
Abstract
Background:
Second-generation antipsychotics (SGAs), also called atypical antipsychotics, are common therapies for women with a spectrum of psychiatric disorders. No systematically ascertained human reproductive safety data are available for lurasidone, and prospective data for quetiapine are limited, making decisions regarding use of these medications during pregnancy complicated.
Materials and Methods:
The National Pregnancy Registry for Psychiatric Medications is a prospective cohort study designed to collect reproductive safety data relative to SGAs. Pregnant women aged 18–45 years, with psychiatric illness and prenatal psychotropic medication exposure completed three phone interviews during pregnancy and the postpartum period. Cases of presumed malformations are abstracted from medical records for adjudication by a teratologist blinded to medication exposure.
Results:
Of 2,293 women enrolled at the time of analysis, 134 in the lurasidone group, 264 in the quetiapine group, and 886 controls completed the postpartum interview and were therefore eligible for inclusion. Dropped or lost-to-follow-up participants (13%) and those currently pregnant were excluded. Participants were predominantly White, college-educated, and married (lurasidone = 88.1%, 76.9%, 77.6%; quetiapine = 89.8%, 71.2%, 75.0%; controls = 92.7%, 86.7%, 89.1%). Absolute risks of major malformations were 2.19% (lurasidone), 1.85% (quetiapine), and 1.77% (controls). Odds ratios comparing lurasidone and quetiapine with controls were 1.24 (95% confidence interval [CI] = 0.36–4.32) and 1.04 (95% CI = 0.38–2.85), respectively.
Conclusions:
No specific patterns of malformations were observed in infants exposed to the medications of interest. Lurasidone and quetiapine did not appear to be major teratogens, but further information is needed to refine risk estimates. Food and Drug Administration guidance underscores the importance of pregnancy registries.
Clinical trial number: NCT01246765.
Introduction
Second-generation antipsychotics (SGAs), also called atypical antipsychotics, are increasingly used as primary or adjunctive therapy by reproductive-age women across a spectrum of psychiatric disorders including bipolar disorder, schizophrenia, unipolar depression, and anxiety disorders. 1,2 Despite increasing frequency of use for on- and off-label indications, 3 current approval standards do not require new medications to be studied for human reproductive safety before entering the market, 4 resulting in sparse data across few prospective studies. 5,6 The 2015 U.S. Federal Drug Administration's Pregnancy and Lactation Labeling Rule (PLLR) emphasizes the importance of pregnancy registries for postmarketing analysis and requires delineation of descriptive pregnancy and lactation risk data in medication label sections 8.1–8.3, replacing the prior A, B, C, D, and X teratogenicity category system, which was widely criticized for its imprecision, deficit of clinical information, misinterpretation as a grading system, and inconsistency with international labeling systems. 7 –9
Current SGA safety information listed in accordance with the PLLR is limited or absent for individual medications within the class, and SGA class information is derived from disparate methodologies including case studies, retrospective cohort studies, manufacturer reports, and a small number of prospective cohort studies. 10 –19 These study designs have varying drawbacks that complicate data interpretation and clinical decision-making surrounding maternal benefits versus fetal exposure risks and that include use of control subjects without psychiatric illnesses, absence of a comparison group, and/or lack of adjustment for confounders including psychiatric indication. 20
Two especially important SGA medications for which to delineate risk are quetiapine, the most commonly prescribed SGA among pregnant women, 21 and lurasidone, a newer SGA for which no human reproductive safety data exist. Although lurasidone has shown no evidence of teratogenicity in animal studies, 22 release of preliminary human data is urgent for providers, as lurasidone use during pregnancy is anticipated to increase owing to recent Food and Drug Administration (FDA) generic approval and addition of indications for bipolar depression monotherapy and lithium or valproate adjunctive therapy. Regarding quetiapine use during pregnancy, prospective cohort studies by Habermann et al., 10 Kulkarni et al., 23 and Sadowski et al. 12 note no significant difference in absolute risk for major malformations compared with controls but do not preclude moderate risk increases, necessitating further study of this widely used medication.
