
Abstract
Background:
To determine whether the 2gether intervention increases use of a dual protection (DP; concurrent prevention of pregnancy and sexually transmitted infections [STIs]) strategy and decreases pregnancy and STIs among young African American females, who disproportionately experience these outcomes.
Materials and Methods:
We conducted a randomized clinical trial comparing the 2gether intervention to standard of care (SOC). Participants were self-identified African American females aged 14–19 years who were sexually active with a male partner in the past 6 months. Participants were followed for 12 months; 685 were included in the analytic sample. The primary biologic outcome was time to any incident biologic event (chlamydia, gonorrhea, trichomonas infections, or pregnancy). The primary behavioral outcomes were use of and adherence to a DP strategy.
Results:
2gether intervention participants had a decreased hazard of chlamydia, gonorrhea, trichomonas infections, or pregnancy during follow-up, hazard ratio = 0.73 (95% confidence interval [CI] 0.58–0.92), and were more likely to report use of condoms plus contraception, generally, adjusted risk ratio (aRR) = 1.61 (95% CI 1.15–2.26) and condoms plus an implant or intrauterine device (IUD), specifically, aRR = 2.11 (95% CI 1.35–3.29) in the prior 3 months compared with those receiving SOC. 2gether participants were also more likely to report use of condoms plus an implant or IUD at last sex and consistently over the prior 3 months.
Conclusions:
2gether was efficacious in increasing use of condoms with contraception and decreasing pregnancy or selected STIs in our participants. Implementation of this intervention in clinical settings serving young people with high rates of pregnancy and STIs may be beneficial.
ClinicalTrials.gov, No. NCT02291224 (
Introduction
Unintended pregnancy and sexually transmitted infections (STIs) are serious, preventable public health problems and are experienced disproportionately by young people. More than 75% of pregnancies that occur in people aged 15–19 years are unintended. 1 In 2019, the birth rate among this age group in the United States was 16.6/1000. 2 While this represents a new record low compared to previous years, 2 it remains high compared to other industrialized countries. 3 African American adolescents, particularly those in the South, have higher birth and STI rates than adolescents of other racial and ethnic groups. 4 There is an urgent need to effectively address both pregnancy and STI prevention among this population.
Dual protection (DP) is the concurrent prevention of unintended pregnancy and STIs. 5 Strategies for DP include actions or combinations of actions that can prevent both outcomes at the same time. Common DP strategies include abstinence, condom use alone, or dual method use (i.e., condoms plus an intrauterine device [IUD], implant, injection, ring, patch, or pill). Dual method use is recommended by many public health and medical organizations as the most effective DP strategy, however, only 9% of youth reported dual method use at last sex in a recent national survey. 5 –9 Use of DP strategies is influenced by individual, relationship, and contextual factors 10,11 ; these factors interact with each other and change over time. As adolescents themselves develop, their sexual relationships change, and other exposures shape their experiences and behaviors. However, effective, developmentally appropriate DP interventions for adolescents that are responsive to their changing lives are currently lacking. 12
“2gether: The Dual Protection Project” is a multicomponent, clinic-based intervention to increase DP and address high rates of STIs and unintended pregnancy among African American adolescent females served by a teen clinic in the Southeastern United States. 13 This patient-centered intervention was informed by the Information-Motivation-Behavior theory and leveraged motivational interviewing (MI) techniques. 14,15 We hypothesized that 2gether participants would have a lower risk of incident chlamydia, gonorrhea, trichomonas infections or pregnancy, and increased use of DP strategies over a 12-month follow-up.
Materials and Methods
We used a nonblinded, randomized trial design to evaluate the 2gether intervention relative to standard of care (SOC). 13 The Institutional Review Boards at our respective institutions approved this protocol. We received a waiver of parental consent for participants aged <18 years.
From March 2015 through August 2017, we recruited participants from a teen clinic that receives Title X funding. Clinic attendees were approached in the waiting area and invited to learn more about the study. Those who were interested in learning more and potentially participating were screened for eligibility. Eligibility criteria included self-identification as Black or African American and female; 14–19 years of age; sexually active with a male partner in the past 6 months; not pregnant; no desire to be pregnant in the next year; HIV negative by self-report; plan to stay in the area for the next year; and not previously enrolled in the pilot study of this intervention.
