
Abstract
Background:
Depression affects one in seven perinatal individuals and remains underdiagnosed and undertreated. Individuals with a psychiatric history are at an even greater risk of perinatal depression, but it is unclear how their experiences with the depression care pathway may differ from individuals without a psychiatric history.
Methods:
We conducted a secondary analysis evaluating care access and barriers to care in perinatal individuals who screened positive for depression using the Edinburgh Postnatal Depression Scale (N = 280). Data were analyzed from the PRogram in Support of Moms (PRISM) study, a cluster randomized controlled trial of two interventions for perinatal depression.
Results:
Individuals with no prepregnancy psychiatric history (N = 113), compared with those with a history (N = 167), were less likely to be screened for perinatal depression, and less likely to be offered a therapy referral, although equally likely to attend if referred. When examining how these differences affected outcomes, those without a psychiatric history had 46% lower odds of attending therapy (95% confidence interval [CI]: 0.19–1.55), 79% lower odds of taking medication (95% CI: 0.08–0.54), and 80% lower odds of receiving any depression care (95% CI: 0.08–0.47). Barriers were similar across groups, except for concerns regarding available treatments and beliefs about self-resolution of symptoms, which were more prevalent in individuals without a psychiatric history.
Conclusions:
Perinatal individuals without a prepregnancy psychiatric history were less likely to be screened, referred, and treated for depression. Differences in screening and referrals resulted in missed opportunities for care, reinforcing the urgent need for universal mental health screening and psychoeducation during the perinatal period. Clinical Trial Registration No.: NCT02935504.
Introduction
Perinatal depression is among the most common complications of pregnancy, 1 –3 and has wide-ranging negative effects on both maternal and child outcomes including breastfeeding, bonding, and early childhood development. 4 –7 Beyond these negative impacts on families, it contributes to preventable maternal mortality in the United States. 8 Despite the high prevalence, known complications, and recommendations from the American College of Obstetricians and Gynecologists (ACOG) 9 and the US Preventative Services Task Force 10 for routine screening, perinatal depression continues to be underdiagnosed and undertreated. 11
The pathway from symptom recognition to successful treatment is complex and multistep. 12 Gaps between care needs and receipt of care include patient and provider-level factors that span psychiatric illness-related stigma to inadequate number of psychiatric providers. 13,14 Some barriers to accessing care for perinatal depression overlap with risk factors for its development, resulting in a double vulnerability. Among known risk factors, a personal history of psychiatric illness places an individual at a greater than twofold increased risk of depression in the perinatal period. 15,16 However, few studies of perinatal mental health have explored how psychiatric illness before pregnancy impacts how individuals are screened, diagnosed, and ultimately receive care for perinatal depression.
Using data from the PRogram in Support of Moms (PRISM) study, a randomized controlled trial evaluating perinatal depression interventions, 17 we examined how access to perinatal depression care and reported barriers to care differ between perinatal individuals with and without a prior psychiatric history.
Methods
Study population
We conducted a secondary analysis of data from the PRISM study. 17 This randomized controlled trial, conducted from 2017 to 2022, included 10 obstetric practices randomized into either (1) the population-level intervention Massachusetts Child Psychiatry Access Program (MCPAP) for Moms, or (2) the MCPAP for Moms program plus a practice-level intervention with implementation support. 17 Obstetric settings included ambulatory academic and private practice offices, and health care professionals included physicians, nurses, midwives, and other staff. The study enrolled perinatal individuals who screened positive for depression on the Edinburgh Postnatal Depression Scale (EPDS) during pregnancy or within the first 3 months postpartum, using a cutoff score of 10 or greater as a positive screen. 18,19
For the purposes of this study, data from the two arms were pooled. The final data set consisted of 280 perinatal individuals who had completed the study and answered the question on past psychiatric history at their initial interview. Participants were considered to have a prior psychiatric history if they answered yes to the question, “Before this pregnancy, did you ever receive a mental health diagnosis from a healthcare professional?.” The PRISM study was approved by the IRB of the University of Massachusetts Chan Medical School.
Measurement of care access
Assessment of participants' access of perinatal depression care was gathered through self-report surveys. Participants completed between three and five surveys depending on when they screened-in to the study with a positive EPDS (4–24 weeks gestation, 32–40 weeks gestation, or 1–3 months postpartum). Participants were asked if they had (1) been screened for perinatal depression during obstetric care, (2) been offered or referred to mental health treatment, and (3) if they accepted or declined treatment. Participants who responded that they had been offered mental health treatment were asked to specify what type (individual therapy, support groups, or medication treatment). If they were offered a referral to either individual therapy or a support group, they were asked whether they were currently participating. Participants were also asked if they were currently prescribed psychiatric medications for depression, and if they were prescribed psychiatric medications before they were pregnant.
