
Abstract
Objectives:
To describe bariatric surgery patients' perioperative conceptualizations about pregnancy.
Materials and Methods:
We performed a secondary analysis of a cross-sectional study performed in 2016, evaluating a nationally recruited convenience sample of U.S. women aged 18–45 years who underwent bariatric surgery within the past 24 months. We assessed four pregnancy constructs: intent, desire, emotional orientation, and importance to avoid. We examined relationships between constructs, with time since surgery, postoperative pregnancy, and contraceptive use using descriptive statistics.
Results:
We included 363 eligible women (response rate 80%). Participant median age was 36 years, 71% (n = 258) were White, 77% (n = 279) were sexually active at the time of the study, and 39% (n = 140) experienced preoperative infertility. Most reported no desire to become pregnant (59%, n = 175) and that it was important to avoid pregnancy (78%, n = 283) within the first 24 months after surgery. Relationships between constructs were complex. Respondents in their first postoperative year more likely reported they would feel upset about a hypothetical pregnancy (40%, n = 74) than those in their second year (27%, n = 48, p = 0.02). Of those with a postoperative pregnancy, 46% (n = 17) felt it was important to avoid pregnancy compared with 81% (n = 266) of those who did not have a pregnancy (p < 0.001). Most used postoperative contraception (66%, n = 241), and those who felt it was important to avoid pregnancy more likely used contraception (82%, n = 197) than those who did not feel it was important (18%, n = 44, p = 0.01).
Conclusions:
Women undergoing bariatric surgery have diverse and complex conceptualizations about future pregnancy. These varied based on time from surgery and influenced postoperative contraceptive use.
Introduction
Approximately 80% of bariatric surgery recipients in the United States are women and 40%–50% are women of reproductive age. 1,2 Bariatric surgery provides effective long-term weight loss, reduces the incidence of obesity-related comorbidities, and decreases obstetric complications due to morbid obesity. 3 –7 However, there may be increased maternal and fetal risks to pregnancies conceived in the early postoperative period, although studies are conflicting about whether there is definitive risk of adverse birth outcomes. 5,7 –10
In response, professional obstetric and bariatric societies have recommended avoiding pregnancy for 12–18 months postoperatively and use of an effective contraceptive method during that time. 11 –13 In addition, the Center for Disease Control Medical Eligibility Criteria lists history of bariatric surgery within 2 years as a condition associated with increased risk in pregnancy. 14
Although these guidelines recommend providers educate patients about these potential risks, it is essential to consider that patients undergoing bariatric surgery may be interested in future reproduction. One study found that 33% of women desired pregnancy within 24 months after bariatric surgery, and another found 4.3% of women attempted conception in the first postoperative year compared with 13.1% in the second postoperative year. 15 Furthermore, as weight loss can improve fertility, some women may undergo bariatric surgery for this reason. 16,17 To inform the provision of patient-centered counseling related to future fertility for this population, it is essential that clinicians understand their reproductive desires.
How individuals conceptualize a potential pregnancy has increasingly been recognized as complex, and a conceptual model illustrating the various factors that impact this has been previously published. 18 –21 Although traditionally the desirability of a pregnancy for an individual woman has rested on assessment of pregnancy intention in both clinical and research contexts, this framing rests on the assumption of an entirely negative value assigned to unintended pregnancies and ignores the nuances of ambivalence or indifference. 18,19
Furthermore, desires for (both positive and negative) and emotional orientations toward pregnancy exist on a continuum, may not always align with pregnancy intentions, and may even change after conception. For example, a woman who highly desires to avoid pregnancy may have a positive emotional response to an unexpected pregnancy. 20,21 The four pregnancy constructs that have been previously described and that we use in this study are desire, intent, emotional orientation, and avoidance: desire being how much one wants a pregnancy, emotional orientation representing how happy one would be if pregnant, intent representing the degree of planning a pregnancy, and avoidance being how much one is trying to not be pregnant.
In this study, we explored these conceptualizations related to pregnancy, including intent, desires for, emotional orientation toward, and importance of avoiding pregnancy, in the first 24 postoperative months after bariatric surgery.
Materials and Methods
We performed a secondary analysis of a previously published cross-sectional study evaluating perioperative contraceptive use and pregnancy counseling in women aged 18–45 years who underwent bariatric surgery within 24 months of the study. 22 We recruited participants using targeted Facebook advertisements between June 2016 and October 2016 connecting to our secure web-based survey, and obtained electronic consent.
