
Abstract
Background:
Most women take medication during pregnancy despite limited scientific evidence on safety. We investigated medication use, including changes in and reasons for changes in use during pregnancy, with attention to medication use in pregnant women with chronic conditions.
Materials and Methods:
We conducted an online survey of pregnant women aged ≥18 years (n = 1,226). We calculated descriptive statistics for aspects of medication use and performed multivariable logistic regression to examine associations between change in use and chronic conditions.
Results:
Seventy-nine percent of women took at least one medication during pregnancy. Among those, 63.2% made at least one medication change: 42.0% started, 34.9% stopped, 30.0% missed dose(s), and 18.1% lowered dose(s) from that originally prescribed or recommended. More than a third (36.5%) of women who stopped, lowered, or missed medication did so independent of health care provider advice; 54.0% cited concern about birth or developmental defects as reasons for change. Odds of medication change were higher for women with chronic conditions: digestive conditions—starting (adjusted odds ratio [AOR] = 1.8, 95% confidence interval [CI] = 1.1–2.7), stopping (AOR = 2.1, 95% CI = 1.4–3.3), and lowering (AOR = 2.4, 95% CI = 1.7–3.3) medication; mental health conditions—starting (AOR = 1.6, 95% CI = 1.2–2.2), stopping (AOR = 3.0, 95% CI = 2.3–4.0), or missing (AOR = 2.1, 95% CI = 1.6–2.8) medication; pain conditions—stopping (AOR = 2.9, 95% CI = 2.0–4.2); and respiratory conditions—starting (AOR = 2.0, 95% CI = 1.3–3.1), stopping (AOR = 1.7, 95% CI = 1.1–2.6), and missing (AOR = 2.2, 95% CI = 1.4–3.4) medication.
Conclusions:
Most pregnant women take medication and many, including those with chronic conditions, change their medication use during pregnancy. Medication change may occur independent of health care provider advice and due to women's safety concerns.
Introduction
Nine out of 10 pregnant women in the United States take a medication at some point in their pregnancy. 1,2 Medications might be taken inadvertently before a woman learns she is pregnant 3 or might be required to treat preexisting or pregnancy-induced health conditions. 1,4,5 Medication use during pregnancy has increased in recent decades 1 and may continue to do so given increases in both maternal age 6 and the prevalence of chronic conditions requiring medication among women of reproductive age. 7,8
There is limited scientific evidence, however, on the safe use of most medications during pregnancy 3,9,10 due to the history of exclusion of pregnant women from drug development research and clinical trials. 5,11 To address this need, the U.S. Food and Drug Administration (FDA) and its Office of Women's Health (OWH) have increased efforts to promote the inclusion of pregnant women in clinical research. FDA has been actively engaged in efforts to improve knowledge and research on safe and effective therapies for use during pregnancy and lactation, such as the Task Force on Research Specific to Pregnant Women and Lactating Women, 12 and the Agency has published guidance outlining-related scientific considerations. 13 –15
In addition, OWH has a long history of funding research 16 to expand the knowledge of medication use in pregnancy and provides a public listing of pregnancy exposure registries to raise awareness of opportunities for pregnant women to participate in research. 17 Despite this headway, there remains a dearth of data to inform drug safety in pregnant women, leaving pregnant women and their health care providers to navigate medication use without adequate information on most drugs' safety, efficacy, or optimal dosing regimen during pregnancy. 5,11
For these reasons, it is important to study medication use in pregnancy. Studies have estimated overall prevalence of medication use in pregnancy, 1,2,4,18 but there is little research regarding patterns or changes in medication use, a critical component to understanding how pregnant women negotiate medication benefits versus risks to the health of themselves and their fetuses. Investigating changes in medication use may be particularly important for pregnant women with chronic health conditions, for which inadequate treatment might increase adverse pregnancy outcomes. 19 –23 Further, pregnant women express fears about medication safety and the potential for its adverse effect on the health of their babies during pregnancy and beyond 24,25 ; international research indicates that these fears influence pregnant women's medication nonuse and nonadherence. 26 –29
To better understand behaviors around medication use in pregnancy in the United States, we surveyed pregnant women about their medication use and how they assessed medication safety. This study investigated changes in and reasons for changes in their medication use during pregnancy with attention to women with chronic conditions.
