
Abstract
Background:
The objectives of this study were to describe trends in the prevalence of postpartum suicidal behaviors in California, 2013–2018, and to estimate associations between adverse perinatal outcomes and suicidal behaviors.
Materials and Methods:
We used data from a population-based cohort derived from all birth and fetal death certificates. Records were individually linked to maternal hospital discharge records for the years before and after delivery. We estimated the prevalence of postpartum suicidal ideation and attempt by year. Then, we estimated crude and adjusted associations between adverse perinatal outcomes and these suicidal behaviors. The sample included 2,563,288 records.
Results:
The prevalence of postpartum suicidal ideation and attempt increased from 2013 to 2018. People with postpartum suicidal behavior were younger, had less education, and were more likely to live in rural areas. A greater proportion of those with postpartum suicidal behavior were Black and publicly insured. Severe maternal morbidity, neonatal intensive care unit admission, and fetal death were associated with greater risk of ideation and attempt. Major structural malformation was not associated with either outcome.
Conclusions:
The burden of postpartum suicidal behavior has increased over time and is unequally distributed across population subgroups. Adverse perinatal outcomes may help identify individuals that could benefit from additional care during the postpartum period.
Introduction
In the United States, suicide accounts for between 4% and 7% of pregnancy-associated deaths (i.e., deaths occurring during or within 1 year of birth). 1 –4 However, because suicide is classified as an external cause of death rather than a death directly caused by pregnancy or its management, it is often excluded from maternal mortality metrics. 1,4 –6 Limited surveillance of pregnancy-associated suicide is a barrier to characterizing the magnitude of the public health problem and, consequently, results in insufficient resources allocated for prevention and treatment. 7,8
Suicidal behaviors, including suicidal ideation and suicide attempt, often precede suicide and are in themselves associated with adverse pregnancy and neonatal outcomes. 9 –12 In a nationally representative U.S. survey administered between 2009 and 2018, 3.4% of pregnant women reported past year suicidal behavior, a construct measured with three questionnaire items capturing ideation, planning, and attempt. 13 A U.S. study using data from an administrative cohort of commercially insured individuals between 2006 and 2017 reported increasing prevalence of diagnoses for pregnancy-associated suicidal ideation (2006: 0.1% to 2017: 0.5%) and intentional self-harm (2006: 0.1% to 2017: 0.2%). 14 Both studies reported similar patterning by sociodemographic and clinical characteristics with greater prevalence among people who are younger and of lower socioeconomic status, and among those with a mental health or substance use disorder diagnosis. 13,14 Continuing to monitor population trends in postpartum suicidal behaviors is critical to support policy development and inform allocation of resources toward groups that experience the greatest burdens.
Pregnancy is a critical period during which engagement in the health care system is high, “so there are multiple opportunities for recognition and treatment, and preventing suicide.” 1 There are well-established risk factors that can be used to screen and identify individuals with elevated risk of suicidal behavior during the perinatal period. 15,16 These include younger maternal age, low education, experience of intimate partner violence, unemployment, and history of a mental health or substance use disorder. 10,16 –21 Less attention has been given to how factors arising during the perinatal period relate to postpartum suicidal behavior.
A few studies have reported that experience of a pregnancy complication, 22 cesarean birth, 23 having a baby born with low birthweight, 23 and fetal or infant death 24 are associated with greater risk of postpartum suicidal behavior. More research is needed to identify how other perinatal outcomes relate to suicide risk postpartum. This information could improve our ability to identify people who may benefit from additional resources and support in the year after birth.
In this study, we describe trends of two postpartum suicidal behaviors (suicidal ideation and suicide attempt) by sociodemographic characteristics in California between 2013 and 2018. We then describe how the prevalence of the two behaviors changed over time. Finally, we assessed whether experiencing an adverse perinatal outcome was related to increased risk of postpartum suicidal behavior. Specifically, we hypothesized that severe maternal morbidity, fetal death, having a baby admitted to the neonatal intensive care unit, or a having baby with a major structural malformation were associated with greater risk of suicidal ideation and suicide attempt.
