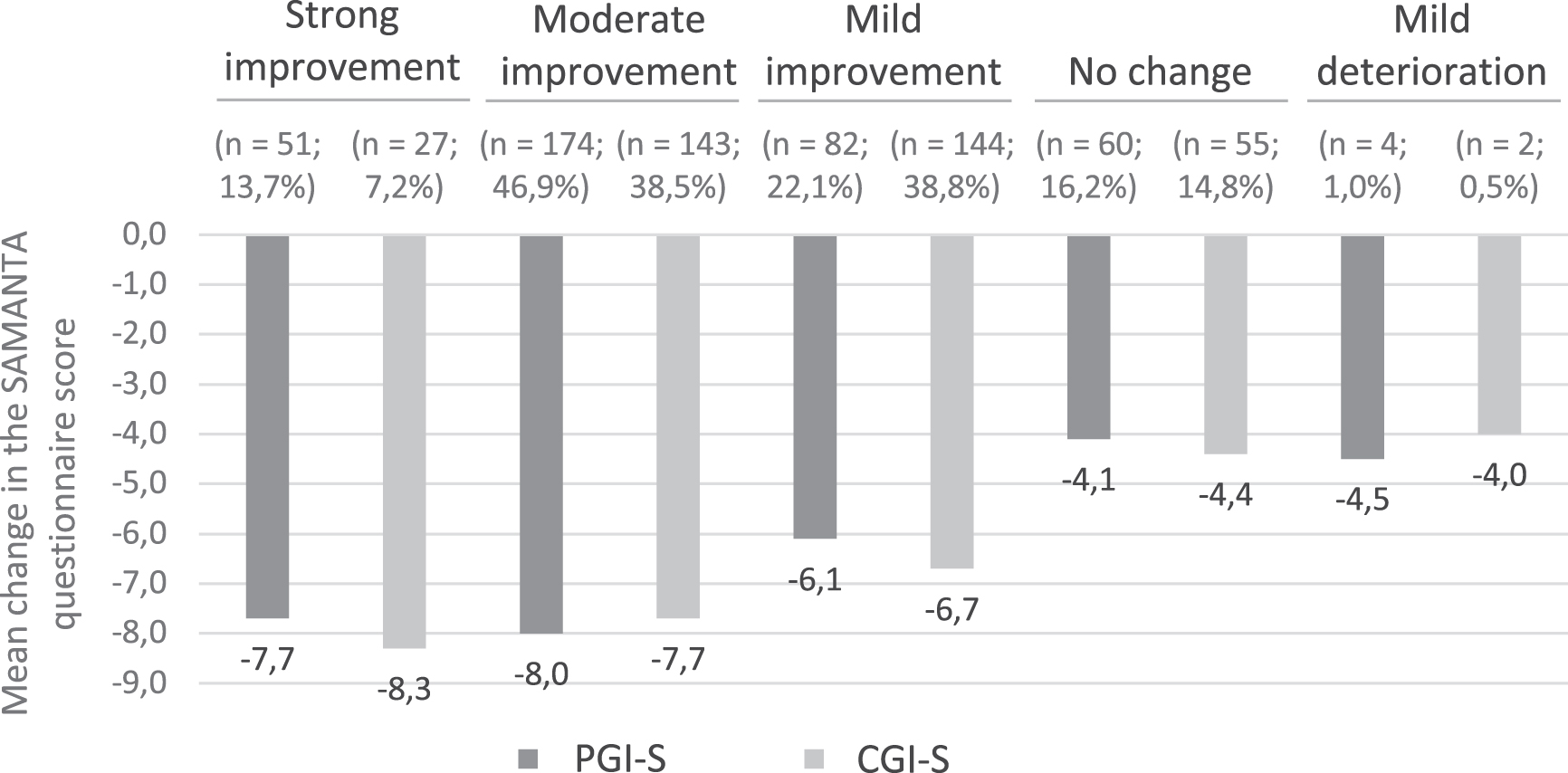
Mean changes in the SAMANTA questionnaire score according to changes in PGI-S and CGI-S (seven levels) after 1 year of treatment. CGI-S, global impression of menstrual bleeding severity in clinicians; PGI-S, global impression of menstrual bleeding severity in patients.
