
Abstract
Cardiovascular diseases (CVD), including coronary artery disease (CAD), continue to be the leading cause of global mortality among women. While traditional CVD/CAD prevention tools play a significant role in reducing morbidity and mortality among both men and women, current tools for preventing CVD/CAD rely on traditional risk factor-based algorithms that often underestimate CVD/CAD risk in women compared with men. In recent years, some studies have suggested that breast arterial calcifications (BAC), which are benign calcifications seen in mammograms, may be linked to CVD/CAD. Considering that millions of women older than 40 years undergo annual screening mammography for breast cancer as a regular activity, innovative risk prediction factors for CVD/CAD involving mammographic data could offer a gender-specific and convenient solution. Such factors that may be independent of, or complementary to, current risk models without extra cost or radiation exposure are worthy of detailed investigation. This review aims to discuss relevant studies examining the association between BAC and CVD/CAD and highlights some of the issues related to previous studies' design such as sample size, population types, method of assessing BAC and CVD/CAD, definition of cardiovascular events, and other confounding factors. The work may also offer insights for future CVD risk prediction research directions using routine mammograms and radiomic features other than BAC such as breast density and macrocalcifications.
Background
Cardiovascular disease (CVD), including coronary artery disease (CAD), continues to be the leading cause of global mortality in both men and women, with women at a greater risk of stroke than men. 1 Based on recent statistics from the United States, cardiovascular mortality has recently increased by 1% annually in women aged ≤55 years, and globally, about 20% of ischemic heart disease events in women occur in the absence of the traditional cardiovascular risk factor. 2,3 Suboptimal prevention of CVD in women, due to many factors including underdiagnosis, undertreatment, system bias, and poorly identified gender-specific risk factors, is of great concern, 4 –6 particularly since women often present later with symptoms of CVD/CAD compared with men. CVD/CAD symptoms in women are often “atypical” unclear or nonspecific compared with traditional symptoms in men. 7
To identify those at high risk of CVD, current techniques rely on risk factor-based algorithms; however, these algorithms perform poorly in women and often underestimate CVD/CAD risk in women. 8 Furthermore, women are less likely than men to have CVD screening or seek help from a general practitioner, while it has been demonstrated, medical practitioners may be less inclined to screen women for CVD compared with men. 7 Hence, additional approaches beyond the traditional medical practitioner led risk factor-based algorithms are required to engage women in cardiovascular (CV) screening and identify women who might be at risk of CVD and most likely to benefit from preventative medical therapy and close monitoring. It is clear that a novel and gender-specific risk assessment strategy is required.
