
Abstract
Background:
Mastitis is a common disorder among postpartum women. The discomfort and pain caused by mastitis may lead to the discontinuation of breastfeeding. Large-scale epidemiological studies examining mastitis are limited. Accordingly, the present study used a nationwide population-based database to collect information about all postpartum women in Taiwan to determine the incidence of and related factors for mastitis.
Materials and Methods:
This retrospective population-based study used the National Health Insurance Research Database to collect records of patients with mastitis during 2008–2017 and then linked the collected data to the Taiwan Birth Registry. We included women diagnosed as having lactational mastitis within 6 months of delivery. A multivariable logistic regression model was used to compare the risk of mastitis between parity in multiparous women.
Results:
We identified 1,686,167 deliveries in 1,204,544 women. 19,794 women with 20,163 deliveries had a medical claim for mastitis. The incidence proportion of mastitis for 6 months postpartum was ∼1.19% and highest during the first month after delivery. Multivariable logistic regression revealed that multiparous women with a history of mastitis were likely to experience mastitis again after subsequent deliveries (adjusted odds ratio = 5.86; 95% confidence interval = 5.21–6.58). The Kaplan–Meier curve indicated that primiparous women had a higher risk of mastitis than did multiparous women (log-rank test, p < 0.001).
Conclusion:
Mastitis generally occurred during the first month postpartum, and primiparous women had a higher risk of mastitis than did multiparous women. Furthermore, multiparous women with a history of mastitis had a 5.86-fold increased risk of recurrence during subsequent deliveries.
Introduction
Mastitis is a common inflammatory reaction in postpartum women, which may or may not be related to infection. It is also called lactational mastitis or puerperal mastitis. Possible causes of mastitis are milk duct congestion due to insufficient removal of milk during breastfeeding or bacterial infection of the breast tissue due to small wounds caused by an infant's suckling. Staphylococcus aureus is commonly found in women with mastitis. 1
The symptoms of mastitis are breast swelling, redness, warm to touch, tenderness, or lumps; these symptoms are occasionally accompanied by general malaise or tiredness, fever, chills, or flu-like symptoms. Studies have estimated that breastfeeding women have a 2%–33% chance of developing lactation mastitis 2 and that 20% of Australian women who still breastfeed 6 months after giving birth experience mastitis. 3 Therefore, mastitis is a major problem for postpartum women.
Mastitis may result in abscesses 4 —localized collections of tissue fluid and purulent material—creating a painful lump on the breast. Treatment options for mastitis include antibiotics, analgesia, percutaneous drainage, and surgical incision and drainage. 5
The discomfort and pain caused by lactational mastitis may lead to the discontinuation of breastfeeding. 4,6,7 However, the World Health Organization recommends exclusive breastfeeding for babies during the first 6 months of life, followed by continued breastfeeding with appropriate complementary foods for up to 2 years or beyond. The American Academy of Pediatrics recommends that breastfeeding should begin as early as possible after birth because breast milk is the best source of nutrients for most babies. 8,9 To avoid mastitis leading to the cessation of breastfeeding, 10 developing measures for preventing and managing mastitis in postpartum women is imperative.
Studies on mastitis have relied on questionnaires or telephone interviews, in which they queried patients' subjective feelings to determine the symptoms, risk factors, and incidence of mastitis. 11 –14 Large-scale epidemiological studies on mastitis are limited, and only a few studies on this topic have used insurance claims data. 15 Accordingly, the present study used a nationwide population-based database to obtain information about all postpartum women in Taiwan to determine the incidence of and related factors for mastitis. Our study findings can increase the understanding of the etiology of this disorder and identify specific groups that can benefit from preventive measures.
Materials and Methods
Data sources
In this retrospective population-based study, we used the National Health Insurance Research Database (NHIRD) to collect the records of patients who were diagnosed as having lactational mastitis (International Classification of Diseases, Ninth Revision, Clinical Modification [ICD-9-CM] code 675.X; International Classification of Diseases, Tenth Revision, Clinical Modification [ICD-10-CM] code O91.X) within 6 months of delivery during 2008–2017, and we linked the collected data to the Taiwan Birth Registry (TBR). Taiwan's National Health Insurance (NHI) program was implemented in March 1995 and covers 99.5% of the population of Taiwan. 16
We searched the NHIRD for records of inpatient and outpatient visits, which contained not only information on medical records, such as date of visit for outpatient, date of admission, and discharge for hospitalization but also prescription details for the type of antibiotics and analgesia; duration, and total expenditure, and furthermore, medical treatments such as needle aspiration, incision, and drainage or operations, comorbid disorders during pregnancy, and medical diagnoses (which were based on ICD-9-CM codes before 2016 and on ICD-10-CM codes after 2016). Patient characteristics such as age at delivery, nationality, income level, and urbanization level were also obtained from the database.