In our setting, adolescents who are living with HIV receive expanded care and support services in a specialized clinic, which could impact follow-up as well as bias the results. Participants who were diagnosed with HIV on the day of enrollment or had pregnancy diagnosed within 4 weeks of enrollment were ineligible for further study participation.
The intervention, SOC control, and study schema detail have been previously described. 13 In brief, control participants received SOC at the teen clinic, which provides comprehensive family planning services. Clinical care follows guidance from the CDC U.S. Medical Eligibility Criteria for Contraceptive Use, U.S. Selected Practice Recommendations for Contraceptive Use, CDC and Office of Population Affairs Quality Family Planning recommendations, and Title X Program requirements. 5,16,17 Although there is no specific counseling protocol as part of the SOC, a typical contraceptive visit involves contraceptive counseling by a medical provider, reinforcing education by a health educator and dispensing of the contraceptive method (when applicable) by a nurse. Teens have follow-up every 3 months and are encouraged to return as frequently as needed.
Intervention participants had access to the same SOC clinical services. They also participated in the 2gether intervention, which included the following components upon enrollment: (1) an interactive multimedia program focused on DP strategies and preparation for the selection of a DP strategy (referred to as the MMDP for multimedia dual protection program), (2) a structured counseling session with a medical provider to select a DP strategy, and (3) a structured health education and counseling session with a study nurse educator to build skills for correct and consistent use of the selected DP strategy.
The MMDP included video vignettes of young African American females who shared motivations for and experiences with relationships, STI and pregnancy prevention, and DP use. It also addressed common myths, sought to increase knowledge about and motivation for DP use. Reflection questions were asked during MMDP to gather information from the participant about priorities and values that may influence her DP strategy. The answers were later used to tailor the DP strategy selection and DP skills counseling. The MMDP was administered by the study team and it took ∼25 minutes to complete, although this was variable because it was interactive and the participant could explore the detailed information as much as she desired.
The MMDP contained a visual aid comparing DP strategies according to how well they could work to prevent STIs and pregnancy and introduced the concept that hormonal contraception or an IUD worked better when used together with a condom. This set the stage for interaction with a provider and selection of a DP strategy. The provider incorporated answers to the reflection questions provided in the MMDP, the participant's self-perceptions of risk for STI and pregnancy, and motivations for DP use to interactively work with the participant to select a DP strategy that she feels would work best for her. Participants were supported in their decision even if their selected strategy was not one that was emphasized in MMDP. Thereafter, participants met with a nurse educator to explore how to apply their selected DP strategy in her unique context outside the clinic setting.
In this study, each participant could consider her life goals and how DP use may help achieve them, anticipate challenges, and identify potential solutions to using her selected DP strategy, learn how to use a condom correctly, and build communication skills. This session was highly interactive and included activities such as role plays, condom use demonstrations, DP strategy journaling, and preparing for change. The structured counseling sessions add about 15 minutes to the clinic visit compared to SOC.
Six months later, participants received (1) an abbreviated version of the MMDP, lasting ∼10 minutes and (2) a structured health education and counseling session with a study nurse educator to reinforce skills for correct and consistent use of the selected DP strategy. Participants who desired to change their DP strategy at the follow-up visit or any other time during study follow-up received structured counseling with a medical provider and nurse educator similar to that at enrollment. Booster intervention phone calls with a nurse educator occurred once per quarter during the follow-up period. All counseling sessions used core principles of MI (i.e., supporting self-efficacy, reflective listening, expressing empathy, supporting change talk) but did not strictly adhere to MI protocols. 14
All medical providers and nurse educators conducting counseling sessions received MI training and had taped sessions with feedback before beginning work on the intervention and ongoing training and support in applying MI techniques throughout the study. DP strategies addressed throughout the 2gether intervention included abstinence, condom use alone, or dual method use, with the latter emphasized because it is recommended as the most effective DP strategy. 5
The primary biological outcome was time to first event of any one of the following: laboratory-confirmed chlamydia, gonorrhea, trichomonas infection, or pregnancy. In addition to laboratory-confirmed outcomes, trichomonas could also be diagnosed by wet prep, and pregnancy could also be diagnosed by an ultrasound examination or documentation of fetal heart tones. STIs were considered incident if a particular STI was negative at enrollment and was newly positive. STIs were also considered incident if a particular STI was positive at enrollment, with either documentation of directly observed therapy or an intervening negative result, and was found to be positive again. All pregnancies diagnosed after 4 weeks postenrollment were considered incident events. We also considered each biological outcome separately.