Materials and Methods
OWH contracted with WebMD Health Corp. (WebMD) to conduct an online survey of pregnant women who visited
Quota sampling was used to recruit respondents by self-reported race and ethnicity (non-Hispanic White, non-Hispanic Black/African American, Hispanic, non-Hispanic other racial and ethnic groups) in proportion to total U.S. 2016 births,
31
and poststratification weights were applied to reflect these population proportions.
32
Respondents were enrolled in a lottery to win 1 of 25 $100 gift cards from WebMD if they completed the survey.
Measures
Respondents' demographic characteristics included self-reported age in years (18–24, 25–29, 30–34, 35 and older), pregnancy trimester at the time of the survey, race and ethnicity (White, non-Hispanic; Black/African American, non-Hispanic; Hispanic or Latina; Asian, non-Hispanic; multiple or other race, non-Hispanic), education level (less than high school; high school, technical/vocational school; college education or degree; postgraduate education or degree), urban or rural residence, and region (northwest; midwest; south; west). We also estimated poverty level using federal poverty thresholds. 33 Household income was recorded in 10 categories ranging from less than $10,000 to over $200,000; we adjusted income to the categorical midpoint for family size 1–5 or more, and categorized women as at or below the federal poverty level or above the federal poverty level. Diagnosis of a chronic health condition was determined by asking respondents “Have you been diagnosed with any of the following chronic (long-lasting or persistent) conditions?”
Response options included any cancer, for example, skin, lung, or breast; any heart or cardiovascular disease, for example, coronary artery disease, atrial fibrillation, or irregular heart rhythm; type 1 or type 2 diabetes; any digestive condition, for example, gastroesophageal reflux disease (GERD) and irritable bowel syndrome; any mental health condition, for example, anxiety or attention-deficit hyperactivity disorder (ADHD); depression; any chronic pain, for example, back, migraine, rheumatoid arthritis, and sciatica; any chronic respiratory condition, for example, asthma, chronic obstructive pulmonary disease (COPD), and any other chronic condition not listed. Women who responded “other” were given a write-in option, and common responses were categorized, i.e., anemia, autoimmune disease, endometriosis, hepatitis C, hypercoagulable state, multiple sclerosis, polycystic ovary syndrome, and thyroid-related conditions, and included in descriptive analysis.
Medication use during pregnancy was assessed by asking women to indicate if they used the following medications during their pregnancy: acetaminophen (Tylenol), aspirin, ibuprofen (Advil, Motrin), antibiotics, antinausea medication, cold/cough/flu medication, allergy medication, antifungal medication, laxatives, anticonvulsant (antiseizure) medication, antidepressants, heart/cardiovascular medication, natural or dietary supplements, iron supplements, prenatal vitamins, and other vitamins (excluding prenatal). Iron supplements and prenatal and other vitamins were not considered to be medication for the purposes of this analysis. Women could choose to report “other types of medication not listed,” and were asked to specify if each of the medications they had taken was prescribed or sold over-the-counter (OTC). They were also asked what actions they had taken to help decide which medications are safe to take while pregnant and were provided a list, from which they could select multiple responses (see response options in Fig. 1).