Relationship Between Changes in the SAMANTA Questionnaire Scores and Changes in Heavy Menstrual Bleeding-Related Clinical Measurements, and in Patient's and Clinician's Global Assessments at Month 12
Wilcoxon–Mann–Whitney two sample test.
Kruskal–Wallis test.
p-value associated with (H0) Rho = 0.
One-way ANOVA with repeated analyses.
Quality of life
At the end of the study, all the SF-36 v.2 domains had significantly improved versus baseline (p < 0.001 for all). These changes were inversely associated with changes in the SAMANTA questionnaire scores (p < 0.001 for all except emotional role: p = 0.0263; Table 4).
Quality of Life of Participants at Baseline and Month 12 and Association with Changes in SAMANTA Scores in the Same Time Period
Wilcoxon Signed-Rank test.
p-value associated to (H0) Rho=0.
Discussion
The results of our study show the significant reduction in the SAMANTA questionnaire score after 1 year of treatment for HMB with hormonal treatment, with 79% fewer women presenting HMB (score ≥3) and 97.3% of women improving this condition (reduction in the score). This reduction was significantly associated with a shorter duration of menstrual bleeding during this period and with a lower percentage of women reporting “abundant or very abundant” blood loss, or considering their menstrual bleeding as severe according to PGI-S. Moreover, the reduction in the SAMANTA questionnaire score was significantly associated with a reduction of blood loss as perceived by the women (PGI-C) and clinicians (CGI-C) (p < 0.001 for all).
The reduction in the SAMANTA questionnaire score associated with the improvement of HMB reflects the reduction in both the intensity of menstrual bleeding and the distress caused by this condition, both of which are the ultimate goal of treatment for HMB. 1,10 Most of the women (86.5%) in this study were using an LNG-IUS, followed by estradiol valerate/dienogest (12%). The use of medroxyprogesterone acetate was marginal (1.9%). The high percentage of women using an LNG-IUS is likely to reflect the fact that it is covered by the Spanish National Health System.
In accordance with the latest National Institute of Health and Care Excellence (NICE) 1 and Cochrane Reviews, 12 the Spanish Society of Obstetrics and Gynecology (SEGO) considers LNG-IUS the first-choice hormonal treatment in women who do not wish to become pregnant, followed by combined oral contraceptives. 13 Given this bias in the use of LNG-IUS, the results of our study largely reflect the effect of using this treatment, although, according to the SAMANTA questionnaire, differences in the percentage of women with HMB after 1 year of treatment with any of the three treatments used were nonsignificant.
The reduction in the SAMANTA questionnaire score after 1 year of treatment was significantly associated with improvements in patient-reported outcome measures (PROMs). These included a shorter duration of menstrual bleeding (from a median of 7 days to 2) and a reduction in the self-perceived intensity (from 98.1% who considered their blood loss abundant or very abundant to 10.3%) and severity of menstrual bleeding (from 53.4% who rated their blood loss as “severe” in the PGI-S to 1.3%).
It is worth noting that the percentage of women with “severe” menstrual bleeding at the beginning of the study was 53.4 according to the women's judgment (PGI-S) and 32.2 according to the clinician's judgment (CGI-S). This finding further supports the subjective perception of HMB by women and the impact this condition has on their QoL. 12 Noticeably, at the end of the study the perception of the severity of menstrual bleeding was similar between women (PCI-S) and clinicians (CGI-S).
When using anchor-based methods to explore women's perception of improvement (i.e., the change in the quantity of menstrual bleeding after 1 year of treatment as recorded by the PGI-C), we also found a significant association between the reduction in the SAMANTA questionnaire score and a self-perceived reduction in the quantity of menstrual bleeding. The perception of the change was similar between women (PGI-C) and clinicians (PGI-C).