This secondary analysis used the same inclusion and exclusion criteria as the primary study: we included women who were 18–45 years old and underwent surgery within 24 months of the time of the survey, and excluded those with a history of hysterectomy or tubal ligation before bariatric surgery or who were sexually active exclusively with women. These final criteria intended to identify respondents to whom pregnancy prevention may be more relevant.
The primary aim of this secondary analysis was to quantify four pregnancy constructs (desire about, emotional orientation toward, importance of avoiding, and pregnancy intent) after having bariatric surgery and their relationships between one another when considering a hypothetical postoperative pregnancy. We used questions derived from existing literature examining these domains of pregnancy conceptualization and validated in various populations. 19,23
Specifically, we examined how the reported importance of avoiding pregnancy related to respondents' desires and emotional orientations toward pregnancy and how pregnancy intent related to desire, emotional orientation, and importance of avoiding pregnancy. Secondary aims included evaluating whether any differences existed in the four pregnancy constructs based on whether respondents reported receiving perioperative pregnancy or contraceptive counseling and for any differences in reported postoperative contraceptive use based on the pregnancy constructs. We determined our recruitment target in a previous study for this same data set. 22
The survey collected demographic, reproductive, and bariatric surgical histories; contraceptive use and type of method used postoperatively; and perioperative receipt of contraceptive and pregnancy interval recommendations. We assessed intention and planning around future childbearing by asking all respondents “are you planning to have (more) children?” with answer choices being “yes,” “no,” and “I don't know.” We then further clarified when after surgery they were planning to become pregnant: <6 months after surgery; 6–12 months after surgery; 1–2 years after surgery; or >2 years after surgery.
To assess conceptualizations of a hypothetical pregnancy, we asked about desire to be pregnant, anticipated emotional orientation toward pregnancy, and importance of avoiding pregnancy in the first 24 months after bariatric surgery. We assessed desire to be pregnant by asking “how much did you want to get pregnant?” with answer choices ranging from “not at all” to “very much” on a 5-point Likert scale. We assessed respondent's emotional orientation if they were to become pregnant by asking “how would you have felt if you got pregnant?” with possible answers ranging from “very upset” to “very happy.” We evaluated the importance of avoiding pregnancy in the 24 months after surgery by asking respondents “how important was it to avoid pregnancy?” with answer choices ranging from “very important” to “not important.”
We performed data analysis using Stata version 14.1 (College Station, TX, USA). We first calculated summary statistics using the appropriate parametric or nonparametric tests for continuous variables depending on distribution and with chi-squared tests for dichotomous or ordinal variables. We next used chi-squared tests to evaluate the association between pregnancy intent, desires, emotional orientations, and postoperative contraceptive use. We also used chi-squared tests to evaluate for any associations between the four pregnancy constructs with type of bariatric surgery, parity, race, and income. We considered statistically significant associations to have a p < 0.05.
We obtained approval from the University of California, San Francisco Institutional Review Board, before beginning the study.
Results
A total of 1086 people attempted to take the survey and 451 were eligible for the primary study as well as this secondary analysis. Of these eligible respondents, 363 (80%) completed the survey and were included in this analysis (Fig. 1). Demographic, reproductive, and surgical descriptors of the study population are listed in Table 1. Participant median age was 36 years, 71% (n = 258) were White, and 77% (n = 279) were sexually active at the time of the study. The study population was geographically diverse. One hundred eighty-five respondents (51%) were within their first postoperative year at the time of the survey, and 178 (49%) were within their second postoperative year.