Taiwanese law stipulates that any fetus born in hospitals or clinics or delivered by midwives, regardless of whether it is a live birth or stillbirth, must be reported to the local household register and health authorities within 10 days after labor. The TBR records information on live births and stillbirths of neonates weighing >500 g or having a gestational age of >20 weeks. In this study, we collected detailed information regarding gestational age, birth weight, delivery method, parity, and maternal age at delivery, in addition to information regarding whether neonates were single or multiple births. Studies have demonstrated the reliability of TBR data concerning neonatal and maternal outcomes. 17
Study cohort
We enrolled women who had given birth between January 1, 2008, and December 31, 2017, and had birth records, including the delivery time, in the TBR. We included women who received a diagnosis of lactational mastitis (ICD-9-CM code 675.X; ICD-10-CM code O91.X) within 6 months after delivery. Moreover, we excluded women who were not enrolled in the NHI program, died during delivery, or had a stillbirth; to confirm new-onset disease postpartum, we also excluded women who received a diagnosis of antepartum mastitis (ICD-9-CM codes 675.03, 675.13, 675.23, 675.83, 675.93; ICD-10-CM codes O91.01X, O91.11X, O91.21X) within 6 months after delivery or received a diagnosis of mastitis (ICD-9-CM code 675.X; ICD-10-CM code O91.X) during pregnancy. Finally, we excluded women who had ever received a diagnosis of inflammatory disorders of the breast (ICD-9-CM code 611.0; ICD-10-CM code N61).
Outcome
We obtained mastitis diagnoses that were obtained by linking the data collected from the NHIRD to the TBR. We searched both outpatient and inpatient claims data in the NHIRD and identified women who received physician-assigned mastitis diagnoses based on ICD-9-CM and ICD-10-CM codes (ICD-9-CM code 675.X and ICD-10-CM code O91.X).
Covariates
The covariates considered in this study were maternal age (from <20 to ≥45 years, divided into 5-year intervals), weeks of pregnancy (<37, 37–41, or ≥42 weeks), single or multiple births, delivery method (vaginal, forceps/vacuum, or caesarean section), nationality (Taiwanese, Chinese, Southeast Asian, or Northeast Asian), comorbidities, urbanization level, and income level. Comorbidities were considered to be possible confounding factors and included gestational diabetes (GDM; ICD-9-CM code 648.0; ICD-10-CM code O24.X), gestational hypertension (ICD-9-CM codes 642.0–642.3; ICD-10-CM codes O10.X, O13.X), and antepartum hemorrhage (ICD-9-CM code 641.X; ICD-10-CM codes O26.85, O46.X). Comorbidities were defined as those occurring within 6 months before delivery day.
Statistical analysis
Demographic and clinical characteristics are presented as numbers and percentages. Categorical variables were examined using the Pearson's chi square test, and continuous variables were assessed using the Kruskal–Wallis test. A multivariable logistic regression model was used to compare the risk of mastitis after subsequent deliveries with that after the first delivery in multiparous women, and the odds ratios (ORs) were adjusted for nationality, age at first delivery, years between deliveries, number of deliveries, methods of delivery, and comorbid disorders during pregnancy. For primiparous and multiparous women, the incidence of mastitis was defined as the number of events divided by the total person-months, and the cumulative incidence was estimated using the Kaplan–Meier method.
The parity groups were compared by calculating incidence rate ratios (IRRs) along with 95% confidence intervals (CIs) and by using the log-rank test. A p value of <0.05 was considered statistically significant for all statistical tests and regression models. All statistical analyses were performed using SAS 9.4 (SAS Institute, Inc., Cary, NC, USA).
Institutional Review Board statement
Ethical approval was obtained through the Institutional Review Board (IRB) of Chang Gung Medical Foundation, Chiayi, Taiwan (IRB 202200695B0). They reviewed the study proposal and deemed it Exempt.