The primary behavioral outcomes were any use of a DP strategy in the past 3 months, use of a DP strategy at last sex, and consistent use of a DP strategy during the past 3 months. We categorized DP strategies in two ways. The first was a three-level variable: (1) no DP strategy, (2) abstinence or condom use alone, or (3) dual method use. The second was a six-level variable that considered each strategy individually: (1) no DP strategy; (2) abstinence; (3) condom use alone; (4) pill, patch, or ring plus condoms; (5) injection plus condoms; or (6) IUD or implant plus condoms. Consistent use of a DP strategy was defined as being abstinent, using condoms alone with every episode of sex, or using condoms with every episode of sex plus use of an IUD, implant, injection, pill, patch, or ring currently and in the past 3 months.
Levels of STI and contraceptive knowledge, condom and contraceptive use self-efficacy and intentions, and partner communication self-efficacy and frequency were examined as secondary behavioral outcomes. We used validated scales for condom use self-efficacy and partner communication self-efficacy and frequency (behavioral outcome measures in Supplementary Appendix SA1). 18,19
We collected urine specimens for STI and pregnancy testing during study visits at enrollment and 6 and 12 months postenrollment. In addition, we abstracted biological outcomes via medical chart reviews for nonstudy-related visits. Participants were asked if they had visited outside clinics and had a pregnancy or STI test since their last study visit; we requested records from visits to outside clinics and abstracted them when possible. We collected behavioral data by self-report every 3 months. At enrollment and 6 and 12 months postenrollment, participants completed the survey using an Audio Computer-Assisted Self-Interview (ACASI) questionnaire. At 3 and 9 months, the survey was administered by phone or in person by study staff. Participants received a $40 gift card for the initial, 6-, and 12-month visits and a $10 gift card for the 3- and 9-month survey.
We calculated the sample size based on the number needed to evaluate our primary biological outcome. Using an expected incidence of 35% over 12 months (from review of laboratory data at this clinic) and an estimated lost to follow-up rate of 35%, a sample size of 710 would allow us to detect a hazard ratio (HR) of 0.65 with 80% power and α = 0.05. 20
We assigned participants to the 2gether intervention or SOC in a 1:1 ratio using permuted block randomization. Randomization and concealment of allocation was accomplished by the use of sequentially numbered, sealed, opaque envelopes containing group assignment. Team members not involved in recruitment prepared the envelopes in advance. We enrolled participants and assigned allocation arm after informed consent and confirmation of eligibility.
To evaluate differences in biological outcomes, we used a two-sided log-rank test to test the null hypothesis of no difference between participants in the intervention and control arms. We used cox proportional hazards regression to estimate a HR and confidence interval (CI) comparing study arms for the composite biological indicator and each biological outcome. Models were adjusted for factors that differed between the groups at enrollment (i.e., consistent DP use, condom use self-efficacy) and STI diagnosis at enrollment. We used Kaplan–Meier curves to estimate the cumulative incidence of chlamydia, gonorrhea, trichomonas, or pregnancy, the primary outcome of interest, by 12 months.
The proportion of participants using any DP strategy, using a DP strategy at last sex, and reporting consistent use of a DP strategy, all measured during the past 3 months, was calculated by study arm. Next, we modeled behavioral indicators from assessments at 3, 6, 9, and 12 months as multinomial outcomes using generalized linear mixed models to account for repeated measures and estimate an adjusted risk ratio (aRR) comparing the study arms. Not using a DP strategy was the referent group in all models. Similarly, secondary behavioral outcomes from assessments at 6 and 12 months were assessed using appropriate summary statistics, compared using Pearson's chi-square tests or Wilcoxon rank-sum tests, and modeled using generalized linear mixed models. Stata Version 15 was used to perform all analyses.