To address the need for robust reproductive pharmacovigilance data, the National Pregnancy Registry for Psychiatric Medications (NPRPM) was established at Massachusetts General Hospital (MGH) in 2008. Modeled after the North American Antiepileptic Drug Registry, the NPRPM captures risk of major malformations following first-trimester exposure to SGAs as a primary outcome. Secondary outcomes include obstetrical, neonatal, and neurobehavioral sequelae. 24
NPRPM results regarding risk of SGAs as a class were reported in 201525 and updated in 2021, 26 suggesting that SGAs are not associated with major teratogenic risk. The Harvard Program on Perinatal and Pediatric Pharmacoepidemiology recently reported on the use of SGAs among publicly insured pregnant women and found no increased risk of major malformations after adjusting for confounders. 27 Despite these encouraging findings, current estimates have not ruled out a modest teratogenic risk, and little prospective data exist for individual SGAs. Preliminary quetiapine risk data were previously released from the NPRPM in 2018 and found no significant increase in major malformation risk associated with its use, but enrollment numbers have greatly increased, allowing for a more precise risk estimate. 28 The current report includes the first release of lurasidone reproductive safety data from the NPRPM and an updated risk estimate for quetiapine exposure.
Materials and Methods
The NPRPM is a prospective cohort study for which detailed methods were previously reported. 24 In brief, pregnant women aged 18–45 years with lifetime histories of psychiatric illness were followed during pregnancy and postpartum to determine risk of major malformations in infants with first trimester in utero exposure to SGAs including aripiprazole, aripiprazole lauroxil, asenapine, brexpiprazole, cariprazine, clozapine, iloperidone, lurasidone, olanzapine, paliperidone, paliperidone palmitate, quetiapine, risperidone, and ziprasidone. Any new SGA medications approved by the FDA were also studied.
Lifetime history of psychiatric illness is defined as diagnosis of a psychiatric illness at any time before enrollment in the study. To capture this history, a semistructured interview, modeled off the Mini International Neuropsychiatric Interview, 29 was conducted. A timeline of symptom onset, diagnoses, and treatment was also collected for each self-reported psychiatric illness. The exposure group included women with first trimester use of any SGA, whereas women in the comparison group remained unexposed to these agents during pregnancy. All participants provided verbal informed consent, and study procedures were approved by the MGH Institutional Review Board.
Participants were interviewed by trained research staff via phone at three points across pregnancy: enrollment (any time during pregnancy), 7 months gestation, and 3 months postpartum. The enrollment interview collected information regarding demographics; pharmacotherapy before, during, and after pregnancy; psychiatric and medical history; family history of birth defects; teratogen exposure; and social factors including drug and alcohol use. The 7-month interview updated these data and noted prenatal complications. The postpartum interview gathered third-trimester updates, medication changes, labor and delivery information, and neonatal outcomes. Maternal report was confirmed to 6 months postpartum using a rigorous maternal and pediatric medical record review process by study staff and a senior physician investigator. Medical records identifying potential major malformations were redacted and sent to a dysmorphologist blinded to medication exposure and psychiatric indication for adjudication.
The primary outcome variable was risk of major malformation, defined as a structural abnormality with surgical, medical, cosmetic, or clinical importance identified within 6 months of birth. 24,30,31 Minor abnormalities, deformations, birthmarks, genetic disorders, chromosomal abnormalities, physiological features owing to prematurity, and any findings by prenatal sonography or at surgery or autopsy not identified by an examining pediatrician were excluded.
Release of findings and other major policy decisions were determined by a Scientific Advisory Board comprising experts in psychiatry, teratology, epidemiology, pediatrics, and pharmacology. The NPRPM is financially supported by pharmaceutical manufacturers who agree to fund reproductive safety research. A listing of past and current sponsors
32
is included at
Statistical analyses
The primary exposures evaluated were use of lurasidone or quetiapine during the first trimester of pregnancy (0 ≤ 13 weeks). Each medication was considered separately. Exposure to each medication was operationalized as a binary variable: use of the selected SGA during first trimester (exposed) or no use of any SGA for the entire pregnancy (unexposed). Women who used an SGA during only the second and/or third trimester were excluded.
Discrete and continuous potential confounders and demographics provided by maternal report are given in Table 1 for quetiapine and lurasidone. All potential confounders were measured at enrollment before or concurrently with SGA exposure and before the primary outcome occurred.