The minimal clinically important difference (i.e., the difference in the SAMANTA questionnaire score representing a clinically significant change) could not be established, given the exploratory nature of this study. Also, the subjective nature of the condition and the myriad of variables affecting how it impacts women's lives hamper standardization of the evaluation. 14 In such a scenario, a range of estimates, rather than a single value, would be considered clinically significant, according to the population's characteristics.
The impact of HMB encompasses all aspects of health-related QoL (HRQoL) as measured by the SF-36, with all items being below the 25th percentile for the general female population within a similar age range. 15 The reduction in the SAMANTA questionnaire scores was associated with positive effects in all the domains of the SF-36 questionnaire, reflected in the two main components (physical and mental). These showed a significant association with improvements in the SAMANTA questionnaire scores, not only as a result of the reduction of menstrual bleeding, but also because this questionnaire records the impact of this bleeding on QoL.
Some limitations are to be acknowledged in our study. First, the diagnosis of HMB was based on clinical criteria rather than on objective tools. The latter are unusual in clinical practice, given their difficulty of use and the current lack of standardization.7 However, HMB was subsequently confirmed in all cases by the SAMANTA questionnaire, including the five women who considered the intensity of their menstrual bleeding to be normal (n = 5) or even light (n = 2). Other limitations stem from the observational nature of the study, which may generate biases in the way participants are selected, the availability of information, and treatment preferences, as previously mentioned.
In our study, the participants were included consecutively, which avoids intentionality in the selection of women to be included and makes it possible to incorporate a random effect. The required information was available for all the women. Finally, all the information gathered is based on subjective opinion or judgment. However, this aspect is inherent to the evaluation and management of the condition since it incorporates subjective aspects such as QoL and even the perception of HMB.
Conclusion
The SAMANTA questionnaire has proven to be a valid tool for monitoring hormonal treatment for HMB as reflected by the significant association of changes in the SAMANTA questionnaire score after 1 year of treatment and changes in several PROMs (perceived duration and intensity of menstrual bleeding, the severity of menstrual bleeding, and changes in the menstrual bleeding pattern). The clinician's judgment of improvements in severity and changes in the menstrual bleeding pattern were consistent with those of the women, and also showed a significant association with changes in the SAMANTA questionnaire scores. Women's QoL improved during this time frame, with changes in all SF-36 domains also showing a significant association with changes in the SAMANTA questionnaire.
Footnotes
Acknowledgments
The authors thank Beatriz Viejo, PhD, for her assistance in writing and editing the article, and all the SAMIRA investigators for their participation and continued commitment to the study: Andrés Calvo, Aldo Giugni, Francisco Javier García, Jorge Iranzo, Cristina Alonso, Ana Carrasca, Susana Costa, Núria Parera, Xavier Planas, M.a Paloma Pino, Rosa Mora, and María Jesús Cancelo.
Authors' Contributions
J.R.-T. contributed to conceptualization, methodology, visualization, investigation, supervision, software, and validation . J.P., J.C., J.R.-T., and M.A. assisted with data curation, writing—original draft preparation, reviewing and editing.
Author Disclosure Statement
J.P. has received honoraria for consulting, participation in advisory boards, or lecturing from Bayer Hispania, MSD, Theramex, Exeltis, Gynea-Kern and Organon. J.R.-T. is a full-time employee of Bayer Hispania S.L. M.A. has received honoraria for consulting, participation in advisory boards, or lecturing from Bayer Hispania, MSD and Gedeon Richter-Preglem. J.C. has received honoraria for clinical training and consulting activities from Bayer Hispania and Gedeon Richter-Preglem.
Funding Information
This study was sponsored by Bayer Hispania S.L. The sponsorship consisted of the provision of services by Adelphi, an independent company, which performed the management and coordination of the research activity (planning and execution), and the statistical evaluation in addition to medical writing and editorial assistance by Beatriz Viejo, PhD.