Results
We assessed 1396 clinic attendees for eligibility; 682 were ineligible (48.9%) (Fig. 1). Not having had sex with a male partner within the past 6 months was the most frequent reason for ineligibility (n = 356). We randomized 714 participants. Twenty-four participants did not complete the enrollment visit and were disenrolled (n = 20 and n = 4 in the 2gether and control groups, respectively). Five participants in the control group were disenrolled due to pregnancy diagnosed within 4 weeks of enrollment (n = 4) or HIV diagnosis at enrollment (n = 1).
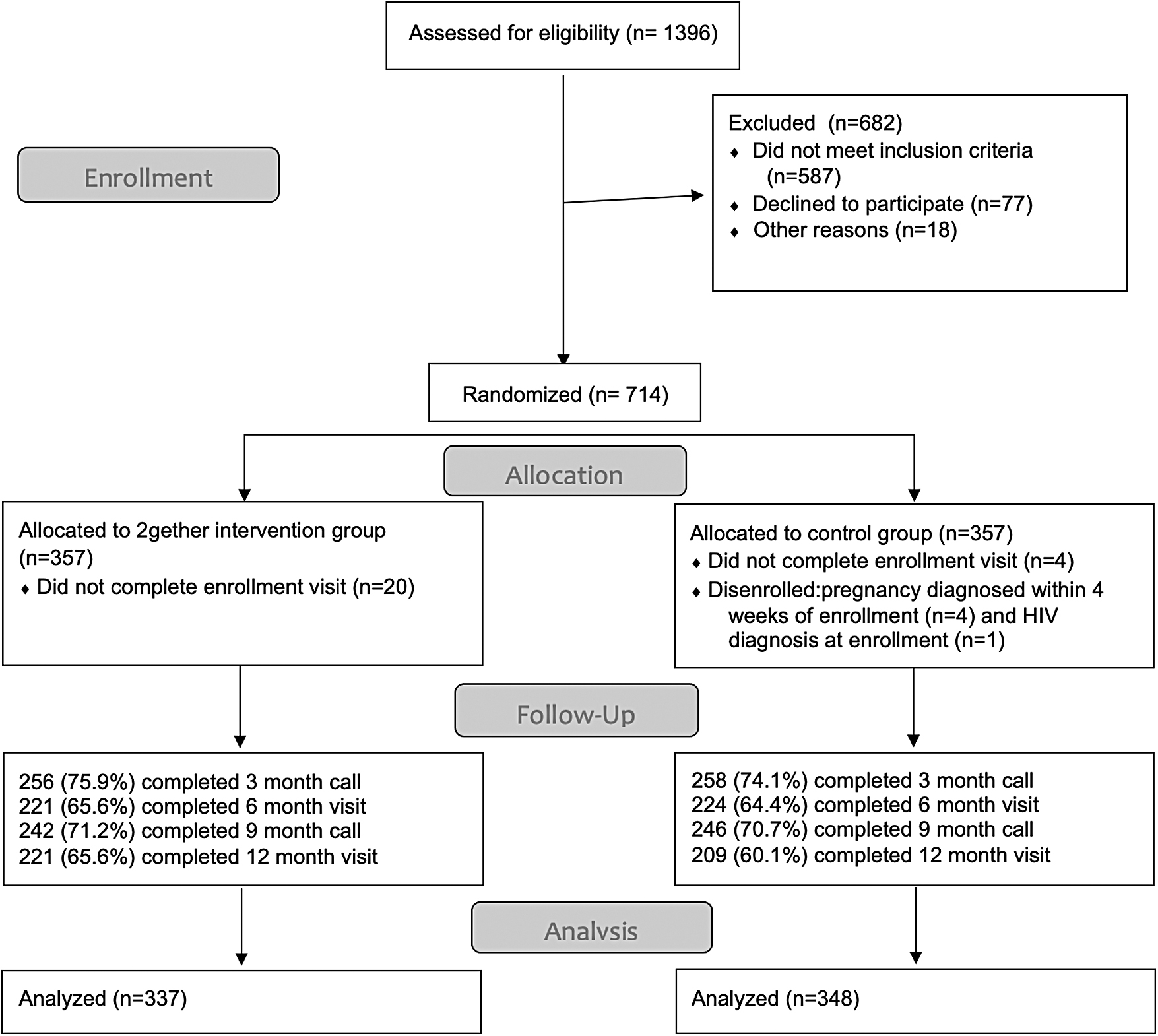
CONSORT Diagram for 2gether: A randomized clinical trial.