Participants were considered to have accessed care if they reported they had either participated in therapy or taken psychiatric medication during the study period. Each step in the pathway from screening to treatment was analyzed independently and compared between those with and without a psychiatric history. Finally, the cumulative measure of care access through either therapy or prescription medication was assessed and compared between groups.
Measurement of barriers to care
Assessment of barriers to perinatal depression care was carried out using the Barriers to Access to Care Evaluation (BACE) (Supplementary Fig. S1). The BACE is a validated 30-item tool for assessing barriers to help-seeking for psychiatric illness. 20 Each survey item is rated on the degree to which it “stopped, delayed, or discouraged [them] from getting or continuing with professional care for a mental health problem,” with 0 being “not at all” and 3 being “a lot.” The scale can be separated into three subscales: stigma-related, attitude-related, and instrumental barriers. The stigma subscale assesses the degree to which perceptions of discrimination influence an individual's behavior and feelings about receiving care. The attitude-related subscale assesses fears, concerns, and preferences regarding care. Finally, the instrumental subscale assesses components of care (i.e., financial considerations) that impact whether an individual can and is comfortable accessing services. The BACE was used to assess barriers at each follow-up, with participants completing the survey 3–5 times depending on the time of recruitment.
Participant responses over the entire study period were averaged to create a mean score for each item as well as for the subscales and total scale score. To examine the proportion of participants facing each barrier, binary measures were created. To capture the most common barriers experienced by participants, we examined the proportion of participants in each group reporting an average score of 1 or more for each individual barrier. To investigate the number of high-level barriers, we examined the number of barrier items participants scored at an average of 2 or greater.
Statistical analysis
Differences in sociodemographic characteristics, depression symptom onset (pregnancy vs. postpartum), depression severity, and comorbid psychiatric symptoms (measured by positive screen on Generalized Anxiety Disorder-7 [GAD-7] for anxiety, or Post-traumatic Stress Disorder Checklist-Civilian Version [PCL-C] for Post-traumatic Stress Disorder [PTSD]), were compared between individuals with and without psychiatric history. Comparisons were made using chi-square and t-tests for categorical and continuous variables, respectively. Rates of care access were compared between groups with and without psychiatric history at each step in the care pathway (screening, referral, and attendance), with chi-square tests. Logistic regression was used to model the effect of psychiatric history on access to perinatal depression care, examining odds of attending therapy, taking psychiatric medication, or receiving any care (either therapy or medication, or both). These models controlled for age, race, ethnicity, income, number of prior pregnancies and psychiatric medication use before pregnancy as a priori confounders, as well as for the clustering of individuals within obstetric practices.
Progressive model building was then carried out, adding each additional covariate one at a time, and examining the change in odds ratio (OR). None of the additional covariates met the predetermined cutoff for inclusion of at least 10% change in OR 21 ; thus, no additional variables were included in the model. We considered depression severity and comorbid psychiatric symptoms as potential mediating variables and thus did not adjust for them in the model. However, we performed a sensitivity analysis to assess the degree to which these covariates contributed to the relationship between psychiatric history and perinatal depression care access.
To examine the role of depression symptom severity on access to care, we compared results from our primary adjusted model to a model in which we accounted for depression severity. To evaluate the role of comorbid psychiatric symptoms, we similarly compared our primary model, with one in which we adjusted for the presence of comorbid psychiatric symptoms. These comparisons were used to informally assess the magnitude of potential mediation or confounding of the effect of psychiatric history on care access by these factors.
Barriers to care were assessed using participant mean scores over the study period, and barriers were ranked by percentage of participants who reported each, indicated by an average score of >1. Barrier subscale scores were similarly evaluated by the percentage of participants reporting a score >1. Finally, the average number of high-level barriers, indicated by an average score of 2 or greater, was calculated and compared across groups. All analyses were conducted using Stata 17 and SAS version 9.4.