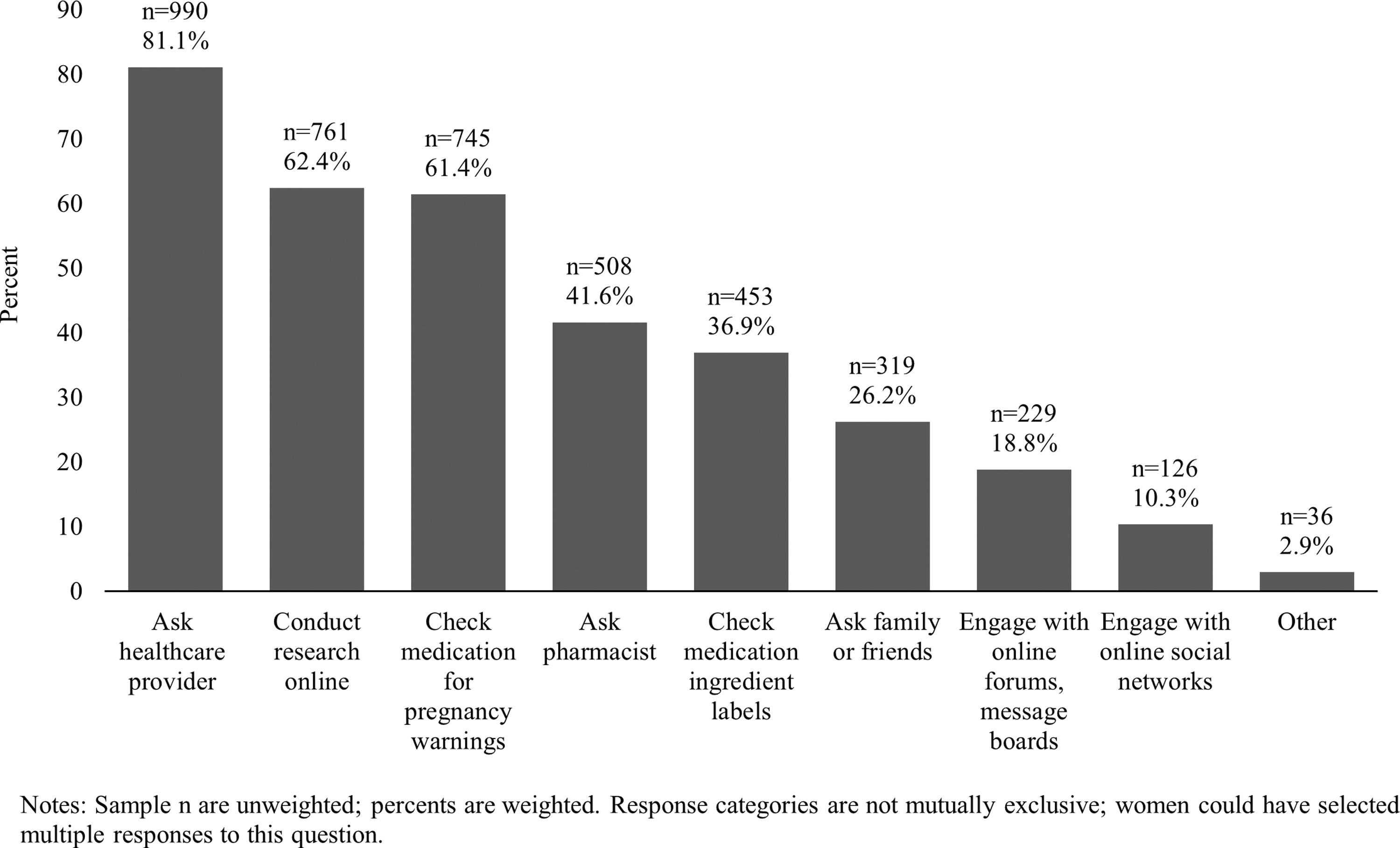
Actions taken to help determine medication safety while pregnant (n = 1,226).
The survey assessed four measures of change in medication use by asking women if they had ever done any of the following while pregnant (response options were yes or no): started a new prescribed or recommended medication; stopped taking a prescribed or recommended medication; took a lower dose of a medication than that originally prescribed or recommended; and missed a dose of a prescribed or recommended medication. Women who indicated that they had stopped, lowered, or missed medication during pregnancy were asked “Did you not take your medication(s) as prescribed or recommended while you were pregnant for any of the following reasons?” and were prompted with a list of eight possible reasons, from which they could select multiple responses (see response options in Fig. 2).

Reasons for change in medication use among women who stopped, lowered, or missed medication during pregnancy (n = 468).
Responses to questions measuring health conditions, medication use, and changes in medication use were not mutually exclusive; women could select multiple responses. To minimize response bias, for each iteration of the survey, the display order of response options was randomized for questions in which the responses did not have a logical order or sequence.