Characteristics of Study Population
n, number of women for which these data were available. Lower numbers most often reflect questions that were added to NPRPM interviews as updates to the protocol and may exclude women who participated before these additions.
N = 262 owing to missing data.
For history of postpartum depression or psychosis, participants were included in the valid n only if they reported a prior pregnancy.
Chronicity was calculated as the difference between baseline age and age at psychiatric symptom onset, divided by baseline age.
NPRPM, National Pregnancy Registry for Psychiatric Medications; SNRI, serotonin–norepinephrine reuptake inhibitor; SSRI, selective serotonin reuptake inhibitor.
The unadjusted odds ratios of a major malformation were compared among infants exposed to each medication and infants unexposed to SGAs and were considered the primary outcome. As a sensitivity analysis, the effects of possible confounding by individual factors listed in Table 1 on the odds ratio and possible direction of bias were examined as given in Figure 2, by applying an analytic model used in previous NPRPM analyses and elsewhere 28,33,34 in which variables were added individually to the crude logistic regression model that had computed the unadjusted exposure odds ratio to examine the change in odds ratio for major malformations.
Analyses were completed using SAS, version 9.4 (SAS Institute, Cary, NC, USA).
Results
From November 2008 to April 1, 2021, 2,293 women were enrolled. Based on completion of the postpartum interview at the time of data extraction, 264 women with exposure to quetiapine, 134 with exposure to lurasidone, and 886 with no SGA exposure were eligible and evaluable for these analyses. Ineligible participants included those who had not completed postpartum interviews, those who dropped from the study or were lost to follow-up, those who had a spontaneous or therapeutic abortion not owing to a known major malformation, and those who were exposed to an SGA medication during only the second and/or third trimester (Fig. 1). The rate of medical record procurement was 76%. Twenty-eight women had twin pregnancies, and 1 woman had a triplet pregnancy.
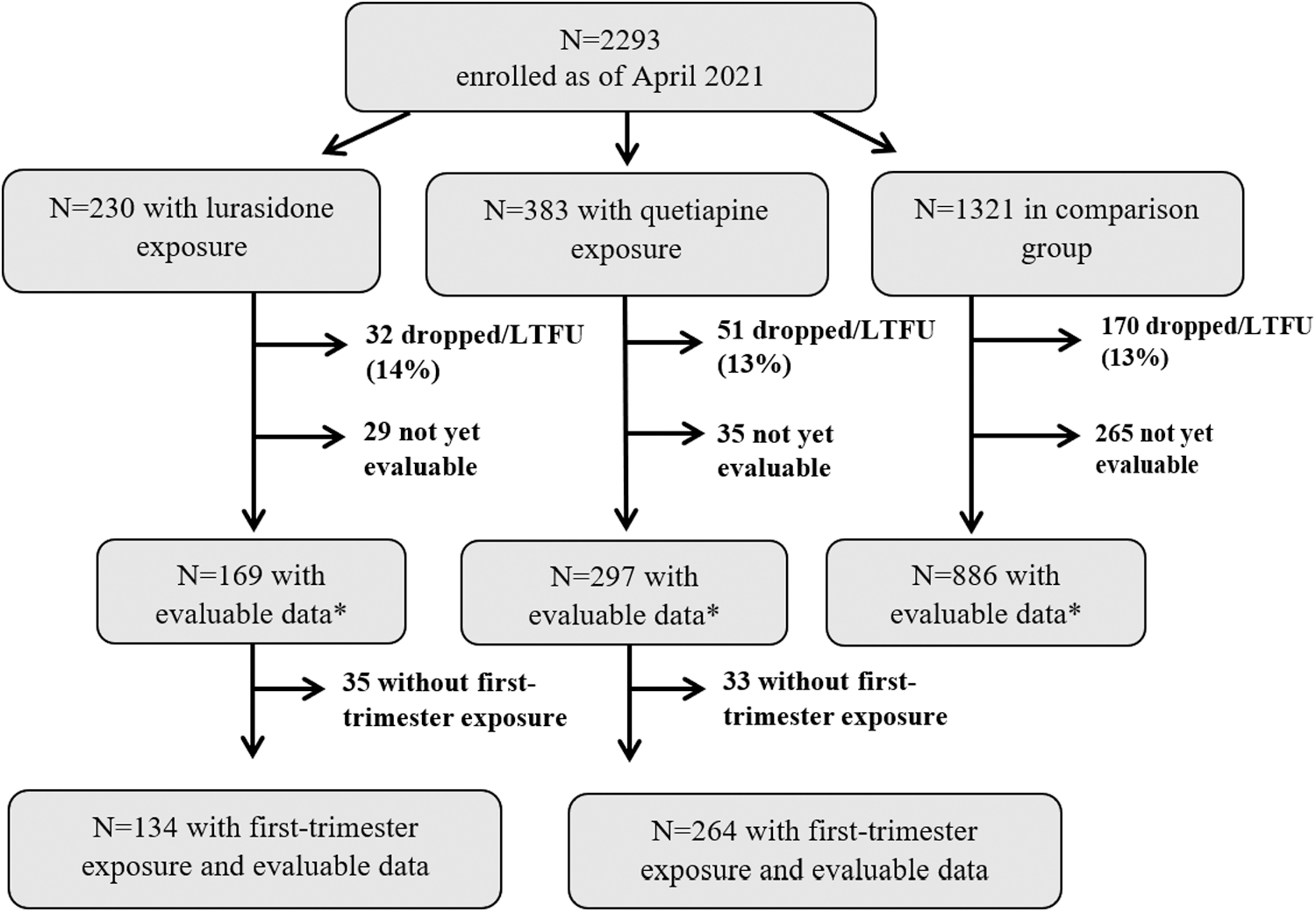
Selection of analytical sample. Study population cohort diagram indicating analytical sample from enrolled population. *Evaluable data include subjects for which a postpartum interview has been completed. Medical records have been obtained for 76% of participants. Major malformations are confirmed with medical records. LTFU, lost to follow-up.