Results
Study population characteristics
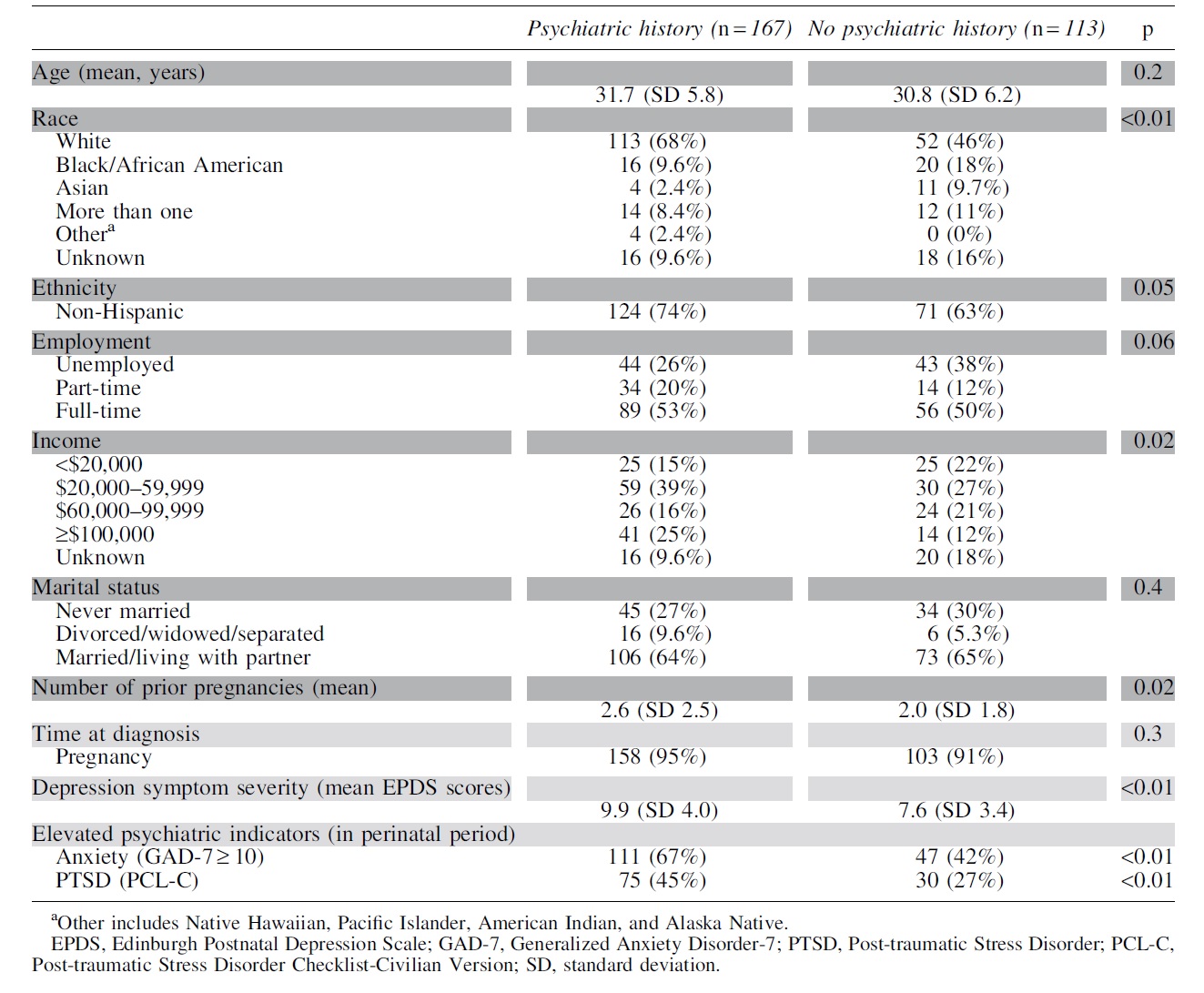
The study sample consisted of 280 perinatal individuals with depression symptoms at enrollment, of which 60% had a history of psychiatric illness before pregnancy (Table 1). Of those with a history of psychiatric illness before pregnancy, more than half reported a prior diagnosis of depression, anxiety, or both (Table 2). Participants with a psychiatric history, as compared with those without, were significantly more likely to be White and had a slightly greater number of prior pregnancies. They also had more severe depression symptoms, as indicated by higher EPDS scores, and had a higher proportion of positive screens for generalized anxiety disorder and PTSD (Table 1).
Study Population Characteristics (Dark Gray) and Psychiatric History Effect Modifiers (Light Gray)
Prepregnancy Psychiatric Diagnoses Among Participants with Psychiatric History
Percentages do not total 100% as participants were able to indicate more than one diagnosis.
Other category includes panic disorder, obsessive compulsive disorder, anorexia, bulimia, attention deficit hyperactivity disorder, psychotic disorders, and substance use disorders.