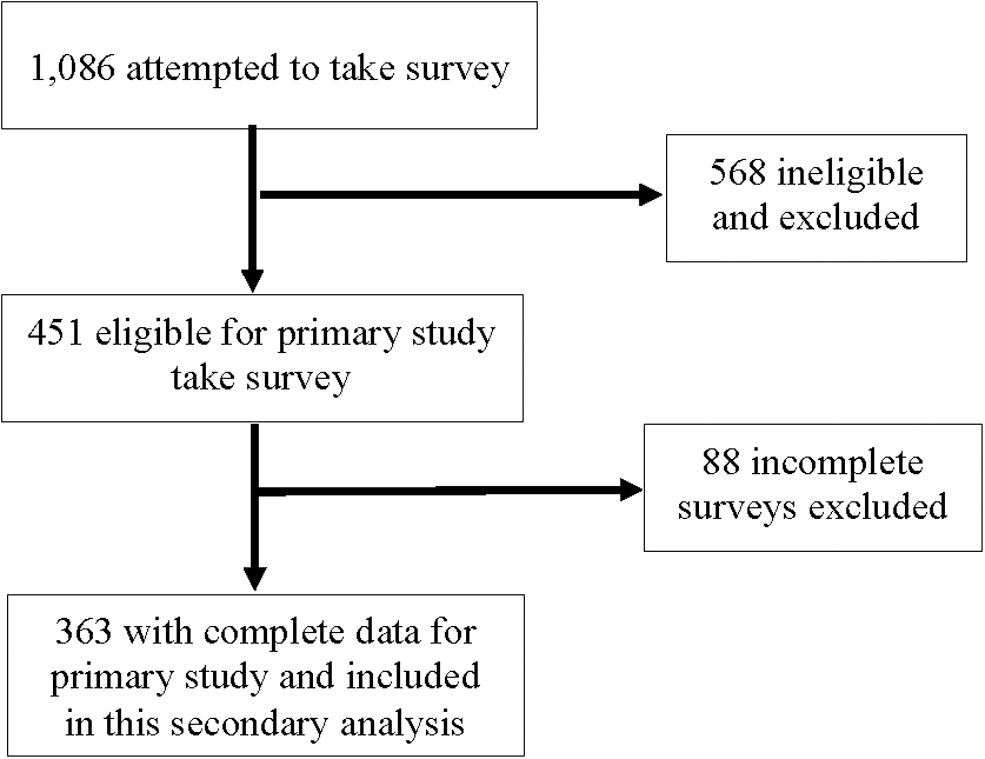
Respondents included in this secondary analysis from a primary cross-sectional study in 2016 evaluating postoperative contraceptive use and perioperative reproductive counseling in women of ages 18–45 years who underwent bariatric surgery within 24 months of study participation.
Demographic, Reproductive, and Bariatric Surgery Characteristics of Women of Ages 18–45 Years Who Underwent Bariatric Surgery Within 24 Months of Participating in a Study Evaluating Postoperative Pregnancy Conceptualizations in 2016 (N = 363)
IQR, interquartile range.
Preoperative fertility and postoperative pregnancies
Approximately 39% (n = 140) of respondents reported preoperative infertility. Improvement of fertility was a factor in the decision to pursue bariatric surgery for 26% (n = 93) of all respondents, of which 83% (n = 78) reported preoperative infertility. When asked whether planning a future pregnancy, 40% (n = 144) responded yes and 33% (n = 120) were unsure. Of those definitely planning a future pregnancy (n = 144), 15% (n = 22) desired this to be within the first year of surgery, 54% (n = 78) 1–2 years after surgery, and 31% (n = 44) >2 years postoperatively.
Overall, 37 postoperative pregnancies were reported at the time of the survey. Among the 185 respondents who completed the survey while in their first postoperative year, 6 postoperative pregnancies were reported. Thirty-one pregnancies were reported from those completing the survey in their second postoperative year (n = 178), with 10 pregnancies (32%) occurring in the first postoperative year and 21 (68%) in the second postoperative year. One participant had two pregnancies: one in the first postoperative year and another in the second postoperative year.
Fourteen postoperative pregnancies were reported from respondents who underwent a malabsorptive procedure (n = 118) and 22 pregnancies in those who underwent a restrictive procedure (n = 235). Of the 37 total postoperative pregnancies, 43% (n = 16) resulted in a live birth, 24% (n = 9) in miscarriage or stillbirth, and 30% (n = 11) were pregnant at the time of the survey (missing data from one respondent).
Postoperative pregnancy conceptualizations
Table 2 lists reported postoperative pregnancy conceptualizations. Although the majority did not desire to be pregnant and felt it was at least “somewhat important” to avoid pregnancy in the first 24 months after surgery, a substantial number of respondents reported they would feel at least “somewhat happy” if they did have a hypothetical pregnancy. Respondents in their first postoperative year were more likely to feel very or somewhat upset about a hypothetical pregnancy (n = 74, 40%) than those in their second year (n = 48, 27%, p = 0.02). Respondents in their first postoperative year more commonly reported it was very or somewhat important to avoid pregnancy (n = 152, 82%) compared with those in their second year (n = 131, 74%, p = 0.05).