In 1995, Moshyedi et al. 9 demonstrated an association between breast arterial calcification (BAC) and CVD/CAD risk factors in women younger than 59 years. Since then, several studies have explored this association, and the majority have confirmed a positive relationship between BAC and CVD/CAD. 10 –26 These studies, however, had limitations relating to sample size, biased populations, CVD events definitions, unknown confounding variables, and variation of the methods used for identifying and quantifying BAC on mammograms. In this review, we focus on some of these limitations in using BAC to determine the risk of CV events and offer insights for future research directions on CV risk prediction using routine mammograms and other radiomic features.
What is BAC?
BAC is a form of medial arterial calcification (MAC), known as Mönckeberg sclerosis, affecting the entire circumference of the mammary vessel and decreasing arterial compliance. 27,28 It can be referred to as peripheral arterial arteriosclerosis, which occurs due to the loss of elasticity of the arteries making them hardened and thick. 29,30 MAC, or Mönckeberg sclerosis, 31 refers to vascular calcification of the medial layer of the vascular wall and mostly affects peripheral arteries with an inclination to be observed in muscular arteries causing loss of elasticity. 32 –34 MAC reflects a process of active calcification resembling bone formation and is often associated with aging, diabetes, and end-stage kidney disease. 35
BAC commonly occurs in small to medium size muscular arteries, including small arterioles; 4,27,36 however, O'Neill and Adams 36 suggested no relationship between artery size and its susceptibility to calcification. Given the small sample size of 19 patients in the study, 36 further data are required to understand the relationship between artery size and the presence of BAC and a potential association should not at this stage be ruled out. Specifically, future studies focusing on the influence of vessel size, type, and other anatomical factors on susceptibility to calcification are needed. 37
BAC can be detected on a mammogram by the presence of parallel lines or tubular tracks; 38,39 however, its identification is still a challenging task for various reasons including differences in size and shape of the lesion, as well as varying contrast of images. 38,40 Also, the nonuniformity in the calcium density within arteries results in topological complexity of BAC lines. 2,41 As illustrated in Figure 1, BAC can exhibit as disconnected, strongly connected, thin, or overlapping lines. 40 Furthermore, BAC is not always clearly visible, resulting in a breast with normal appearances. 41
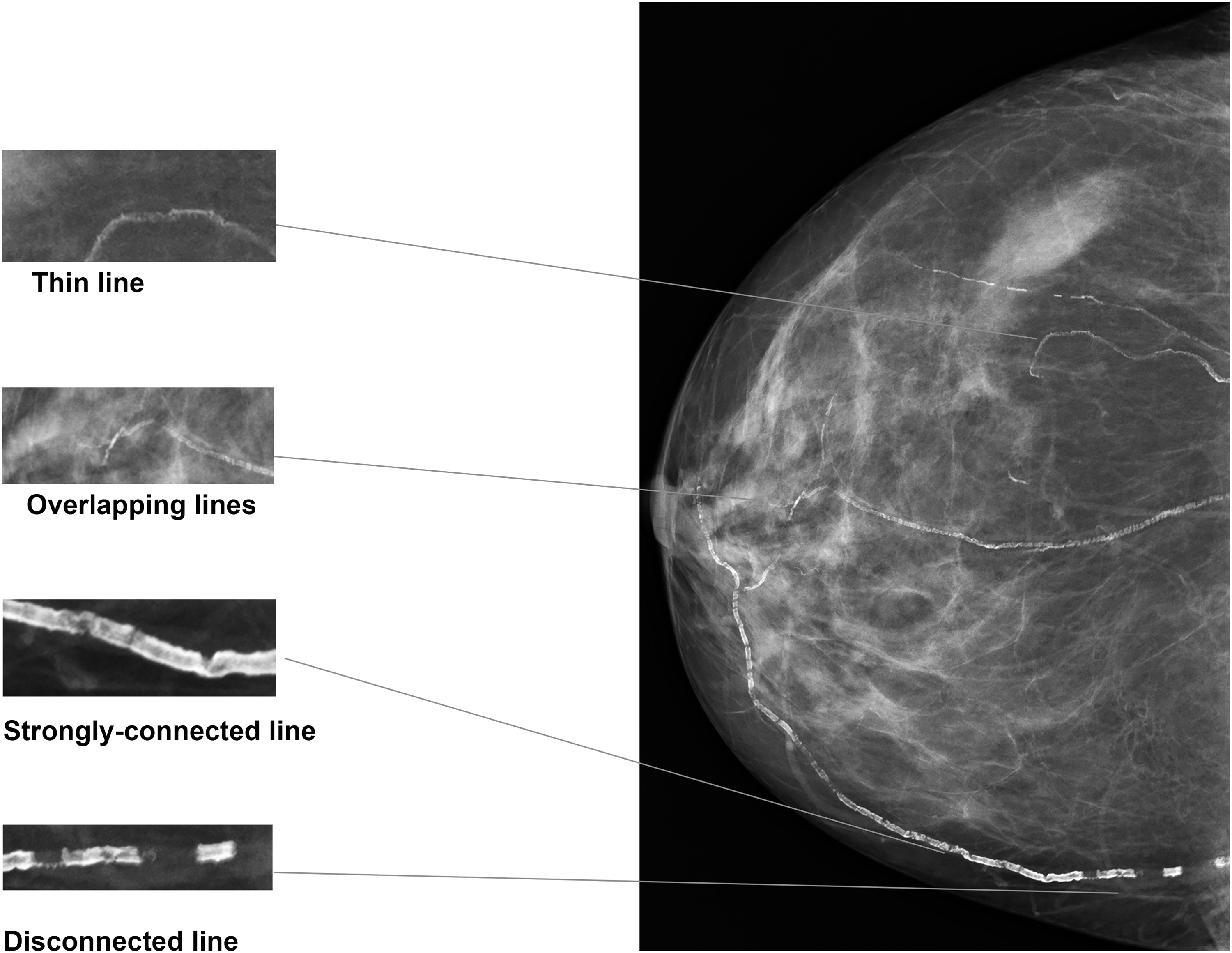
Examples of different appearances of BACs. BAC, breast arterial calcification.