Results
We identified a total of 2,001,043 deliveries from 1,399,684 women for the period between 2008 and 2017. Of these deliveries and women, we excluded women who were not enrolled in the NHI program; deliveries involving maternal death on the day of delivery; deliveries involving stillbirths; and women diagnosed as having antepartum mastitis, mastitis during pregnancy, or inflammatory disorders of the breast (Fig. 1). Because these conditions may have occurred more than once, data for both the excluded women and the number of corresponding deliveries were considered. Finally, 1,204,544 women with 1,686,167 deliveries were included in our analysis. Of these, 19,794 women with 20,163 deliveries had a medical claim for mastitis.
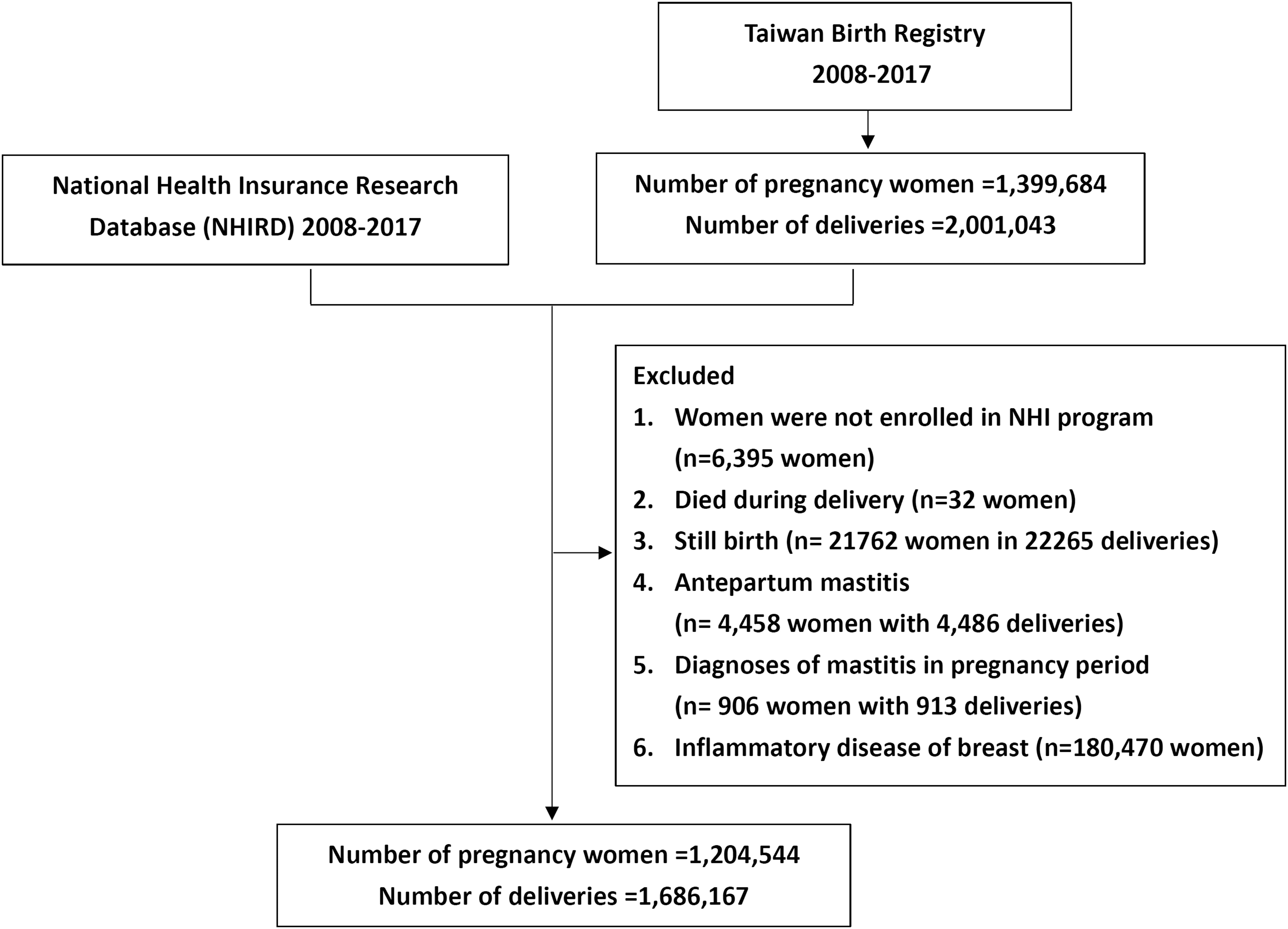
Flowchart for patient selection.