Access of perinatal depression care
Perinatal individuals with a psychiatric history versus those without differed in their experiences along the depression care pathway. Individuals without a prior psychiatric diagnosis were less likely to be screened for perinatal depression during obstetric care (88% vs. 96%, p < 0.01). They were also much less likely to be offered referral to therapy for perinatal depression (34% vs. 60%, p < 0.01), although if offered a referral they were equally likely to accept (41% vs. 57%, p = 0.1) and attend therapy (54% vs. 51%, p = 0.8; Fig. 1). Of all participants who completed the survey of care access, only 20% reported having attended therapy.
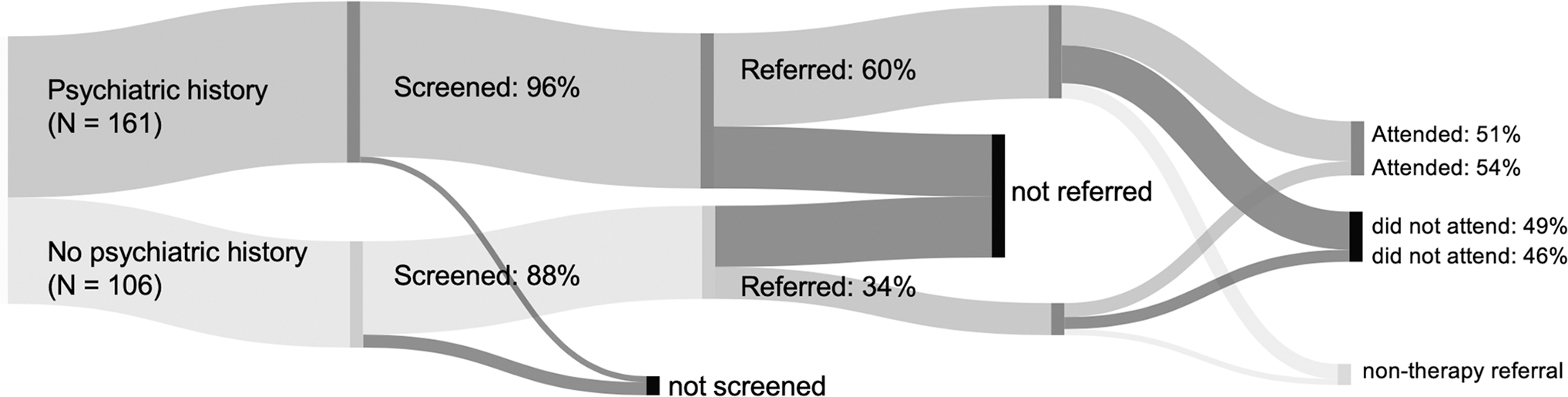
Sankey diagram of the perinatal depression care pathway as experienced by those with versus without psychiatric history. Pathway includes screening, referral to psychotherapy, and attendance of psychotherapy. Differences were statistically significant in rates of screening and therapy referral; there was no significant difference in therapy attendance.
When examining how differences in each step of the care pathway affected the ultimate receipt of care, we found that after controlling for demographic differences, perinatal individuals without a psychiatric history had 46% lower odds of attending therapy for perinatal depression, although this was not significant (OR = 0.54, 95% confidence interval [CI]: 0.19–1.55, p = 0.22) (Supplementary Tables S3 and S4). After controlling for demographic factors, as well as for depression medication use before pregnancy, individuals without a psychiatric history had 79% lower odds of taking prescription medication for perinatal depression (OR = 0.21, 95% CI: 0.08–0.54, p = 0.005) (Supplementary Tables S1 and S2). Overall, those with no psychiatric history had 80% lower odds of receiving any perinatal depression care (OR = 0.20, 95% CI: 0.08–0.47, p = 0.002) (Table 3; Supplementary Tables S5 and S6).
Odds of Receiving Perinatal Depression Care (Prescription Medication, Psychotherapy, or Either/Both [i.e., Any Care]) for Those Without Psychiatric History as Compared with Those with Psychiatric History
Adjusted model includes age, race, ethnicity, income, number of prior pregnancies, and prescription depression medication use before pregnancy.
CI, confidence interval.
Sensitivity analyses
A history of psychiatric illness was associated with higher EPDS scores and a greater likelihood of a positive screen on GAD-7 and PCL-C. Sensitivity analysis demonstrated that the severity of psychiatric symptoms (mean EPDS) partially explained the relationship between psychiatric history and care access. On average, the presence of psychiatric history was associated with an increase in both the severity of depression symptoms and the likelihood of care access. However, even when accounting for depression severity with sensitivity analysis, the presence of a psychiatric history continued to predict greater likelihood of care access for perinatal depression. Similarly, sensitivity analysis examining the impact of comorbid psychiatric symptoms demonstrated that a positive PCL-C or GAD-7 screen partially explained the relationship between psychiatric history leading to greater care access. However even when removing the effect of this potential mediator, the presence of psychiatric history continued to predict a greater likelihood of accessing perinatal depression care.