Materials and Methods
Setting
Data for this study come from an administrative cohort of all live born infants and fetal deaths in California, 2013–2018. 25 Birth and fetal death certificates maintained by California Vital Statistics were linked to maternal hospital discharge, emergency department, and ambulatory surgery records for the years before and after delivery. These data, maintained by the California Office of Statewide Health Planning and Development (OSHPD), include up to 25 diagnosis and up to 21 procedure codes recorded using the International Classification of Diseases, 9th Revision, Clinical Modification (ICD-9; 2013 through October 2015), and the International Classification of Diseases, 10th Revision, Clinical Modification (ICD-10; October 2015 through 2018). Information from outpatient visits and diagnoses was unavailable.
To link individuals across data sources, we identified variables that were available in both vital statistics and hospitalization records. These variables included the birthing person's date of birth, hospital of birth, infant birth date, and sociodemographic and clinical characteristics of the birth (Supplementary Table S2). Lastly, linkage with California Vital Statistic death records was used to identify maternal deaths occurring up to 1 year after pregnancy. This SOMI study was approved by the California Department of Public Health and the UC San Diego Human Research Protection Program.
For the current analyses, we included singleton births occurring between 2013 and 2018. We excluded multiple gestation pregnancies and births where linkage between vital statistics and maternal OSHPD data was not possible (9%). These eligibility criteria resulted in a sample size of 2,563,288 births, including 2,551,922 live births and 11,366 fetal deaths. A comparison of those in the analytic sample and those that were excluded due to no linkage is provided in Supplementary Table S3.
Measures
Diagnoses of postpartum suicidal behavior, including suicidal ideation and suicide attempt, were determined from ICD-9 and ICD-10 codes in OSPHD data (Supplementary Table S1). 26 Suicide attempts included those due to self-inflicted poisoning (e.g., drug overdose) and intentional self-harm (e.g., firearms, hanging, and jumping from high place). The hospital admission date associated with each code and delivery date was used to categorize timing of suicidal behavior into two periods (<3 months since delivery, 3–12 months since delivery).
Most suicidal ideation codes or suicide attempt codes were identified in emergency room or hospital inpatient records, rarely in ambulatory surgery records (Supplementary Table S4). Occurrence of suicide deaths was identified from linkage to California death certificates or OSHPD hospital discharge records where discharge status was “died.”
Adverse perinatal outcomes included severe maternal morbidity, neonatal intensive care unit (NICU) admission, major structural malformation, and fetal death. Fetal death was coded if a fetal death certificate was issued, NICU admission was determined from birth records, and the other outcomes were determined from OSHPD data (Supplementary Table S1). We used the Centers for Disease Control definition of severe maternal morbidity that includes a list of 21 serious maternal outcomes (e.g., acute myocardial infarction, eclampsia, and sepsis). 27
We considered several sociodemographic variables obtained from birth and fetal death certificates. These included maternal age (<18 years, 18–34 years, and >34 years), National Center for Health Statistics urban–rural classification for county of residence 28 (large central, fringe metro, medium metro/small metro, and micropolitan/noncore), self-identified race/ethnicity (non-Hispanic White, Hispanic, Black, Indigenous, Hawaiian/Pacific Islander, Asian, two or more races, and other/not stated/unknown), education (<12 years, 12 years, >12 years, and unknown), payer for delivery (private, public, self-pay, and other), and receipt of women, infants, and children (WIC) benefits (yes, no).
Lastly, we considered whether maternal OSPHD records included any substance use-related diagnosis during pregnancy or diagnosis of a mental disorder complicating pregnancy. The ICD-9 and ICD-10 codes used to identify the substance use and mental health diagnoses are provided in Supplementary Table S1.
Statistical analysis
We described demographic characteristics of the sample stratified by diagnosis of postpartum suicidal behaviors (no suicidal behavior, suicidal ideation with no attempt, and suicide attempt). We used a chi-square analysis to test independence of each sociodemographic variable with postpartum suicidal behavior. Then, we estimated 2013–2018 prevalence of postpartum suicidal ideation and attempt and plotted trends in each variable across time. We used birth year as the time variable, so estimates should be interpreted as prevalence of suicidal behaviors among individuals giving birth in a specific year. When information on specific cause was available, we stratified suicide attempt into attempts due to poisoning versus attempts due to self-inflicted injury or self-harm.