Table 1 presents the characteristics of the included women. Most of them were aged 30–34 years (39.2%). Of the included women, 4.1% and 3.8% were of Chinese and Southeast Asian nationalities, respectively. Table 2 presents the demographic characteristics of women with and without mastitis in each pregnancy and delivery. Women aged 30–34 years tended to be susceptible to mastitis (1.3%); the mean (standard deviation) ages of women with and without mastitis were 31.0 (4.5) and 31.1 (4.9) years, respectively. Moreover, A relatively high proportion of primiparous women (1.4%) suffer from mastitis, also had comorbidity of GDM (2.1%) during pregnancy.
Characteristics of Postpartum Women in Taiwan from 2008 to 2017
The Demographic Characteristics of Women With and Without Mastitis in Each Pregnancy and Delivery
SD, standard deviation.
Table 3 presents the incidence of mastitis after the second delivery of multiparous women compared with that after their first delivery. Our multivariable logistic regression model revealed that multiparous women who had a history of mastitis after their first delivery were at a higher risk of mastitis after their second delivery. The adjusted OR was 5.86 (95% CI = 5.21–6.58).
The Incidence of Mastitis After the Second Delivery with That After the First Delivery in Multiparous Women
Adjusted for nationality, age at first delivery, years between deliveries, number of deliveries, methods of delivery, and comorbid disorders during pregnancy.
CI, confidence interval; OR, odds ratio.
The incidence of mastitis 6 months postpartum was 2.38 (95% CI = 2.34–2.42) per 1000 person-months in primiparous women and 1.56 (95% CI = 1.52–1.59) in multiparous women, indicating that primiparous women had a greater risk of mastitis compared with multiparous women (IRR = 1.53; 95% CI = 1.48–1.57). In addition, the incidence proportion of mastitis for 6 months postpartum was ∼1.19% (20,163/1,686,167). We estimated the cumulative incidence of mastitis among primiparous and multiparous women. The derived Kaplan–Meier curve indicated that primiparous women had a higher risk of mastitis (log-rank test, p < 0.001). The occurrence rate of mastitis is illustrated in Figure 2.
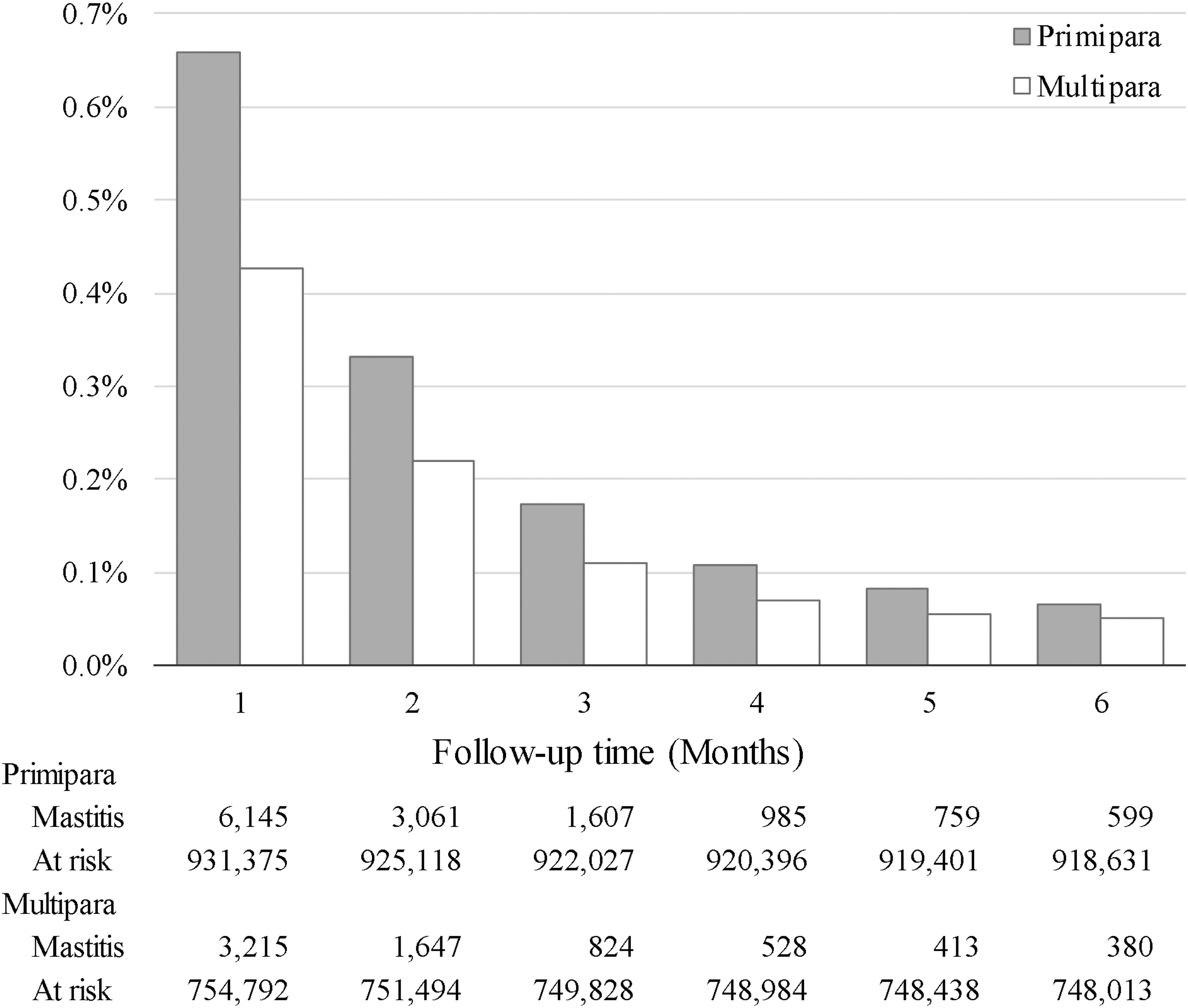
The occurrence rate of mastitis.