Barriers to perinatal depression care
Perinatal individuals with and without psychiatric history reported similar difficulties in accessing perinatal depression care, with average BACE scores of 17 of 90 in both groups. Participants reported an average of approximately three barriers as preventing them from receiving care “a lot” or “quite a lot.” Examining barrier subscales, the most reported barriers were attitude-related barriers, followed by stigma-related barriers, and finally instrumental barriers. Perinatal individuals with and without psychiatric history reported similar degrees of each of the three barrier types. Attitude-related barriers predominated in both groups, with ∼70% of participants reporting the desire to “solve the problem on [their] own” as a substantial barrier to accessing care. Although the proportion of individuals endorsing each barrier was similar between groups for most barriers, there were notable exceptions in the case of “concerns about treatments available” and “thinking the problem would get better by itself,” which were significantly more prevalent in those without a psychiatric history (Fig. 2).
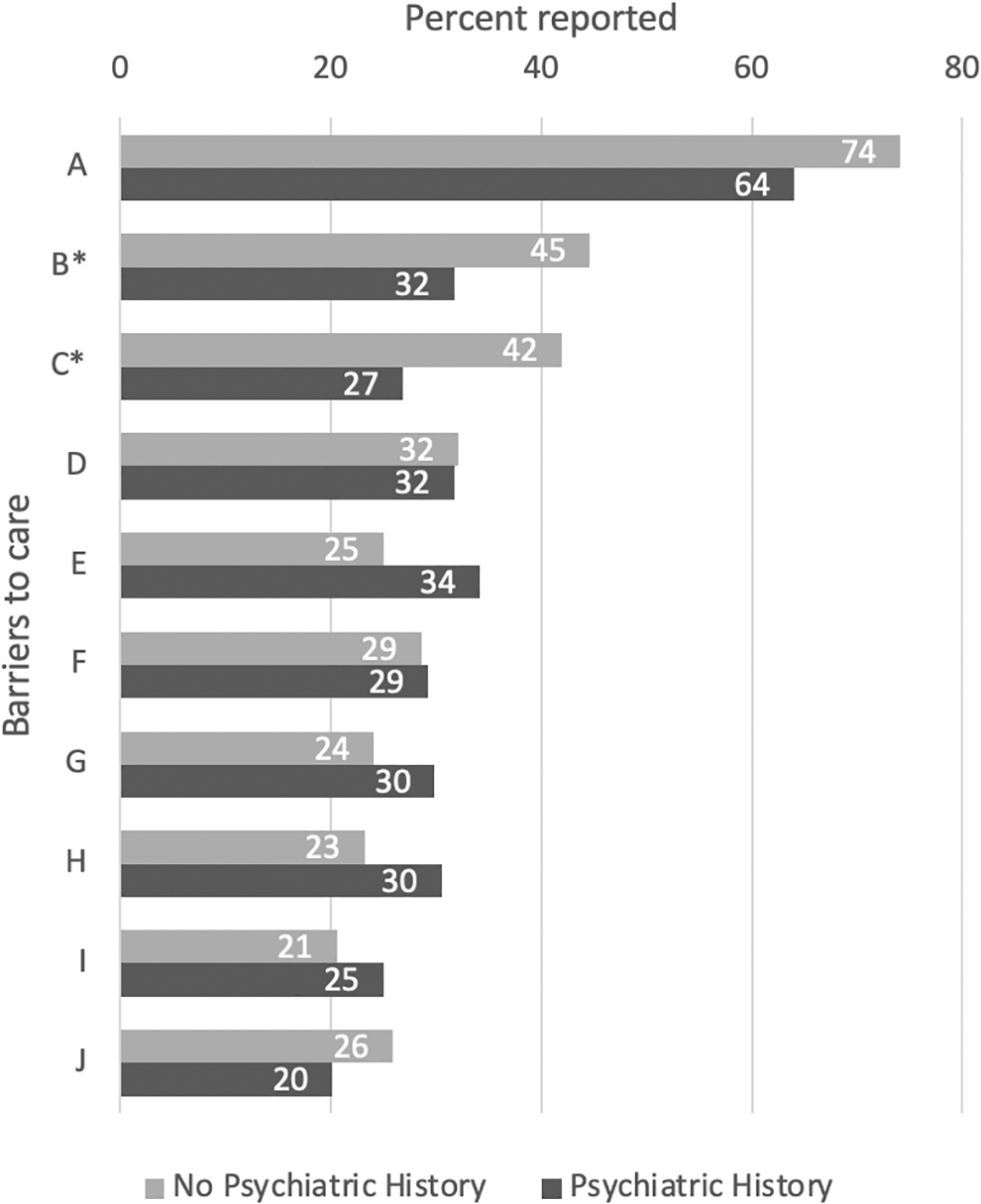
Percent of perinatal individuals with versus without psychiatric history reporting each of the top 10 most reported barriers to perinatal depression care. *Statistically significant difference in rates between groups.