Table 1 provides cohort characteristics including demographics, clinical information, psychotropic medication use during pregnancy, and other exposures (alcohol, illicit/recreational drugs, cigarettes, prenatal vitamins) for both exposure and comparison groups.
There were a number of differences between participants in the exposed and unexposed groups. Women in the quetiapine and lurasidone exposure groups were less likely to be college-educated than controls (71.2% and 76.9% vs. 86.7%), less likely to be married (75.0% and 77.6% vs. 89.1%), less likely to have planned pregnancies (73.5% and 76.1% vs. 82.2%), and more likely to be multigravida (37.5% and 38.1% vs. 29.3%). First trimester alcohol use was more prevalent in controls (31.5%), compared with quetiapine (22.3%) and lurasidone (21.6%). Cigarette use was more prevalent in exposure groups (quetiapine = 19.7% and lurasidone = 14.2% vs. controls = 5.5%).
There were also notable differences in psychiatric history and psychotropic medication exposure. The quetiapine and lurasidone groups were more likely to have primary psychiatric diagnoses of bipolar disorder (63.3% and 75.4% vs. 9.9%) and less likely to have primary diagnoses of depression (12.1% and 6.7% vs. 33.3%) or anxiety (7.6% and 3.0% vs. 31.4%) than controls. Control participants were more likely to use selective serotonin reuptake inhibitors (56.1% vs. quetiapine = 31.1% and lurasidone = 21.6%) and less likely to use lithium (2.4% vs. quetiapine = 7.6% and lurasidone = 7.5%). The class of medication most frequently used concomitantly with SGAs was anticonvulsants (quetiapine = 34.8%; lurasidone = 33.6%).
Of the infants born to participants, 273 were in the quetiapine-exposed group, 137 were in the lurasidone-exposed group, and 904 were in the comparison group. The absolute risks of major malformations in the exposure groups were 1.83% (95% confidence interval [CI] = 0.60–4.22; 5 malformations) for quetiapine and 2.19% (95% CI = 0.45–6.27; 3 malformations) for lurasidone, as compared with 1.77% (95% CI = 1.01–2.86; 16 malformations) in the unexposed group (Table 2). General population malformation risk data from the U.S. Centers for Disease Control and Prevention (CDC) and Brigham and Women's Hospital Active Malformations Surveillance Program (BWH-AMSP) and data from the NPRPM examining risk of exposure to aripiprazole or SGAs as a class are given in Table 2 for clinical context. 26,30,31 The unadjusted odds ratio of a malformation owing to quetiapine exposure compared with controls was 1.04 (95% CI = 0.38–2.85), and that owing to lurasidone exposure compared with controls was 1.24 (95% CI = 0.36–4.32) (Table 2).