Data analysis
Unweighted frequencies and weighted percentages were calculated for respondent characteristics, chronic health conditions, and aspects of medication use during pregnancy for the full study sample. Among women who took a medication during pregnancy, unadjusted logistic regression was used to test for associations between demographics, health conditions, type of medication use, and change in medication use. Also, among women who took a medication during pregnancy, a series of multivariable logistic regression models were estimated to identify associations between health conditions and changes in medication use. The multivariable models were mutually adjusted for age, trimester, race/ethnicity, education, estimated poverty status, and for having a chronic health condition and were only estimated for health conditions with sufficient observations given the number of covariates in the model (i.e., digestive, mental health, pain, and respiratory conditions). 34 All regression models were weighted, and analyses were performed using SAS v9.4 (SAS Institute Inc., 2016).
Results
Characteristics of the full study sample (n = 1,226) are presented in Table 1. Each of the following age groups comprised a quarter or slightly more respondents: 25–29 years (24.9%), 30–34 years (28.8%), and ≥35 years (27.9%); 18.3% were between 18 and 24 years. Nearly half of women (49.2%) were in the first trimester of pregnancy. Most women were non-Hispanic White (52.1%), while 23.3% identified as Hispanic or Latina, 14.1% non-Hispanic Black/African American, 6.7% multiple or other racial or ethnic groups, and 3.9% non-Hispanic Asian.
Descriptive Characteristics of the Study Sample (n = 1,226)
Sample n are unweighted; percents are weighted.
Hispanic or Latina includes any or multiple races.
Based on 2019 federal poverty guidelines. 33 Household income was adjusted to the categorical midpoint for family size 1–5+. Poverty could not be calculated for n = 154 respondents who declined to provide household income.
Includes suburban and exurban.
Defined by U.S. Census Bureau. 58
Categories are not mutually exclusive; women may have selected more than one response.
Includes G6PD deficiency, pernicious anemia.
Includes Crohns' disease, Sjogren's syndrome, lupus, psoriasis, idiopathic thrombocytopenic purpura, ulcerative colitis, and pernicious anemia.
Includes antiphospholipid syndrome, protein C deficiency.
Includes hypothyroidism, hyperthyroidism, Hashimoto's disease, Grave's disease.
List of medications provided to respondents included: acetaminophen (Tylenol), aspirin, ibuprofen (Advil, Motrin), antibiotics, antinausea medication, cold/cough/flu medication, allergy medication, antifungal medication, laxatives, anticonvulsant (antiseizure) medication, antidepressants, heart/cardiovascular medication, natural or dietary supplements, and other types of medication.
OTC, over-the-counter.
The majority had college educations or degrees (52.0%); 27.4% had completed high school or technical/vocational school, 15.1% had completed postgraduate education, and 5.6% had less than a high school education. Most women were above the poverty level (61.5%) and were from urban areas (84.2%). By U.S. region, 38.7% of women lived in the South, 24.4% in the West, 21.1% in the Midwest, and 15.6% in the Northwest.
Slightly less than half of women reported being diagnosed with chronic health conditions (47.7%). Nearly a third (32.0%) reported a mental health condition, followed by 13.3% who reported having chronic pain. Approximately 8% reported a digestive condition (8.7%), chronic respiratory condition (8.4%), or other chronic condition (7.9%). Four percent of women reported being diagnosed with cardiovascular disease and 3.2% with diabetes. Fewer than 2% of women reported other health conditions such as thyroid-related conditions, polycystic ovary syndrome, or cancer. Nearly 80% of women had taken a medication during pregnancy (79.0%) with 48.1% taking a prescription medication and 70.0% taking an OTC medication. Four in 10 women (39.1%) took both a prescription and an OTC medication during pregnancy; 30.9% took an OTC medication only and 9.0% took a prescription only. Iron supplements and prenatal and other vitamins were not considered to be medication.