Accordingly, the analytic sample included 685 participants, with 337 participants in the 2gether group and 348 in the control group; an intent to treat analysis was performed. Although less than our proposed initial sample size, data capture from medical chart abstraction resulted in identification of biologic outcomes that may not have otherwise been identified and were not part of the sample size estimation. Follow-up was similar between the groups and ranged from 60% to 76% across assessment timepoints.
The average age of participants was 17 years (Table 1). The majority had not yet completed high school, received public assistance, and had public health insurance; over one quarter and one third reported a previous pregnancy or STI, respectively. At enrollment, intervention group participants were more likely to report use of no DP strategy consistently in the past 3 months (69.1% vs. 57.8%, p = 0.01); this was driven by the difference in report of consistent condom use (27.0% vs. 38.8%, p = 0.001). There were no differences in STI prevalence at enrollment.
Characteristics of Participants in the 2gether Intervention and Control Groups at Enrollment (n = 685)
DP, which is the concurrent prevention of unintended pregnancy and sexually transmitted infections. Dual method is use of condoms plus an IUD, implant, injection, ring, patch or pill.
To assess use of a DP strategy, participants were asked, “Some women and their partners choose to use two methods of contraception at the same time (together) to prevent pregnancy AND STDs. By same time I mean you use both methods when you have sex. What two methods have you used together to prevent pregnancy and STDs in the PAST 3 MONTHS?”
Consistent over past three months required use with every episode of sex over the past 3 months
2gether biologic outcomes included chlamydia, gonorrhea, trichomonas, or pregnancy. Having a negative pregnancy test at enrollment was an eligibility requirement for participation in the trial.
DP, dual protection; GED, General Educational Development; IUD, intrauterine device; SD, standard deviation; STD, Sexually Transmitted Disease.
We identified 391 events during the 12-month follow-up (Table 2). The unadjusted hazard ratio for time to any event (chlamydia, gonorrhea, trichomonas infection, or pregnancy), the primary biological outcome, showed a protective effect of the 2gether intervention (HR = 0.73; 95% CI, 0.58–0.92). The adjusted hazard ratio (aHR) was similar (aHR = 0.71; 95% CI, 0.56–0.90). The Kaplan–Meier survival curve is shown in Figure 2. Although our study was not powered to examine a difference for each biological outcome separately, significant protective associations were observed for trichomoniasis in unadjusted (HR = 0.59, 95% CI, 0.37–0.95) and adjusted models (aHR = 0.59, 95% CI, 0.36–0.94). Findings for the other individual outcomes were null.