Major Malformation Absolute Risks and Odds Ratios in Infants Across Exposure Groups
Absolute risks and odds ratios of a major malformation for infants exposed to quetiapine or lurasidone compared with unexposed controls, with important clinical reference values. Risk information is provided for aripiprazole, SGA medications as a class, and baseline malformation rates from the general population as references for clinical comparison and were not included in present analyses.
Adjusted data provided for reference from recent publications. Because analyses were carried out separately from those presented here, the control group n for these publications is different than the reference shown above the double line. 26,33
CDC Metropolitan Atlanta Congenital Defects Program measures rates of major malformations in all infants born to women in the general population of the United States. 30
Brigham and Women's Hospital Active Malformations Surveillance Program examined the rates of malformations for infants born at Brigham and Women's Hospital in Boston, Massachusetts, from 1972 to 2012. 31
CDC, Centers for Disease Control and Prevention; SGA, second-generation antipsychotic.
None of the characteristics that differed in Table 1 between exposed and unexposed groups significantly changed the CI for the estimate of malformation risk in comparing the exposed and unexposed groups in the regression model (Fig. 2).

Sensitivity analysis adjusting malformation ORs for covariates. Sensitivity analysis adjusting malformation ORs for covariates comparing lurasidone (N = 137)
Supplementary Figure S1 provides the stabilization of risk and confidence intervals over time with increasing cohort size. Because of this stabilization, the NPRPM Scientific Advisory Board approved release of reproductive safety data for these molecules.
Details of confirmed malformations for each group are listed in Table 3. No patterns of malformations were observed in any group.
Malformations and Concomitant Medication Exposures by Group
List of major malformations confirmed by an expert teratologist in infants in exposure and control groups.
All concomitant medication exposures during pregnancy are listed to reflect polypharmacy.
PIK3CA, phosphatidylinositol-4,5-bisphosphate 3-kinase catalytic subunit alpha.
Discussion
These results represent the first human reproductive safety data for lurasidone and provide updated estimates of risk for major malformations for quetiapine, demonstrating that fetal exposure to either is not strongly associated with increased rates of major malformations. These findings are consistent with previously reported studies, 19,25,27,35 although sample size remains insufficient to preclude modest teratogenic effects for either medication. Of note, in addition to finding no increased risk of major malformations, we observed no distinct pattern of malformations in either the exposure or comparison groups, providing further reassuring evidence that these molecules are not strongly associated with specific deformities.
The findings presented here are consistent with extant literature examining risk of exposure to SGAs, which despite significant methodological heterogeneity across studies, do not show a strong association between first trimester exposure and increased rates of major malformations. Although two large epidemiologic studies reported a risk ratio 1.5–2.5-fold higher for major malformations in infants exposed to SGAs as a class compared with unexposed infants 10,23 and noted a significant increase in cardiac defects, it is notable that pregnancies of women treated with psychotropic medications are more likely to be screened for congenital cardiac defects than unexposed women and may be subject to detection bias. 36 Other studies, including a case review of over one million women enrolled in Medicaid, 27 are consistent with our findings showing low absolute and relative risks and no pattern of malformations among SGA-exposed infants. 37,38
Clinical implications of the findings from the current report are noteworthy. The data highlight the importance of considering absolute risks of major malformations in exposed versus unexposed groups. Data from the CDC and from BWH-AMSP show a major malformation prevalence of 3% and 2.43%, respectively, among all live births in the United States. 30,31 In the current analysis, the absolute risk of major malformations was lower in all three groups (quetiapine = 1.83%; lurasidone = 2.19%; unexposed = 1.77%), suggesting the low observed absolute risks might be influenced by high rates of healthy behaviors in women who elect to enroll in a pregnancy registry. Examining individual molecules within the SGA class side-by-side allows for initial impression of relative contributions of these specific medications relative to the reproductive safety of the class. Because of sample sizes, direct head-to-head comparison is still not possible.