Figure 1 shows actions that women in the full study sample took to determine medication safety during pregnancy. The majority (81.1%) asked a health care provider. Approximately 6 in 10 women conducted research online (62.4%) and checked medications for pregnancy warnings (61.4%). Roughly 4 in 10 (41.6%) asked a pharmacist and checked medication labels (36.9%), and 26.2% asked family or friends.
Among women who reported taking any medication during pregnancy, a majority (n = 609, 63.2%) made at least one change in their medication use during pregnancy, and 38.4% (n = 369) made more than one change (data not shown). Table 2 shows that 42.0% started a new medication that was prescribed or recommended to them while slightly fewer stopped a medication (34.9%). Smaller but notable percentages of women reported missing a dose (30.0%) or lowering the prescribed or recommended dose (18.1%).
Among women taking a medication, age, race/ethnicity, and education were not associated with change in medication use. Pregnancy trimester was associated with starting medication (second trimester: odds ratios [OR] = 1.8, 95% confidence interval [CI] = 1.3–2.5; third trimester: OR = 2.3, 95% CI = 1.7–3.2) and with missing doses (third trimester: OR = 1.6, 95% CI = 1.2–2.3; Table 2). Being at or below poverty was associated with missing doses (OR = 1.6, 95% CI = 1.2–2.2) compared with being above the poverty level. There was a significant, positive association between diagnosis with a chronic health condition and each of the measures of change in medication use; ORs ranged from 1.8 (95% CI = 1.4–2.3) for starting medication use to 3.3 (95% CI = 2.5–4.4) for stopping.
The type of medication was also significantly associated with each of the changes in medication use. Compared to women taking OTC medication only, the odds of a change were greater for women taking both prescription and OTC medications and for women taking prescription medications only (Table 2). We tested for association between reported diagnosis with a health condition and type of medication and found a significant, positive association with prescription medication (OR = 2.9, 95% CI = 2.2–3.8) but no association with OTC medication (OR = 0.7, 95% CI = 0.4–1.0; data not shown).
Figure 2 presents reasons for change in medication use among women who reported stopping, lowering, or missing medication during pregnancy. The majority, 64.4%, reported following the advice of health care professionals while smaller percentages reported following advice based on internet research (30.5%) and from family and friends (18.5%). More than half (54.0%) cited concern about birth defects or other developmental issues as a reason for change in medication. Other concerns related to adverse health outcomes were also reported, including concern for miscarriage or stillbirth (40.4%), for personal health (24.8%), and that the baby would develop autism (21.7%).
Table 3 presents results from a series of multivariable logistic regression models testing for associations between select health conditions (i.e., those with sufficient observations) and changes in medication use during pregnancy, controlling for demographic measures. Each of the health conditions examined had a significant association with at least one of the measures of medication change. Women who reported digestive conditions had greater odds of starting (adjusted odds ratio [AOR] = 1.8, 95% CI = 1.1–2.7), stopping (AOR = 2.1, 95% CI = 1.4–3.3), and lowering (AOR = 2.4, 95% CI = 1.7–3.3) medication, while women with mental health diagnoses were more likely to start (AOR = 1.6, 95% CI = 1.2–2.2), stop (AOR = 3.0, 95% CI = 2.3–4.0), or miss (AOR = 2.1, 95% CI = 1.6–2.8) medication compared to women without these respective conditions.
Characteristics Associated with Change in Medication Use Among Women Taking Medication During Pregnancy (n = 965)
Percents are weighted. ORs are considered significant if 95% CIs do not include 1.0. Categories are not mutually exclusive; women may have made more than one change in medication use.
Hispanic or Latina includes any or multiple races.
Based on 2019 federal poverty guidelines. 33 Household income was adjusted to the categorical midpoint for family size 1 to 5+. Poverty status could not be calculated for n = 116 respondents who declined to provide household income.
CI, confidence interval; OR, odds ratios; OTC, over-the-counter.
Chronic Health Conditions Associated with Change in Medication Use Among Women Taking Medication During Pregnancy (n = 965)
Percents are weighted. AORs of the association between change in medication use and each of the health conditions were estimated using multivariable logistic regression. Each model adjusted for age (ref: 30–34 years), trimester (ref: first), race/ethnicity (ref: White, non-Hispanic), education (ref: college education or degree), poverty estimate (ref: above poverty level). AORs are considered significant if 95% CIs do not include 1.0.