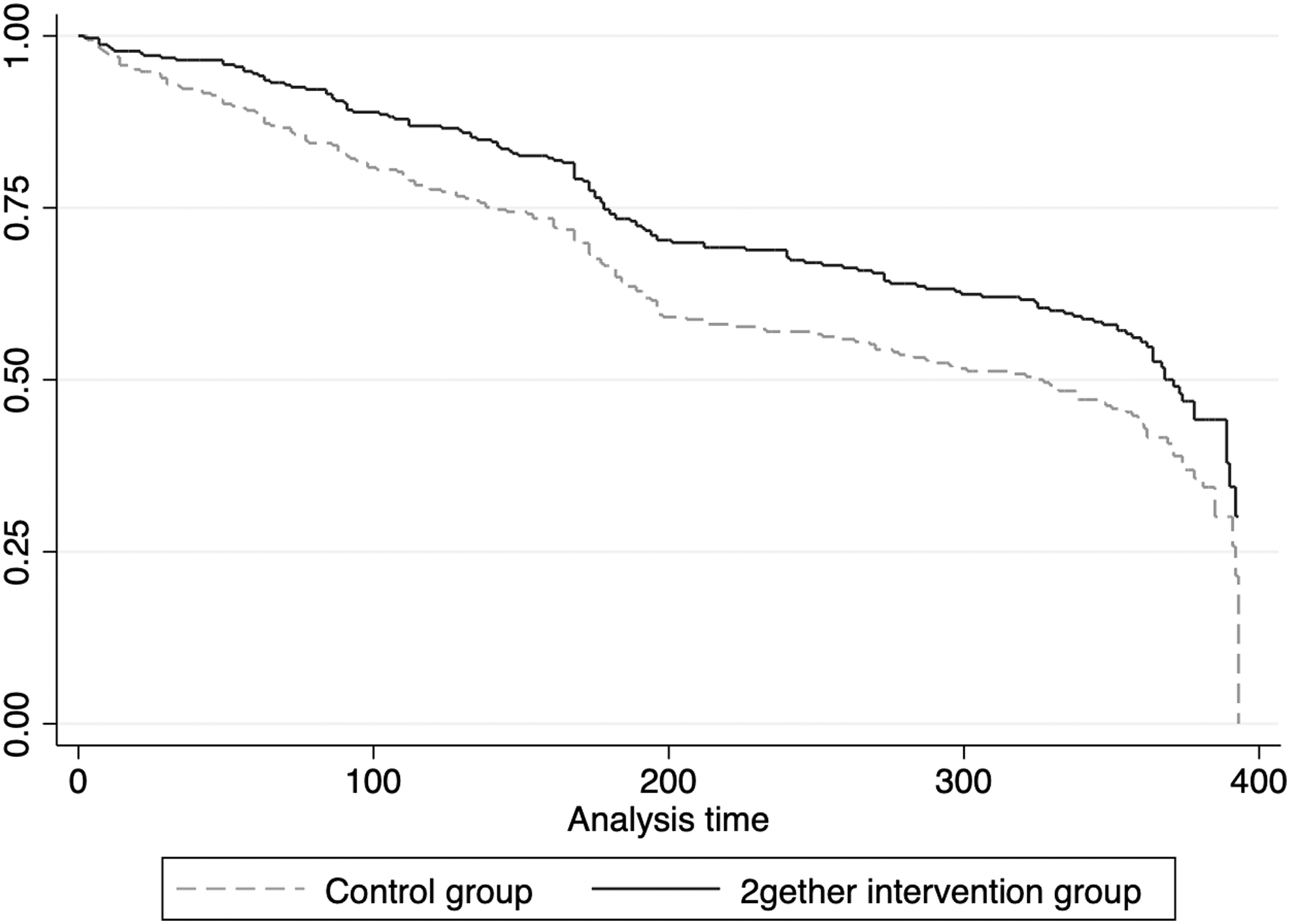
Kaplan–Meier curve of time to chlamydia, gonorrhea, trichomonas, or pregnancy for participants in 2gether intervention compared to control group (analysis time in days).
First event of Chlamydia, Gonorrhea, Trichomonas Infection, or Pregnancy During the 12-Month Follow-Up for Participants in 2gether Intervention Compared to the Control Group
Adjusted Model was adjusted for consistent dual protection use over past 3 months, condom self-efficacy, and biologic outcome at enrollment.
Numbers may not equal the sum of individual outcomes if more than one event occurred on the same day.
aHR, adjusted hazard ratio; CI, confidence interval; HR, hazard ratio; STI, sexually transmitted infection.
Over the 12-month follow-up, there were 171 outcomes (chlamydia, gonorrhea, trichomonas infection, or pregnancy) in the intervention group and 220 outcomes in the control group. Looking at our composite variable of any outcome, individuals in the intervention group had a repeat event of any outcome 43 times compared to 53 times in the control group; this was not statistically significant.