Strengths of this study include its prospective design, selection of an appropriate comparison group of women with psychiatric disorders, methodical collection of important social, medical, psychiatric, and pregnancy-specific history using structured interviews, systematic medical record review for extraction of primary and secondary outcomes by both study staff and a senior physician investigator, and rigorous malformation adjudication process by a teratologist blinded to medication exposure and psychiatric diagnoses.
The prospective design of the NPRPM minimizes recall and selection biases, and the dual review of medical records and maternal report allows the research team to obtain in-depth contextual information regarding potential confounders (lifestyle and demographic factors, psychiatric illness burden, and detailed medication use patterns), which are not typically discernable from medical records alone. These potential confounders relate to many factors known to impact malformation risk, including pharmacotherapy, planned pregnancy status, maternal age, diagnosis and severity of illness, body mass index, first trimester environmental and teratogenic exposures, family history of birth defects, prenatal vitamin use, and social indicators including alcohol and cigarette use.
Another strength is that participants in the reference group were recruited and enrolled using the same methodology as the exposure groups. Whereas studies using large claims databases or national birth registries typically assess reproductive risk of SGAs using a control group of women from the general population, participants in the NPRPM comparison group had histories of psychiatric illness and other psychotropic medication use. These enrollment criteria mitigate confounding by several variables including psychiatric illness indication, illness severity, and associated behaviors.
Limitations of this study include the relatively small sample size of participants exposed to individual molecules and the generalizability of results. Although our sample size is among the largest of all prospective studies to date, participants in the NPRPM are disproportionately White, married, and well-educated compared to the general population of women treated with SGA medications. 39 Few women in the NPRPM have a diagnosis of schizophrenia, resulting in an underrepresentation of women with schizophrenia treated with SGAs relative to those with bipolar disorder diagnoses, who make up the majority of women in the exposure groups. Furthermore, the NPRPM analyzes risk of major malformations as a function of medication exposure rather than indication. It is possible that indication may influence outcomes, but it is reassuring that only a very small number of women in the NPRPM take SGAs for an indication other than bipolar disorder, and major depressive disorder minimizing any potentially confounding effects owing to variation in indication of SGA users with nonmood disorder indications such as sleep or anxiety.
In addition, enrollment in the NPRPM is voluntary and may lead to self-selection bias, as participants who opt in may be more health conscious, higher functioning, and better informed than nonparticipants. It is unknown how significantly the population of women who enroll in pregnancy registries differ from nonenrollees, and therefore the data regarding reproductive safety may not account for unidentified confounding factors.
Another study limitation is the absence of standardized genetic testing in infants exhibiting a major malformation. Our analyses exclude cases of malformations caused by known genetic or chromosomal abnormalities (e.g., Down's syndrome), but it is possible that malformation cases included in this analysis were caused by an undiagnosed genetic disorder rather than an in utero teratogenic exposure. If such cases were indeed included in the analysis, our findings may overestimate true absolute risk.
The NPRPM's robust data collection make it a strong platform to support a variety of future analyses, including long-term neurobehavioral effects of in utero exposure to SGAs as well as various obstetrical and neonatal outcomes associated with pharmacotherapy. Given high utilization rates of quetiapine and the increasing use of lurasidone by reproductive-age women, there is a pressing need for patients and providers to have access to rigorous data about other potential risks of fetal exposure to these drugs to facilitate clinical decision-making.
As NPRPM enrollment continues, larger sample size and greater diversity of participants will increase external validity and narrow CIs around major malformation odds ratios for each medication. It must be emphasized that potential risk of malformations associated with fetal exposure to medication is only one of the many considerations used by women as they consider use of pharmacotherapy during pregnancy. Other relevant factors that are typically factored into discussions of potential use of psychotropics during pregnancy include risk of relapse with and without medication discontinuation, severity and previous course of illness for an individual patient, risk of in utero exposure to untreated psychiatric illness, treatment preferences, and other patient-specific variables. 40
Many women experience psychiatric illness while pregnant or planning pregnancy, and use of a medication such as an SGA may be the most favorable treatment plan for some patients. 40 Such results are an important basis for thoughtful risk/benefit conversations between patients and clinicians, facilitating collaborative, informed decisions about psychiatric treatment during pregnancy factoring in patients' clinical history and wishes.