We used modified Poisson regression with robust variances to account for individuals with more than one pregnancy. 29 We estimated crude and adjusted risk ratios (RRs) and 95% confidence intervals (CIs) for associations between each adverse perinatal outcome and each suicidal behavior. Also, we stratified the adjusted models by timing of postpartum suicidal behavior (<3 months from delivery, 3–12 months from delivery) to examine potential effect modification by time since delivery. Adjusted models included maternal age, urban–rural classification, race/ethnicity, education, payer for delivery, receipt of WIC benefits, diagnosis of a mental disorder complicating pregnancy, or a substance use-related diagnosis during pregnancy. All data management and statistical analyses were carried out using SAS 9.4.
Results
The prevalence estimates for diagnoses of postpartum suicidal ideation and attempt in California increased from 143 and 21.4 per 100,000 persons in 2013 to 198.9 and 50.2 per 100,000 persons in 2018. Most postpartum suicide attempts were due to self-inflicted poisoning (Fig. 1).

Prevalence per 100,000 of suicidal ideation and suicide attempt diagnoses, California 2013–2018. Suicide attempts include fatal and nonfatal events. Poisoning and self-harm rates do not sum to all suicide attempts because not all suicide attempts could be disaggregated and methods were not mutually exclusive.
The prevalence of suicidal behaviors varied by sociodemographic characteristics (Table 1). People with either suicidal ideation or attempt postpartum were younger and had less years of education compared with those with no suicidal behavior. A greater proportion of people with suicidal ideation or attempt lived in rural counties, were Black, Indigenous, or identified as two or more races, were publicly insured, or receiving WIC benefits. Among people with suicidal behavior, there were no meaningful differences between those who had suicidal ideation with no attempt and those with a suicidal attempt (Table 1).
Demographic Characteristics of Pregnancies With and Without Diagnosis of Postpartum Suicidal Behavior, California 2013–2018 (n = 2,563,288)
Chi-square analysis of independence yielded statistically significant results (p < 0.001) for all comparisons.
Suicide attempt includes fatal and nonfatal events.
Large central metro is the most urban (counties in MSAs of 1 million or more population), micropolitan or noncore includes the most rural counties.
AI/AN, American Indian/Alaska Native; MSAs, metropolitan statistical areas; PI, Pacific Islander; WIC, women, infants, and children.
Severe maternal morbidity was associated with 2.6 (95% CI 2.2–2.30) times greater risk of suicidal ideation and 5.8 (95% CI 4.7–7.1) times greater risk of suicide attempt. These RRs were attenuated to 1.4 (95% CI 1.2–1.6) and 3.3 (95% CI 2.7–4.1) after adjustment. Fetal death was similarly associated with risk of both outcomes. After adjustment, fetal death was associated with 2.5 (95% CI 1.8–3.4) times greater risk of suicidal ideation and 2.1 (95% CI 1.1–4.2) times greater risk of suicide attempt.
Having a baby admitted to the NICU was associated with greater risk of suicidal ideation (crude: 2.2, 95% CI 2.0–2.4; adjusted: 1.3, 95% CI 1.2–1.4) and suicide attempt (crude = 1.9, 95% CI 1.5–2.3; adjusted = 1.2, 95% CI 1.0–1.4). Having a baby with a major structural malformation was not associated with either outcome (Table 2).
Associations Between Adverse Perinatal Outcomes and Diagnoses of Postpartum Suicidal Behavior, California, 2013–2018
Adjusted RR includes adjustment for maternal age, urban–rural classification, race/ethnicity, education, payer for delivery, receipt of WIC benefits, mental disorder complicating pregnancy, or substance-related diagnosis.
Severe maternal morbidity defined using CDC criteria (21 indicators).
CDC, Centers for Disease Control and Prevention; CI, confidence interval; RR, risk ratio.
After stratifying by time since delivery, we reported a much larger association between fetal death and suicidal ideation during the first 3 months after delivery (RR = 4.1, 95% CI 2.5–6.6) compared with between 3 and 12 months after delivery (RR = 1.9, 95% CI 1.9–1.3, 2.9). The size of other exposure–outcome associations did not meaningfully vary by time since delivery (Fig. 2).