Discussion
Our study compared experiences in accessing and receiving care for perinatal depression between those with and without a prepregnancy psychiatric history. We found that participants without a psychiatric diagnosis before pregnancy were less likely to access perinatal depression care, with lower rates of referral to psychotherapy and lower rates of medication access. Attitude-related barriers, as compared with stigma or instrumental, were most reported in both groups. Individuals without a psychiatric history were more likely to report attitudinal concerns about available treatments and the belief that perinatal depression would resolve on its own.
It is important to note a few key demographic differences between those with versus without psychiatric diagnoses before pregnancy. Given that social determinants of health impact both the development of psychiatric illness 22 and access to psychiatric assessment and treatment, 23,24 some demographic differences were expected. Study participants differed in both income level and number of prior pregnancies; however, the most significant difference between the groups was race. Black participants were less likely to have a psychiatric diagnosis before pregnancy compared with White participants.
Although not the primary aim of this study, investigating racial disparities is important to understanding gaps in perinatal depression care. Racial inequities in mental health care in the United States result in underdiagnosis, misdiagnosis, and undertreatment of Black individuals suffering from psychiatric illness. 25,26 It is therefore unclear if Black participants in this study had lower rates of prepregnancy psychiatric illness or if they were less likely to have their illness detected and diagnosed. 25,27 The role of race in access to psychiatric care before, during, and after pregnancy will be critical to understand in future studies, especially given that maternal morbidity and mortality disproportionately impacts Black Americans, 28 and mental health conditions are a leading cause of pregnancy-related deaths. 29
A comparison of psychiatric symptoms between groups revealed some key differences. Perinatal individuals with a prior psychiatric diagnosis had higher average EPDS scores, indicating potentially more severe depression, and were more likely to screen positive for anxiety or PTSD. These differences were expected, as individuals with a psychiatric history are at greater risk for severe perinatal depression and many individuals had prior diagnoses of, and potentially comorbid, anxiety or PTSD. These findings are consistent with the understanding that higher depression severity and greater comorbid psychiatric illness burden may be part of the mechanism through which prior psychiatric history impacts perinatal depression care. 30
Access of perinatal depression care
Perinatal individuals without a psychiatric history were less likely to access care at multiple points along the perinatal depression care pathway. Although PRISM study recruitment included mental health screening, study participants were also asked whether they were screened for perinatal depression at their obstetric practice. The answers to these questions revealed that universal screening has not yet been attained and that there are screening differences by psychiatric history. 12 Those without a psychiatric history were less likely to be screened for perinatal depression during obstetric care. Although current ACOG recommendations are for universal screening for depression in the perinatal period, 9 providers may be more diligent in screening those with a psychiatric history, as they have a known risk factor. However, the physiologic and psychosocial changes of pregnancy and postpartum increase the risk of depression for all perinatal individuals, 15,31 necessitating universal screening.
Those without prior psychiatric history were also less likely to be referred to therapy. This could be related to lower provider concern given lower symptom severity; however, sensitivity analysis accounting for EPDS scores showed that depression severity accounted for only a small part of the between-group difference. Of importance, in the setting of perinatal depression, in which early initiation of treatment is recommended, 32 the tradeoff between sensitivity and specificity may favor the use of a lower screening score (10 as opposed to 13). USPSTF guidelines note that therapy is effective in preventing perinatal depression and recommend that all perinatal individuals at elevated risk of depression receive therapy. All patients with a psychiatric history or with depressive symptoms, including those with elevated but subthreshold scores on screening, are considered higher risk and should be referred for preventative therapy. 9,32
In examining the receipt of pharmacotherapy for perinatal depression, we found that even when controlling for baseline use of medication, those without psychiatric history were much less likely to be prescribed medication for perinatal depression compared with those with a psychiatric history. One mediator of this difference was depression symptom severity; however, sensitivity analysis demonstrated that this accounted for only a small part of the difference in access to prescription medications. There is no current consensus on the impact of symptom severity on access to care for depression. Some studies have shown facilitating effects, whereas others have shown that more severe symptoms are a barrier to care. 33 Those with a history of psychiatric illness are at higher risk of experiencing severe depression symptoms and comorbid psychiatric symptoms, as compared with those without a psychiatric history. 30
These two factors may be part of the mechanism by which a history of psychiatric illness affects perinatal depression care. For example, providers may be more likely to recommend medications for those with a prior psychiatric history, especially for individuals who report that medication treatment has been effective. It is also possible that patients without a prior psychiatric history may be less familiar with treatments or more hesitant to try medication treatment. This is supported by our finding that those without a psychiatric history were more likely to report “concerns about treatments available” as a barrier to accessing care. However, our data do not elucidate whether the differences in medication and therapy access were because of patient versus provider factors. This must be explored in future studies.