Postoperative Pregnancy Conceptualizations (Intent, Desire, Emotional Orientation, and Importance of Avoiding a Hypothetical Pregnancy) Among Women of Ages 18–45 Years Who Underwent Bariatric Surgery Within 24 Months of Study Participation in 2016 (N = 363) with Comparison of Conceptualizations by Time Since Surgery and by Bariatric Procedure Type
Responses reported on a scale from 0 (not at all) to 5 (very much) and are reported as categorical data here.
There were no meaningful or statistically significant differences in the four pregnancy constructs by race, income, or surgery type. Respondents who were nulliparous were more likely to report planning a future pregnancy (54%, n = 77) compared with those who were not nulliparous (30%, n = 67, p ≤ 0.001).
Of those who had a postoperative pregnancy (n = 37), 46% (n = 17) felt it was very or somewhat important to avoid a hypothetical pregnancy compared with 82% (n = 266) of those who did not have a postoperative pregnancy (n = 326, p < 0.001). With respect to emotional orientation, 86% (n = 31) of those who had a postoperative pregnancy would feel very or somewhat happy if they were to become pregnant compared with 44% (n = 143) of those who did not have a postoperative pregnancy (p < 0.001). Intent and postoperative pregnancy were also correlated, with 67% (n = 24) of those who had a postoperative pregnancy intending to have a future pregnancy compared with 36% (n = 119) of those who did not have a postoperative pregnancy (p = 0.002).
Relationship between pregnancy constructs
We evaluated the relationships between the four pregnancy constructs that revealed complex relationships. Figure 2 demonstrates the relationship between emotional orientation toward pregnancy in the first 24 months after surgery in relation to the importance of avoiding pregnancy, revealing a relatively uniform spread across the various emotional orientations for those who felt it was important to avoid a hypothetical pregnancy. Among the 175 respondents with no desire for a hypothetical postoperative pregnancy, 83% (n = 146) reported it was somewhat or very important to avoid pregnancy in the first 24 months after surgery.

Respondents' reported emotional orientation toward a hypothetical pregnancy in the first 24 months after bariatric surgery in relation to reported importance to avoid pregnancy (N = 363).
Figure 3 shows the relationship between pregnancy intent and emotional orientation, revealing a nuanced relationship. Among those who did not intend a future pregnancy (n = 99), 92% (n = 88) noted having no desire to be pregnant and 80% (n = 79) noted that it was very important to avoid a hypothetical pregnancy (data not shown, p < 0.001).

Respondents' reported emotional orientation toward a hypothetical pregnancy in the first 24 months after bariatric surgery in relation to pregnancy intent (N = 363).
Relationship between perioperative pregnancy counseling, postoperative contraception, and pregnancy constructs
Overall, 66% (n = 241) of women used contraception in the first 12 postoperative months. Respondents who felt it was very important to avoid pregnancy were more likely to use postoperative contraception (p = 0.01, Fig. 4). Approximately 51% (n = 187) of respondents reported having discussions about perioperative pregnancy interval recommendations, with bariatric surgeons being the most commonly cited source of these recommendations (n = 173, 92%). We evaluated whether having perioperative pregnancy counseling influenced perceptions about the importance to avoid a hypothetical postoperative pregnancy.

Rates of contraceptive use and nonuse in the first 12 postoperative months in relation to respondents' reported importance to avoid pregnancy in the first 24 months after bariatric surgery (N = 363).
Having perioperative counseling was not associated with reporting that it was either “very important” or “somewhat important” (n = 151, 81%) to avoid pregnancy compared with those who did not feel it was important (n = 113, 78%, p = 0.7). However, having perioperative pregnancy counseling or not did demonstrate differences in pregnancy desire, emotional orientation, and whether a respondent was planning a future pregnancy. With respect to pregnancy desire, those who received counseling were more likely to report a higher postoperative pregnancy desire (54%, n = 79) than those who did not receive counseling (26%, n = 38, p = 0.009).
Those who did not receive perioperative counseling were more likely to report they were not planning a future pregnancy (41% vs. 19%, p ≤ 0.01) and that they would feel very or somewhat upset if a pregnancy occurred (44% vs. 28%, p = 0.005).
Discussion
Most women felt it was very important to avoid pregnancy in the 24 months after surgery, consistent with national recommendations. However, the relationships between pregnancy intention, desires, emotional orientations, and the importance of avoiding pregnancy were complex; many, including those who felt it was important to avoid pregnancy, had some desire for pregnancy and a positive emotional orientation toward the possibility of pregnancy in that same time period. We also found that a substantial minority underwent bariatric surgery for improved fertility.