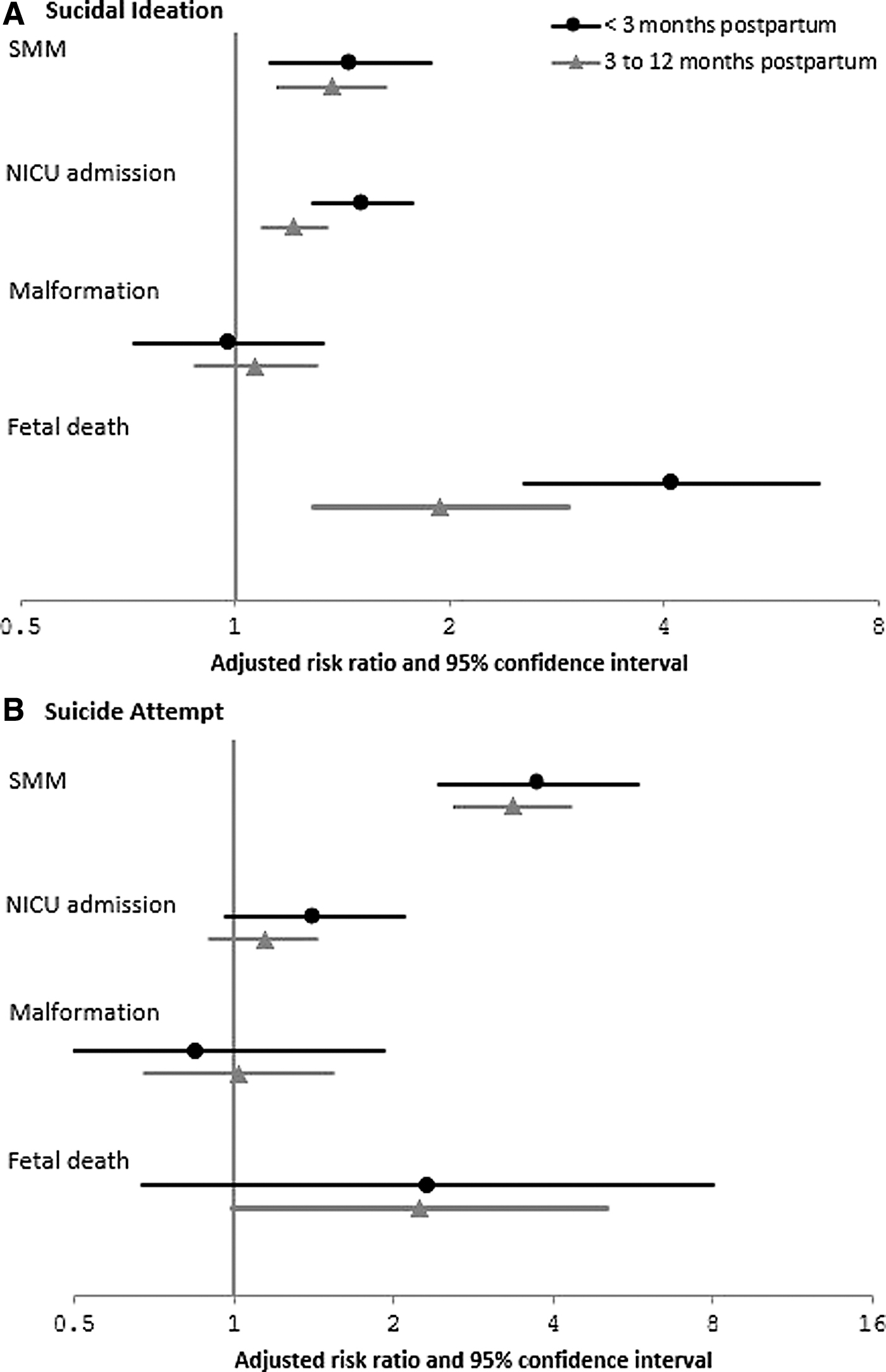
Associations between adverse perinatal outcomes and diagnoses of postpartum suicidal behavior stratified by time since birth, 2013–2018. Adjusted RR includes adjustment for maternal age, urban–rural classification, race/ethnicity, education, payer for delivery, receipt of WIC benefits, mental disorder complicating pregnancy, or substance-related diagnosis. RR, risk ratio; WIC, women, infants, and children.