Intervention participants were more likely to report any dual method use during the past 3 months (aRR = 1.61; 95% CI, 1.15–2.26) compared with participants receiving SOC (Table 3). Examining specific types of dual method use, participants in the 2gether group were significantly more likely to report any use of implants or IUDs plus condoms in the prior 3 months (aRR = 2.11; 95% CI, 1.35–3.29); at last sex (aRR = 1.53; 95% CI, 1.01–2.33); and consistently over the past 3 months (aRR = 1.73; 95% CI 1.07–2.80). The only other significant effect observed was condom use alone as a DP strategy at last sex (aRR = 0.64, 95% CI, 0.41–0.99).
Primary and Secondary Behavioral Outcomes During the 12-Month Follow-Up for Participants in 2gether Intervention Compared to the Control Group
DP, which is the concurrent prevention of unintended pregnancy and sexually transmitted infections. Dual method is use of condoms plus an IUD, implant, injection, ring, patch, or pill.
n = number of reports from the assessments at 3, 6, 9, and 12 months.
Adjusted for baseline value.
To assess Use of a DP strategy, participants were asked: “Some women and their partners choose to use two methods of contraception at the same time (together) to prevent pregnancy AND STDs. By same time I mean you use both methods when you have sex. What two methods have you used together to prevent pregnancy and STDs in the PAST 3 MONTHS?”
Consistent use of a DP strategy was defined as being abstinent, using condoms alone with every episode of sex, or using condoms with every episode of sex plus use of an IUD, implant, injection, pill, patch, or ring currently and in the past 3 months.
Participants in the intervention arm had significantly higher contraceptive knowledge, condom and contraceptive use self-efficacy, and intention to use contraceptives, compared with the control arm (Table 3). There were no differences between study arms in STI knowledge, partner communication self-efficacy or frequency, or intention to use condoms. Reports of verbal or physical threats or abuse by a partner were not different between study arms.
We identified 55 serious adverse events in 24 participants, most commonly due to hospitalizations related to pregnancy (birth, pregnancy complications, and ectopic pregnancy) (n = 14) (details in Supplementary Data). None was determined to be related to study participation.
Discussion
Over the 12-month follow-up period, participants receiving the 2gether intervention had a lower risk of experiencing any biological event (chlamydia, gonorrhea, trichomonas infection, or pregnancy) and were more likely to report any use of dual methods during the past three months compared with participants receiving SOC. These are promising findings as previous studies aimed at increasing DP have not reported significant protective associations with biological outcomes. 21 –24 Furthermore, the 2gether intervention was associated with increased use of dual methods, specifically IUDs and implants with condoms, for all measures (any use, at last sex, and consistently in past 3 months). This is important because recent reports have found decreased condom use with implants and IUDs compared to pills, patch, and rings among adolescents. 25,26 Some have hypothesized that use of condoms with other contraception was motivated by additional pregnancy prevention rather than STI prevention. 27,28
However, the 2gether intervention intentionally focused on skills, self-perception of risk, and motivations for preventing both STIs and pregnancy simultaneously. 2gether was a novel, theoretically informed intervention that combined several strategies for supporting behavior change, including increasing knowledge, MI techniques, and use of peer role models. MI has been used successfully for adolescent behavior change, including for sexual health. 29 –32 This approach, coupled with increased knowledge and self-efficacy, as was reflected in the findings for secondary behavioral outcomes, may have led to contingency planning and the ability to apply DP use even in complex and changing circumstances.
Our participants had high rates of STIs and pregnancy. Compared with African American females aged 15–19 years across the United States in 2019, our participants had about 3.5 times and 4.5 times the rates of chlamydia and gonorrhea, respectively. 4 While reliable national data on trichomonas are not available, incidence was high in this study. Over the 12-month follow-up period, intervention participants had fewer infections of all three STIs we studied, and this was particularly true for trichomonas. Other studies have reported associations between reduced risk of trichomonas and hormonal contraception. 33,34 2gether group participants were more likely to report use of hormonal contraception compared to those in the control group; this may have contributed to the observed differences.