Conclusions
In summary, these findings provide reassuring evidence that quetiapine and lurasidone are not major teratogens. Although major methodological differences between existing studies examining reproductive safety create barriers to comparing the risk of malformations across analyses, the cumulative evidence indicates low absolute risks of congenital deformities associated with SGA use. These data will help patients and providers as they make collaborative treatment decisions and carry important implications for maternal mental health and neonatal outcomes. Further investigation is essential to increase precision of malformation risk estimates and study additional maternal and neonatal outcomes associated with use of quetiapine and lurasidone, as well as other SGAs, during pregnancy.
Footnotes
Authors' Contributions
L.S.C.: supervision, conceptualization, funding acquisition, methodology, writing—original draft; T.R.C.: investigation, data curation, visualization, writing—original draft; M.P.F.: supervision, conceptualization, funding acquisition, methodology, writing—review and editing; P.G.: formal analysis, data curation, visualization; P.S.C.: investigation, data curation, writing—review and editing; L.A.K.: investigation, data curation, visualization, writing—review and editing; M.A.: investigation; E.T.R.: investigation, data curation, visualization, writing—review and editing; D.C.: conceptualization, methodology, investigation, writing—review and editing; S.H.-D.: conceptualization, methodology, writing—review and editing; A.C.V.: supervision, conceptualization, funding acquisition, methodology, writing—review and editing
Disclaimer
Sponsors have no role in research design, data collection, analysis, release of findings, or article preparation.
Author Disclosure Statement
T.R.C., P.G., P.S.C., L.A.K., M.A., E.T.R., and D.C. report no conflicts of interest.
Funding Information
L.S.C.—as of 9/20/2022. Research Support: Dr. L.S.C. is an employee of MGH, and works with the MGH National Pregnancy Registry. MGH National Pregnancy Registry: Current Sponsors: Alkermes, Inc. (2016–Present); Eisai, Inc. (2022–Present); Johnson & Johnson/Janssen Pharmaceuticals, Inc. (2019–Present); Otsuka America Pharmaceutical, Inc. (2008–Present); Sage Therapeutics (2019–Present); Sunovion Pharmaceuticals, Inc. (2011–Present); Supernus Pharmaceuticals (2021–Present); Teva Pharmaceutical Industries Ltd. (2018–Present). Past Sponsors: Forest/Actavis/Allergan (2016–2018, declined to sponsor: 2018–Present), AstraZeneca Pharmaceuticals (2009–2014, declined to sponsor: 2014–Present); AuroMedics Pharma LLC (2021–2022, declined to sponsor 2022–Present); Aurobindo Pharma (2020–2022, declined to sponsor: 2022–present); Ortho-McNeil-Janssen Pharmaceuticals, Inc. (2009–2014, declined to sponsor: 2015–Present); Pfizer, Inc. (2009–2011, declined to sponsor: 2012–Present). As an employee of MGH, Dr. L.S.C. works with the MGH CTNI, which has had research funding from multiple pharmaceutical companies and NIMH.
Other research support: Brain & Behavior Research Foundation; National Institute on Aging; National Institutes of Health; SAGE Therapeutics. Advisory/Consulting: JDS Therapeutics LLC. Speaking/Honoraria: None. Royalty/patent, other income: None.