And although most respondents felt that it was important to avoid pregnancy in the first 24 months, over half of those wishing to have a future pregnancy desired it within 2 years of surgery and 40% of respondents who reported a postoperative pregnancy had one within the first postoperative year.
Our study provides a nuanced description of women's perioperative pregnancy conceptualization during the bariatric surgery process, and to our knowledge is the first study to evaluate these pregnancy constructs in women receiving bariatric surgery. Our findings are also consistent with other studies that have described that conceptualization of pregnancy is a complex construct in the broader population of people who have the capacity for pregnancy. For example, women who unequivocally voice desire to avoid pregnancy can also have a positive emotional orientation to the idea of becoming pregnant based on their consideration of the positive and negative implications of a pregnancy at any given time. 18,21,22
Women undergoing bariatric surgery undoubtedly also experience this complex interaction of many personal and reproductive factors that inform their motivations to undergo surgery as well as future childbearing, including infertility, weight loss, and potential maternal or fetal risks in early postsurgical pregnancies.
Public health experts and pregnancy care providers inherently desire to optimize and improve both maternal and fetal outcomes. However, the counseling that arises from this desire must be informed by individual preferences and needs, especially as it relates to reproduction. This is especially true for outcomes that have yet to be definitely proven, such as the risks of an early postoperative pregnancy after bariatric surgery, for which evidence has been somewhat conflicting.
In addition, many of the risks identified in existing literature are mainly fetal in nature, highlighting the potential conflict of maternal desires and autonomy with fetal well-being. Bariatric and reproductive health care providers alike should make an intentional effort to engage in patient-centered counseling about perioperative pregnancy interval and contraceptive use. This may include counseling about the recommendations for pregnancy intervals in the context of conflicting available data regarding risk, and explicitly discussing pregnancy intention, desires, and emotional orientation so that patients may make informed decisions about pregnancy within a supportive environment.
Strengths of this study include the large number of respondents as well as the demographic similarity of our study population to the general bariatric surgery population, making our results more generalizable. 24,25 An additional strength is that we used questions derived from existing literature examining these domains of pregnancy conceptualization and validated in various populations, although not in a bariatric population. Our study is limited; however, given our online recruitment method utilizing a convenience sample of Facebook users, our study population may not be representative.
An additional limitation is that we surveyed respondents at a single point in time who were at different stages in their postoperative course compared with one another, with 50% still being within their first postoperative year, and asked them to retrospectively report on their conceptualizations of pregnancy. As a result, both time since surgery and reproductive experiences between surgery and the time of the survey may have influenced responses. Lastly, we relied on self-report to document the occurrence of perioperative discussions and counseling, which may not be accurate and may be impacted by recall bias.
Conclusion
Pregnancy conceptualization is complex, and this is evident in our study of a reproductive-aged population who have undergone bariatric surgery. Most participants in our study felt that avoiding pregnancy in the first 24 months postoperatively was important, however, many also expressed positive emotional orientation or desire for a pregnancy. As the prevalence of obesity continues to increase in the United States, a growing number of reproductive-aged women may utilize bariatric surgery for successful weight loss and comorbidity reduction.
This makes gaining a detailed understanding of the nuances surrounding pregnancy intention, desires, emotional orientation, and reproductive health counseling preferences imperative. Providers should make a concerted effort to maintain a patient-centered approach to perioperative counseling and recommendations around pregnancy and contraception utilizing shared decision making. 26 In addition to needing more studies that specifically evaluate appropriate timing of pregnancy after bariatric surgery and risks of an early postoperative pregnancy, future qualitative studies are needed to further understand women's pregnancy desires and orientations in the context of bariatric surgery as well as explore strategies to optimize perioperative reproductive health counseling centered upon patient preferences.
In addition, bariatric and reproductive health care experts and organizations, ideally in collaboration, should develop evidence-based patient-centered interventions that adequately address patient's concerns regarding pregnancy and reproductive health in the perioperative period to support health care providers in delivering quality comprehensive care.
Footnotes
Authors' Contributions
B.M. contributed to conceptualization, methodology, formal analysis, writing—original draft, and funding acquisition. J.S. was involved in conceptualization, methodology, writing—reviewing and editing, and supervision. J.C. was in charge of methodology, resources, and writing—reviewing and editing. A.R. took care of project administration, investigation, and writing—reviewing and editing. C.D. was in charge of conceptualization, methodology, writing—reviewing and editing, and supervision.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This study was supported by the Society of Family Planning Research Fund (Grant No. SFPRF 16–18).