For too long, there has been a separation between research and programming in family planning and in HIV/STIs. This may be driven by differing expertise, funding mechanisms and setting-specific priorities. 35 Messaging tends to focus on the pros of one prevention approach for one outcome, often at the cost of the other. For example, condoms are critical for STI prevention but are less effective at pregnancy prevention. 36 In this trial, we focused on the goals of the patient to prevent both rather than an either/or approach with a simple message that “contraception and condoms are better together.” Multipurpose prevention technologies, a class of products that prevents pregnancy and some STIs, could simplify the end-user experience and potentially improve outcomes. 37 Undoubtedly, there is value in this type of technological advancement, particularly for methods that are female-controlled and not coitally dependent. 38
However, this study suggests that technology alone will be insufficient. All participants in this trial had access to the technologies necessary to prevent both pregnancy and STIs (i.e., full scope of contraceptives, condoms, STI screening, and treatment for patient and partner), offered in a clinical setting that sought to decrease common barriers (i.e., flexible clinic hours, walk-in visits, no requirements for pelvic exams, no out-of-pocket fees, same day contraceptive initiation/placement) 39 and still, pregnancy and STIs were common. This reinforces the enduring need for effective culturally sensitive behavioral interventions that address both outcomes. 12
Several limitations should be considered when interpreting these findings. First, this study was conducted in a single center with young people who identified as female and African American, limiting generalizability. While we used ACASI interview techniques and trained our staff on how to collect data around sensitive questions, social desirability bias may have influenced participant reporting of behaviors. Next, this study was unblinded, which may have influenced participants' or the study team's behaviors. This was also a multicomponent intervention; we cannot assess the contribution of each component to our findings. Finally, we conducted a thorough medical record review but may not have identified all STIs or pregnancies for participants seen at other sites during follow-up.
Although our study findings may not be generalizable to all settings, they may be valuable for other settings with high STI and pregnancy burden for young African American females. The intervention requires front-end training and integration into clinical flow; this may be challenging for clinical environments that do not engage a team approach to clinical care, those that have high staff turn-over, and those that require rapid throughput. Future implementation studies would be beneficial to determine how best to support integration in diverse settings, as well as exploring virtual and nontraditional clinical spaces. Further exploration of the most effective components of the intervention and how to enhance them will be important for scaling. In addition, inclusion of male partners will require intentional and creative efforts, but may be particularly impactful in optimizing DP.
Findings suggest that participation in the 2gether intervention resulted in increased use of a DP strategy and decreased cases of pregnancy or selected STIs among young African American females. The combination of in-depth education, MI techniques, shared decision-making, skill-building, planning for challenges, and frequent follow-up may help decrease STIs and unintended pregnancy among adolescents disproportionately affected.
Footnotes
Acknowledgment
The authors thank the study team, the clinic team, and their study participants, without whom this study would not have been possible.
Authors' Contributions
M.J.K.: Conceptualization, Data curation, Funding acquisition, Investigation, Visualization, Supervision, Writing—Original Draft, and Writing—Reviewing and Editing. J.M.S.: Conceptualization, Data curation, Investigation, Visualization, Supervision, Writing—Original Draft, and Writing—Reviewing and Editing. P.G.: Conceptualization, Data curation, Investigation, Project Administration, Visualization, Writing—Original Draft, and Writing—Reviewing and Editing. J.L.B.: Conceptualization, Data curation, Investigation, Visualization, Supervision, Writing—Original Draft, and Writing—Reviewing and Editing. K.H.T.: Conceptualization, Investigation, Visualization, Writing—Original Draft, and Writing—Reviewing and Editing. E.H.K.: Investigation, Visualization, Supervision, Writing—Original Draft, and Writing—Reviewing and Editing. J.W.H.: Formal analysis, Visualization, Writing—Original Draft, and Writing—Reviewing and Editing. J.M.K.: Conceptualization, Investigation, Visualization, Writing—Original Draft, and Writing—Reviewing and Editing. A.P.K.: Conceptualization, Investigation, Visualization, Supervision, Writing—Original Draft, and Writing—Reviewing and Editing.
Author Disclosure Statement
M.J.K. currently receives investigator-initiated funding paid to Emory University from Merck/Organon. J.L.B. receives investigator-initiated support paid to the University of Cincinnati from Gilead Sciences, Inc., The rest of the authors have no disclosures.
Funding Information
Centers for Disease Control and Prevention, Cooperative Agreement, Grant No. U01 DP003894.
Supplementary Material
Supplementary Data
Supplementary Appendix SA1
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.