For both primiparous and multiparous women, the highest occurrence rate of mastitis was noted during the first month after delivery, and this rate was almost halved during the second month. Although primiparous women had a higher incidence of mastitis than did multiparous women, the incidence rate decreased with time until 6 months postpartum.
To determine the medical utilization rate for mastitis, we analyzed data on the history of medications and treatments from the NHIRD. Antibiotics (78.8%) and analgesia (79.1%) were the most common treatment for mastitis. More invasive medical treatments such as needle aspiration (1.9%) and incision and drainage (2.6%) were rarely used. Most of the patients with mastitis were treated through outpatient care; only 3.5% of the patients required hospitalization.
Discussion
According to our review of the literature, this is the first national cohort study to explore the incidence of and related factors for mastitis in an Asian country. Our results reveal that women with comorbid diabetes were susceptible to mastitis. The literature indicates that delayed onset of lactogenesis could occur in one-third of women with GDM. Women with GDM experience difficulty in expressing colostrum, which often occurs during the first 2 days after delivery. The overall effect of delayed milk production and excretion could be the possible link between GDM and mastitis. Furthermore, mastitis creates an inflamed environment that raises blood sugar levels and quickly exacerbates diabetes. 18
We observed that multiparous women with a history of mastitis after their previous delivery had a 5.86-fold increased risk of mastitis after their second delivery. Wilson et al 6 conducted a systematic review to determine whether women with a history of mastitis would be at an increased risk of mastitis during their next lactation. Multiple risk factors were assessed and reported to be associated with lactational mastitis. Women who previously had mastitis because of improper breastfeeding techniques or poor hygiene may experience mastitis again during their future lactation periods. 19 Therefore, mastitis recurrence must be prevented; this can be achieved through early treatment for damaged nipples, aggressive management of breast engorgement, and early intervention to aid in positioning and attachment, which can reduce the risk of mastitis.