Discussion
In an administrative cohort of California births between 2013 and 2018, we characterized the prevalence of postpartum suicidal ideation and attempt in a California population-based cohort study. We reported that the prevalence of diagnosed suicidal ideation and suicide attempt has increased across time, that most suicide attempts were caused by self-inflicted poisoning, and that there was substantial variation by sociodemographic characteristics. In addition, we estimated associations between adverse perinatal outcomes and postpartum suicidal behaviors. We reported that severe maternal morbidity, NICU admission, and fetal death were associated with higher risk of postpartum suicidal behavior. We reported that having a baby with a major structural malformation was not associated with the same outcomes.
Our report of rising prevalence of both suicidal ideation and attempt parallels the trends reported in a recent study using claims data for a U.S.-wide national commercially insured population. 14 However, we note that the studies are not directly comparable because that study aggregated diagnoses of suicidal behavior from 1 year before and 1 year after pregnancy, whereas we examined diagnoses only in the year after pregnancy. Nonetheless, both administrative studies substantially underestimate the prevalence of suicidal ideation and attempt reported in observational studies using self-reported measures of suicidality, which are five to seven times greater in magnitude. 10,13,17 Thus, we can infer that the majority of cases are not being detected and/or diagnosed in clinical settings.
Several of the sociodemographic correlates of suicidal behavior identified in this study—younger age, Black race, and socioeconomic disadvantage—are well established. 7,10,14,17,30 Our study also adds data showing a disproportionate burden of suicidal behavior among Indigenous people and among those living in rural settings. These demographic data are critical in identifying high-risk populations and determining where resources for prevention and treatment should be prioritized.
Our finding that experience of fetal death was strongly associated with suicidal ideation and attempt supports prior research from Washington State, which reported three times greater risk of suicide attempt postpartum after a fetal or infant death, 24 and Taiwan, which reported five times greater odds of completed suicide after fetal loss. 31 We add that the association between fetal death and suicidal ideation was much larger during the first 3 months postpartum, perhaps when the grief of losing the baby is most intense. Of note, we did not observe the same attenuation of effect for the association between fetal death and suicide attempt. Experiencing a fetal death was associated with over two times greater risk of attempt in both time periods (<3 months and 3–12 months postpartum). Considering the consistency of these findings across settings, prevention efforts must focus on improving access to psychological services for postpartum individuals after fetal loss, particularly in the first few months after the end of pregnancy.
We reported that the adverse perinatal outcome most strongly associated with suicide attempt was severe maternal morbidity, and that this association did not attenuate after 3 months postpartum. Severe maternal morbidity is a composite outcome that includes life-threatening conditions during pregnancy or childbirth, such as eclampsia, acute myocardial infarction, and sepsis. These events are serious, stressful, and negatively affect maternal mental health. For example, women who experience severe maternal morbidity have two to three times greater odds of postpartum depression 32 and post-traumatic stress disorder 33,34 compared with women with healthy pregnancies.
An administrative study using hospitalization data from Florida showed that even among women without pre-existing psychiatric conditions, those who experienced severe maternal morbidity had increased odds of a hospitalization or emergency room visit for depression, anxiety, and psychosis within 1 year of delivery. 34 Our study adds to this evidence base that severe maternal morbidity is also associated with increased risk of suicide ideation and attempt. These findings are consistent with findings from a New York City study that reported that individuals with pregnancy complications had nearly five times higher odds of postpartum suicidal ideation than individuals without complications. 22
The mechanisms contributing to these associations are likely varied and should be studied in future research. It may be that the stress that comes with experience of severe maternal morbidity causes increased suicidal ideation and attempt, or it may be that these associations are due to unmeasured confounding. Regardless of whether these relationships are causal, these events serve as important flags for predicting which individuals may benefit from increased screening and resources after pregnancy.