Many perinatal individuals prefer psychotherapy over pharmacotherapy owing to concern about the effects of medications on the fetus in pregnancy or infant via lactation. 34 However, 2%–7% of individuals take antidepressants in the perinatal period, 35 and selective seretonin reuptake inhibitor have a relatively strong safety profile and are among the more studied classes of medications in pregnancy. 35 –37 Our results (1) emphasize the importance of framing discussions in terms of the risk of treated versus untreated disease, and (2) reinforce the need for thorough counseling and shared decision making to ensure all perinatal individuals have access to the full range of therapeutic options. 38
Barriers to perinatal depression care
Given the high and increasing incidence of psychiatric illness in individuals of childbearing age, understanding how the presence of this history impacts how individuals receive care is crucial. Given that all participants reported barriers to depression care, increased attention to addressing barriers as part of regular obstetric practice is needed. The general trends in the presence barriers were similar across groups, with two notable exceptions: we observed important differences in prevalence of (1) concerns about available treatments, and (2) belief that the problem would get better on its own. Both barriers were highly prevalent in those without a psychiatric history (the second and third most reported barriers in this group) and less common in those with a prior psychiatric diagnosis.
These specific differences highlight the impact of experience with psychiatric illness on accessing mental health care; they suggest that prior experience can increase comfort with psychiatric care and improve understanding of the need for treatment of psychiatric illness. This is consistent with studies demonstrating that prior psychiatric care access predicts perinatal depression care access 39 and reinforces the importance of psychoeducation as part of routine perinatal visits.
Attitude-related barriers were the most reported, with “wanting to solve the problem on my own” as the most prevalent barrier to accessing care. It is important to recognize how common these attitudes are, as this is a place where psychoeducation may be helpful. 40 Encouragement from obstetric providers to engage in treatment, explanation that symptoms of depression are not a normal part of pregnancy and postpartum, and education around the potential negative impacts on both mother's and child's health, may help increase uptake of psychiatric resources. 41 Attitudes about self-reliance are recognized as prominent barriers for psychiatric illness help-seeking 42 and more research is needed to determine effective strategies to address these barriers in the clinical setting.
Stigma was also a barrier to perinatal depression care, with the most common barrier reported being “concern that I might be seen as a bad parent.” This is in line with the qualitative literature on barriers to help-seeking for perinatal depression, which shows fears around stigma related to psychiatric illness and parenting. 14 Provider acknowledgement and reassurance around these fears could be a powerful method to addressing this barrier, although continued societal efforts to de-stigmatize mental illness remain important.
Although several prior studies have described instrumental factors as leading barriers to the receipt of perinatal depression care, in our study instrumental barriers were the least cited. Of importance, this study was conducted with individuals receiving perinatal care in obstetric practices involved in interventions specifically aimed at connecting perinatal individuals to care. 17,43,44 Instrumental barriers being minimally cited potentially reflects the effectiveness of the primary study intervention in achieving its goal.
It is important to note that instrumental barriers also vary along with social drivers of health, and with government and social resources that change by state. Understanding how these social determinants interact with barriers will be crucial in future work to determine how best to improve care access in all perinatal individuals. Critically, there was one instrumental barrier that remained highly prevalent, which was childcare difficulties. Lack of childcare has been frequently noted as a barrier to receiving perinatal depression care; 14 this was reaffirmed in this study. Increasing psychiatric care flexibility, such as by maintaining and expanding the use of telehealth, and improving access to affordable childcare, could help address this persistent barrier. 45,46
Study strengths and limitations
This study was strengthened by its unique combination of data including both depression screening, and assessments of care access and barriers to care access. It is unique in examining the relationship between psychiatric history and access and barriers to care. Our study population was diverse and demographically representative of perinatal individuals in the state of Massachusetts. 47,48 Even with these strengths, some aspects of the PRISM data set limited our analysis. Our study was limited in its investigation of treatment acceptance, which would benefit from future research expanding on our results. In addition, the exposure to the MCPAP for Moms and PRISM programs may have decreased instrumental barriers and may limit the generalizability. Finally, although our study observed differences in prepregnancy psychiatric diagnoses by race, we were not able to explore the causes of these differences or how they may be addressed. Further work is needed to understand and address perinatal depression in marginalized populations.