Categories are not mutually exclusive; women may have made more than one change in medication use or had more than one health condition.
AOR, adjusted odds ratios.
For women who reported respiratory conditions, the odds of starting (AOR = 2.0, 95% CI = 1.3–3.1), stopping (AOR = 1.7, 95% CI = 1.1–2.6), and missing (AOR = 2.2, 95% CI = 1.4–3.4) medication were greater than for women who did not report respiratory conditions. Women who reported chronic pain conditions had 2.9 (95% CI = 2.0–4.2) greater odds of stopping a medication compared to women who did not report pain conditions.
Discussion
In our study investigating pregnant women's behaviors related to medication safety and use during pregnancy, we found that nearly 80% of women surveyed reported taking a medication during pregnancy. These findings are in line with earlier estimates using population-based data 1 and with more recent cohort study data, 18 which report that the percentage of women in the United States using any medication during pregnancy ranges from 73% to 89%. Our estimates of prescription (48.1%) and OTC medication use (70.0%) were similar to those reported by other research in the United States. 1,35 –37 and supply further evidence that medication use in pregnancy is common.
Women reported using several behaviors to help them decide which medications were safe to take while pregnant. Although most women in our study asked their health care providers (81.1%) or pharmacists (41.6%), more than 60% conducted their own research online (62.4%) or checked the medication for pregnancy warnings (61.4%). Use of the internet as a source of health information, including for medication safety, 38 –40 is widespread among pregnant women. 41 There is limited evidence, however, as to the quality of the information accessed; a survey of pregnant women contacting a teratology information service, for example, found that 22% had retrieved incorrect information from the internet about their medication exposure. 40 Further, most women do not discuss the information they find with their health care provider. 41
Medication labeling may also be an imperfect resource for products with insufficient data to inform risk on use during pregnancy. The FDA's Pregnancy and Lactation Labeling Rule (PLLR) requires that product labeling present benefit-risk information for pregnancy and lactation; information on pregnancy testing, contraception, and infertility is included, if applicable. 42 While the PLLR provides a cohesive and standard format, it is limited by the data or lack thereof. 43 A 2020 review of labeling for 290 medications found only 11% presented data derived from human studies and 90% relied on animal data. 44
Among women who took a medication during pregnancy, we found that a majority (63.2%) reported making at least one change in medication use during their pregnancy. Forty-two percent started a prescribed or recommended medication while slightly fewer stopped medication (34.9%) or missed (30.0%) or lowered the prescribed or recommended dose (18.1%). Few U.S. studies have quantified changes in medication use during pregnancy. 18,45 Our findings suggest that there are additional unexplored patterns of use and adherence with potential to impact maternal and fetal health.
We also asked women who had stopped, lowered, or missed medication the reason for not taking a medication as prescribed or recommended. While a majority (64.4%) stated they followed the advice of a health care provider, more than one-third (35.6%) made a medication change independent of provider advice. Moreover, notable percentages of women reported stopping, lowering, or missing a dose due to concerns over medication safety, including that the medication would cause birth defects or developmental issues (54.0%), miscarriage or stillbirth (40.4%), negative impact on their own personal health (24.8%), and autism spectrum disorder in their baby (21.7%).
The finding that pregnant women changed their medications and dosing out of concern for safety and without consulting a health care provider is concerning for maternal and fetal health. Although the lack of scientific data prevents understanding the true risks for most medications in pregnancy, studies suggest that women overestimate the risks of taking medication 26,46 –48 and decide against use when their own research yields conflicting information on safety. 49 Caution toward and avoidance of medication during pregnancy is further fed by social structures, which prioritize fetal health and judge the mother as responsible for and in control of fetal health. 50 These forces are evident in qualitative research, in which women report focusing most heavily on the safety of the fetus in their decisions about medication use 24,25 and may have influenced medication change among women in our study.