In our study, the incidence proportion of mastitis for 6 months postpartum was 1.19% (20,163/1,686,167). The incidence proportion was highest during the first month postpartum (46.4%; 9,360/20,163) and then declined thereafter. These results are similar to those of previous studies. For example, Scott et al 7 reported that the incidence proportion of mastitis in a Scottish cohort was 18% (74/420) and that approximately half of the cases (30/57) occurred during the first month postpartum. Similarly, Amir et al 11 demonstrated that 17% (206/1,193) of women experienced mastitis and that 53% (194 of 365) of the cases occurred during the first month postpartum.
In addition, they revealed that the incidence proportion of mastitis in primiparous women was 65.2% (13,156/20,163), which was significantly higher than that observed in multiparous women. Shahin et al 20 reported that 66.6% (33/45) of mastitis cases occurred in primiparous women. By contrast, Egbe et al 13 revealed that the incidence proportion of mastitis was 68.6% in multiparous women, which was higher than that observed in primiparous women.
The differences in the incidence proportions among the aforementioned studies may be explained by the differences in the definitions of mastitis, differences in populations, selection bias, and other unmeasured factors. Egbe et al 13 inferred that when medical records were used for examination, the incidence proportion of mastitis was <10%, but when self-reported symptoms were used for examination, the incidence proportion was >20%. Wilson et al 6 indicated that the incidence of mastitis varies widely; although the reason for this extensive variation was unknown, they speculated that diagnoses based on questionnaire and interview responses would be influenced by differences in the respondents' expectations, perceptions, and subsequent reporting of symptoms.
In our study, mastitis was diagnosed by specialist physicians, and women were identified using diagnostic codes from the NHIRD; therefore, the accuracy of the diagnoses should be reliable. A possible reason for the lower incidence proportion in our study compared with those reported by previous studies is that some women do not seek medical treatment for mild lactational mastitis but instead opt for breast massage, self-management, or other remedies that do not require an insurance claim; because of the nature of our screening process, these women would have been overlooked in our study.
Another possible reason is that most of the previous studies have utilized questionnaires or telephone interviews, 6,11 –14 limiting the sample size and influencing enrollment conditions due to patient emotions, recall difference, and selection bias. By contrast, we had a large denominator, and our nationwide cohort comprised all postpartum women, including those who were not at risk of lactational mastitis because their babies were weaned or not breastfeeding.
Breastfeeding women may be reluctant to take medications because of concerns about the medications affecting their child; they may instead seek physiological methods to reduce the symptoms of mastitis. However, if the symptoms are not resolved, they may opt for antibiotic treatment. According to statistics regarding medications for mastitis treatment in Taiwan, oral drugs constitute the main treatment. We noted that antibiotics were administered to 78.8% (15,894/20,163) of patients and that analgesics were administered to 79.1% of patients. Osterman et al 21 reported that because of the potential presence of pathogenic bacteria in milk, 61% of women in Sweden with mastitis opted for antibiotic therapy. Fetherston et al 22 revealed that 85% of breastfeeding mothers in Australia took antibiotics for mastitis.
The question regarding the necessity of the use of drugs for mastitis is controversial. A Cochrane review indicated that evidence is insufficient to confirm or deny the effectiveness of antibiotics for mastitis treatment; nevertheless, antibiotics could alleviate discomfort rapidly in cases of infectious lactation mastitis. Physicians primarily prescribe dedications on the basis of clinical symptoms. 2,23
Limitations
This study has several limitations. First, risk factors for mastitis include breastfeeding and other related factors such as nipple damage, milk stasis, and maternal stress; however, we could not obtain data regarding breastfeeding status in the medical records collected from the NHIRD. Second, women with mastitis have several options to relieve their discomfort. Some women tend to avoid clinics and hospitals but instead seek a massagist or lactation consultant to relieve their discomfort. These methods are nonpharmaceutical intervention and not considered as medical practice, therefore which are not covered by NHIRD. Our study may have overlooked these groups, which may result in data bias.
Conclusions
Mastitis often occurred during the first month after delivery, and primiparous women were at a higher risk of mastitis than multiparous women. Furthermore, multiparous women with a history of mastitis had a 5.86-fold increased risk of recurrence. The identification of these at-risk groups can enable the provision of early intervention and implementation of precautions against mastitis.
Footnotes
Acknowledgments
We thank Health Information and Epidemiology Laboratory of Chang Gung Memorial Hospital, Chiayi Branch, for the comments and assistance in data analysis.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This study was supported by a grant (No. CLRPG6N0041) from Chang Gung Memorial Hospital.