Conclusions
Perinatal depression should be a primary concern of those caring for perinatal individuals because it is a preventable cause of maternal morbidity and mortality. 8 Despite increasing awareness of its prevalence, it remains underdiagnosed and undertreated, 11 resulting in needless suffering of perinatal individuals and their families. This study demonstrates the importance of an individual's psychiatric history or lack thereof, in understanding their ability to access steps along the depression care pathway. Those without a psychiatric history before pregnancy are less likely to access care for perinatal depression. They are less likely to be screened, offered referral, or be prescribed pharmacotherapy.
These results underline the need for all obstetric providers to universally screen for depression in pregnancy and postpartum, as recommended by ACOG and the USPSTF. 9,32 Our results also shed light on the importance of shared and informed decision-making regarding perinatal psychopharmacotherapy. Perinatal individuals without a psychiatric history are also more likely to believe depression symptoms will self-resolve and have fears about available therapies. These findings strongly support the need for psychoeducation regarding perinatal depression, especially for those without experience with the psychiatric care system. Our results suggest that greater focus on patient education, universal screening, and a low threshold for referral to therapy would improve access to depression care for perinatal individuals.
Footnotes
Acknowledgments
The authors sincerely thank the obstetric practices and the perinatal individuals that participated in the PRISM study, as well as the MCPAP for Moms and PRISM study teams. The authors thank Linda Brenckle for her leadership on the PRISM study and guidance in navigating the PRISM data set and Martha Zimmermann for feedback on this article.
Authors' Contributions
E.M. conceived of the presented analysis and completed the initial draft of the article. A.P.N. supervised the development of the methods. J.F. completed the majority of the statistical analyses. T.A.M.S. and N.B. supervised the project. All authors critically reviewed and edited each draft for important intellectual content and provided approval for publication and agree to be accountable for all aspects of the work.
Author Disclosure Statement
T.A.M.S. is lead obstetric engagement liaison as a consultant for the MCPAP for Moms and as such has received a stipend from the Massachusetts Department of Mental Health via Beacon Health Options. T.A.M.S. is medical director of Lifeline for Moms at UMass Chan Medical School and Multiple Principle Investigator (MPI) of the Lifeline for Moms National Network of Perinatal Psychiatry Access Programs which is supported by the Perigee fund. In addition, she is co-PI, MPI or co-investigator (co-I) on other federally funded grants focused on intervention or resource development and evaluation related to perinatal mental health. T.A.M.S. is co-chair of the ACOG's Maternal Mental Health Expert Work Group, a member of ACOG's Clinical Practice Guidelines—Obstetrics Committee, a member of the Alliance on Innovation in Maternal Health's (AIM) perinatal mental health conditions patient safety bundle development work group and lead faculty for the Institute of Healthcare Innovation's (IHI) associated change package work group.
N.B. has received salary and/or funding support from Massachusetts Department of Mental Health via the MCPAP for Moms. She is also the Medical Director of Research and Evaluation for MCPAP for Moms and the Executive Director of the Lifeline for Families Center and Lifeline for Moms Program at UMass Chan Medical School. She is the Corresponding Principal Investigator (PI) of the Lifeline for Moms National Network of Perinatal Psychiatry Access Programs, and PI, MPI, or co-I on several extramurally funded grants focused on intervention or resource development and evaluation related to perinatal mental health. She has received honoraria from Global Learning Collaborative. She has also served as a consultant for The Kinetix Group, VentureWell, and JBS International. All other authors have no conflicts of interest to disclose.
Funding Information
This research was supported by the University of Massachusetts Chan Medical School Center for Clinical and Translational Science. The PRISM study was primarily supported by the Centers for Disease Control and Prevention (CDC) through a Cooperative Agreement (Grant No. 1U01DP006093) awarded to the University of Massachusetts Chan Medical School.
Supplementary Material
Supplementary Figure S1
Supplementary Table S1
Supplementary Table S2
Supplementary Table S3
Supplementary Table S4
Supplementary Table S5
Supplementary Table S6
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.