Our findings also indicated that women with chronic conditions were more likely to have taken a prescription medication during pregnancy and to have made a medication change than those without a chronic condition. We further examined the relationship between specific chronic conditions and medication change. Although our survey did not track individual medications or their indications, we noted patterns in change specific to each health condition. Women with chronic digestive, mental health, or respiratory conditions had higher odds of starting and of stopping a medication compared to women without these respective conditions, and women with chronic pain were more likely to have stopped a medication than were those without pain.
Starting a medication may reflect treatment of a condition and, in combination with stopping a medication, may reflect a modification in treatment appropriate to standards of care during pregnancy, for example, switching from one medication to another with a more favorable safety profile. Starting and stopping a medication might also indicate treatment and resolution, respectively, of a temporary problem or the recurrence of a chronic condition exacerbated by pregnancy. In contrast, ours and other research also suggest that women stop medication used to treat chronic conditions independent of health care provider instruction due to concerns about medication safety 25,28,29,51 –53 or due to unintentional nonadhereance. 54
Concerns about safety and nonadherence may be further reflected in our findings that women with these health conditions were more likely to lower (for digestive conditions) or miss (for mental health and for respiratory conditions) prescribed or recommended doses. Many chronic conditions worsen during pregnancy and when treated inadequately or inappropriately are linked to adverse pregnancy and birth outcomes. 19 –23
Our findings further suggest that patient–provider communication on medication use and safety is critical during pregnancy. Decisions on medication use and on treatment of chronic conditions during pregnancy are best made by the patient in concert with the provider to support the full evaluation of medication risk and benefit using the available data. 23 Research shows that evidence-based counseling on medication safety is successful at reducing anxiety and increasing adherence among pregnant women, 46 including those with chronic conditions. 55
Our study is among the first in the United States to quantify actions pregnant women take to determine medication safety as well as changes in and reasons for changes in medication use during pregnancy. Further strengths include the representative nature of our sample, which used quotas to ensure racial and ethnic representation similar to that of the U.S. population, had a prevalence of chronic conditions and of medication use similar to that seen in other U.S.-based studies, 1,7,18 and was drawn from one of the most heavily accessed health-based websites in the United States. 30 Still, the sample may not be representative of individuals without access to or regular use of the internet and may be biased toward individuals more likely to use and to rely on the internet as a health information source.
In addition, we cannot calculate a response rate since survey administration did not capture refusal to participate and since there is no sampling frame for visitors to
Conclusions
A majority of pregnant women take at least one medication during pregnancy. Although most rely on health care provider advice both for evaluating medication safety and for making a medication change, a notable number take actions on safety or make medication changes independent of their health care provider. These findings are potentially problematic for maternal and fetal health as untreated health conditions may lead to adverse pregnancy outcomes, and providers cannot deliver adequate care if they are not informed of their patients' true medication use patterns.
An opportunity exists for patients and providers to discuss potential medication safety concerns and for providers to use evidence-based counseling, which has been shown to improve pregnant women's medication adherence and outcomes. Finally, additional research to inform safe medication use during pregnancy is necessary. FDA OWH remains committed to supporting this research, to providing education, and to advancing understanding of medication, use, safety, and effectiveness in pregnancy and lactation.
Footnotes
Acknowledgment
The authors thank the study participants for sharing their experience and Joanne Berger, FDA Library, for article editing assistance.
Disclaimer
The contents of this publication reflect the thoughts of the authors and do not represent the official views of, nor an endorsement by, the FDA, Department of Health and Human Services, or U.S. Government.
Authors' Contributions
S.K.H.: Conceptualization, Methodology, Formal analysis, and Writing—Original Draft. L.D.: Conceptualization, Methodology, and Writing—Review and Editing. E.M.S. and C.L.: Conceptualization, Methodology, Writing—Review and Editing, Project administration. S.Z.: Conceptualization, Methodology, Formal analysis, Writing—Review and Editing, and Project administration. K.V.: Project administration, Funding acquisition, and Writing—Review and Editing. S.B.-M.: Conceptualization, Supervision, and Writing—Review and Editing.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This work was supported by a contract between FDA and WebMD Health Corp (Grant No. FDABAA-18-00123N).