The last two outcomes we examined in relation to postpartum suicidal behavior were having a baby admitted to the NICU and having a baby with a major structural malformation. Infant admission to the NICU is an established risk factor for postpartum depression, and universal postpartum mental health screening for parents of NICU babies is recommended. 35 We reported that NICU admission was associated with a small (20%–30%) increased risk of suicidal ideation and attempt. Unfortunately, we were not able to measure whether an individual received maternal mental health screening or resources while their baby was in the NICU. Future research should investigate the modifying effects of maternal interventions received in the NICU setting.
Regarding having a baby with a major structural malformation, much less is known. A couple of studies have reported increased psychological distress during pregnancy after diagnosis of a congenital anomaly. 36,37 We did not find any evidence to suggest that having a baby with a major structural malformation was associated with postpartum suicidal behavior.
Several methodological limitations should be considered. These data cannot inform whether rising trends in suicidality reflect increases in the experience of suicidal behaviors or increased detection of suicidal behaviors. Future research interested in identifying causes of pregnancy-associated suicidal behavior will need to disentangle those concepts. Also, the United States transitioned from the ICD-9-CM to ICD-10-CM coding scheme to classify diagnoses in 2015. The wording of intentional self-harm codes changed from “suicide and self-inflicted injury” in ICD-9-CM to “intentional self-harm” in ICD-10-CM. Furthermore, the ICD-10-CM introduced suicide attempt as its own code, distinct from intentional self-harm. These changes may have resulted in differential capture of suicidality across years and should be considered when examining time trends. 38,39
Also, we present data from 5 years, a period of time that may be too small to draw meaningful conclusions regarding the stability or drivers of these trends. However, these data serve as a baseline as we plan to continue monitoring suicidal outcomes as more years of data become available.
Lastly, we likely underestimate the true prevalence of pregnancy-associated suicidality for a couple of reasons. We ascertained occurrence of suicidal behavior by OSHPD discharge code. Thus, people who did not seek care or were not admitted to the hospital would not be recorded. 8 Also, people may not feel comfortable disclosing their suicidal behavior and, in some cases, may not have even been asked about suicidality by their providers. These factors likely vary by health care setting (e.g., hospitalization and emergency room) and provider characteristics that are not measured in this study.
Conclusions
This study provides data showing that the burden of suicidal behavior in the year postpartum is growing and is unequally distributed across population subgroups. Surveillance of suicidal behaviors in this population is poor despite increasing recognition and dialogue surrounding maternal mental health. These data contribute to filling this gap. Pregnancy and the postpartum period mark critical periods in one's life when people tend to have increased engagement in health care, thus, it is an optimal time to intervene.
Focused efforts to screen pregnant and newly postpartum people and identify individuals who can be connected to additional care are of high priority. 1,4 Expansion of policies and programs such as home visiting and peer support programs, telehealth, and extension of national Medicaid coverage through at least the first year after pregnancy are examples of strategies that could substantially improve detection and treatment of pregnancy-associated suicidality. 40
Footnotes
Author Disclosure Statement
Financial interests. C.C. has received research funding from the following industry sponsors and a foundation: Amgen, Inc.; AstraZeneca; Celgene; GlaxoSmithKline; Janssen Pharmaceuticals; Pfizer, Inc.; Regeneron; Hoffman La-Roche-Genentech; Genzyme Sanofi- Aventis; Takeda Pharmaceutical Company Limited; Sanofi; UCB Pharma, USA; Sun Pharma Global FZE; Gilead; and the Gerber Foundation. These entities had no role in the study design, collection, analysis, interpretation of data, or writing this report. The other authors have no relevant financial or nonfinancial interests to disclose.
Funding Information
The San Diego Study of Outcomes in Mothers and Infants (the “SOMI Study”) is funded by the Rady Children's Institute for Genomic Medicine. Additional sources of funding include NIH/NICHD R01HD101540 (PI: C.C.) and NIH/NIAAA K01AA027811 (PI: G.B.).
Supplementary Material
Supplementary Table S1
Supplementary Table S2
Supplementary Table S3
Supplementary Table S4
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.