M.P.F.—as of 9/20/2022. Research Support: Dr. M.P.F. is an employee of MGH, and works with the MGH National Pregnancy Registry. MGH National Pregnancy Registry: Current Sponsors: Alkermes, Inc. (2016–Present); Eisai Inc. (2022–Present); Johnson & Johnson/Janssen Pharmaceuticals, Inc. (2019–Present); Otsuka America Pharmaceutical, Inc. (2008–Present); Sage Therapeutics (2019–Present); Sunovion Pharmaceuticals, Inc. (2011–Present); Supernus Pharmaceuticals (2021–Present); Teva Pharmaceutical Industries Ltd. (2018–Present). Past Sponsors: Forest/Actavis/Allergan (2016–2018, declined to sponsor: 2018–Present), AstraZeneca Pharmaceuticals (2009–2014, declined to sponsor: 2014–Present); AuroMedics Pharma LLC (2021–2022, declined to sponsor 2022–Present); Aurobindo Pharma (2020–2022, declined to sponsor: 2022–present); Ortho-McNeil-Janssen Pharmaceuticals, Inc. (2009–2014, declined to sponsor: 2015–Present); Pfizer, Inc. (2009–2011, declined to sponsor: 2012–Present).
Other Research Support: SAGE Therapeutics. JayMac. As an employee of MGH, M.P.F. works with the MGH CTNI, which has had research funding from multiple pharmaceutical companies and NIMH. Advisory/Consulting: Independent Data Safety and Monitoring Committees: Janssen (Johnson & Johnson), Novartis, Neurocrine; Advisory Boards: Eliem, Sage, Brainify, Everly Health. Speaking/Honoraria: WebMD, Medscape, Pri-Med, Postpartum Support International. Royalty/patent, other income: Scale Royalties—through MGH Scale, The Massachusetts General Hospital Female Reproductive Lifecycle and Hormones Questionnaire.
A.C.V.—as of 9/20/2022. Research Support: Dr. A.C.V. works with the MGH National Pregnancy Registry. MGH National Pregnancy Registry: Current Sponsors: Alkermes, Inc. (2016–Present); Eisai Inc. (2022–Present); Johnson & Johnson/Janssen Pharmaceuticals, Inc. (2019–Present); Otsuka America Pharmaceutical, Inc. (2008–Present); Sage Therapeutics (2019–Present); Sunovion Pharmaceuticals, Inc. (2011–Present); Supernus Pharmaceuticals (2021–Present); Teva Pharmaceutical Industries Ltd. (2018–Present). Past Sponsors: Forest/Actavis/Allergan (2016–2018, declined to sponsor: 2018–Present), AstraZeneca Pharmaceuticals (2009–2014, declined to sponsor: 2014–Present); AuroMedics Pharma LLC (2021–2022, declined to sponsor 2022–Present); Aurobindo Pharma (2020–2022, declined to sponsor: 2022–Present); Ortho-McNeil-Janssen Pharmaceuticals, Inc. (2009–2014, declined to sponsor: 2015–Present); Pfizer, Inc. (2009–2011, declined to sponsor: 2012–Present). Other Research Support: SAGE Therapeutics. Advisory/Consulting: Up-to-Date. Speaking/Honoraria: None. Royalty/patent, other income: None.
S.H.-D. —as of 9/20/2022. Research Support: National Institutes of Health. Epidemiologist for the North American Antiepileptic Drugs pregnancy registry and advisor for the Antipsychotics Pregnancy Registry, which are funded by multiple companies.
Other Research Support: None. Advisory/Consulting: Roche, UCB and Moderna. Advisor for the MGH National Pregnancy Registry: Current Sponsors: Alkermes, Inc. (2016–Present); Eisai Inc. (2022–Present); Johnson & Johnson/Janssen Pharmaceuticals, Inc. (2019–Present); Otsuka America Pharmaceutical, Inc. (2008–Present); Sage Therapeutics (2019–Present); Sunovion Pharmaceuticals, Inc. (2011–Present); Supernus Pharmaceuticals (2021–Present); Teva Pharmaceutical Industries Ltd. (2018–Present). Past Sponsors: Forest/Actavis/Allergan (2016–2018, declined to sponsor: 2018–Present), AstraZeneca Pharmaceuticals (2009–2014, declined to sponsor: 2014–Present); AuroMedics Pharma LLC (2021–2022, declined to sponsor 2022–Present); Aurobindo Pharma (2020–2022, declined to sponsor: 2022–Present); Ortho-McNeil-Janssen Pharmaceuticals, Inc. (2009–2014, declined to sponsor: 2015–Present); Pfizer, Inc. (2009–2011, declined to sponsor: 2012–Present).
Supplementary Material
Supplementary Figure S1
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.