Prevalence of BAC
The prevalence of BAC in mammography is inconsistent and depends on the study population. Pooled analysis of data from 18 studies conducted in a general population yielded a prevalence estimate of 12.7% (95% confidence interval [CI] 10.4%–15.1%). 42 Among different predictors, age is the most explored factor. Reddy et al. 43 conducted a cross-sectional study of 1,905 females with a mean age of 57.6 years: the participants were divided into five age groups, 35–44, 45–54, 55–64, 65–74, and 75–90 years, and the prevalence of BAC among these age groups was shown to be 3.9%, 15.1%, 31.8%, 55.7%, and 54.4%, respectively. According to a meta-analysis of 10 studies, 42 age is a significant determinant with an odds ratio (OR) of 2.98 (95% CI 2.31–3.85) for every 10 year increase. 42
Reproductive and hormonal factors also affect the prevalence of BAC. A meta-analysis of seven studies found that parous women had an OR of 3.43 for the presence of BAC compared with nonparous women. 42 Moreover, number of children and breastfeeding have found to be positively associated with the presence of BAC. 42 BAC is more common after menopause and less frequent in women receiving hormone replacement therapy. 44 Race is also another important risk with BAC prevalence reported highest among Hispanics (35%), followed by African Americans (25%), Caucasians (24%), and finally Asians (7%). 43
Association Between BAC and CVD
BAC is generally considered a benign finding in mammograms. It has been known to radiologists for a long time; however, little clinical significance was linked to it until 1980 when researchers discovered an association between the presence of BAC and diabetes mellitus. 45 Since that time, multiple studies have been conducted to evaluate the association between BAC and other diseases such as CVD or CAD. Iribarren et al. 46 conducted a study on 5,059 postmenopausal women (with no symptoms of CVD/CAD) aged between 60 and 79 years who underwent breast screening from October 2012 to February 2015.
BAC was present in 26% of these women. To investigate the relationship between BAC and atherosclerotic cardiovascular disease (ASCVD) and global CVD, the authors performed a follow-up after 6.5 years and found that the presence of BAC was strongly associated with ASCVD and global CVD with increased hazard ratios (HRs) of 1.51 (95% CI 1.08–2.11; p = 0.02) and 1.23 (95% CI 1.002–1.52; p = 0.04), respectively. One major issue of this study is that its findings may not be generalizable to women younger than 60 years.
To date, most studies have confirmed a positive relationship between BAC and CVD/CAD; 10 –26 however, one should acknowledge that a small number of other studies have failed to show a relationship. 47 –49 The studies included in this review article is summarized in Table 1. In this section, we briefly review the studies investigating the association between BAC and (1) coronary artery calcium (CAC)/subclinical CAD, (2) peripheral arterial disease, (3) stroke, and (4) cardiovascular mortality. Differences in the conclusions from these studies may be related to study design, the number of participants, age of participants, methods of assessing BAC, and detecting CVD. Some of the key issues regarding these studies are discussed below.
Summary of Studies Investigating the Association Between Breast Arterial Calcification with Cardiovascular Diseases/Coronary Artery Disease and Other Diseases
ASCVD, atherosclerotic cardiovascular disease; BAC, breast arterial calcification; BMD, bone mineral density; CAC, coronary artery calcium; CAD, coronary artery disease; CAD-RADS, Coronary Artery Disease-Reporting and Data System; CC, case–control; CCAP, calcified carotid artery plaque; C-IMT, carotid intima-media thickness; CKD, chronic kidney disease; CS, cross-sectional, CTCA, computed tomography coronary angiography; CV, cardiovascular; CVD, cardiovascular diseases; DM, diabetes mellitus; ESRD, end-stage renal disease; FRS, Framingham Risk Score; HL, hyperlipidemia; HRT, hormone replacement therapy; MI, myocardial ischemia; MPS, myocardial perfusion scan; MS, metabolic syndrome; MSCT, multislice computed tomography; N/A, not applicable; OCA, oral contraceptive agent; P/A, presence/absence; PAC, peripheral arterial calcification; PAD, peripheral arterial disease; PCE, the 2013 Cholesterol Guidelines Pooled Cohort Equations.
BAC and CAC/subclinical CAD
Although the etiology of coronary arterial calcification is predominantly intimal which differs from BAC, that strictly involves medial calcification, 50 several studies have suggested that there is a correlation between the presence of BAC and CAC scoring. 24,50 –55 CAC scoring is considered one of the most promising methods for identifying the risk of experiencing a CAD event; however, the high cost and radiation exposure associated with the use of computed tomography (CT) to establish CAC scores are two major disadvantages preventing CAC scoring from being implemented on a wide scale. 4 Interestingly, however, millions of women undertake breast screening mammograms every year across the world while some of these also undergo CAC scoring for CAD screening. This provides an excellent opportunity to explore potential associations between BAC and CAC that could enable a sex-specific method for predicting the risk of CAD in asymptomatic women with low cost and no extra radiation exposure. 56
To date, the potential association between BAC and CAC has been confirmed: Maas et al. 50 conducted a prospective study among 499 women with follow-up period between 6 and 11 years and found a positive relationship between the presence of BAC and the development of CAC >0 with an adjusted OR of 2.0 (95% CI 1.03–3.86); Chadashvili et al. 52 conducted a small retrospective study of 145 women and used CAC score >11 as the measurement outcome of CAD and found an adjusted OR of 4.53 (95% CI 2.04–10.08) for patients with BAC; Newallo et al. 53 investigated the relationship between BAC and CAC score >100 among 204 African American women and showed a significant association with an OR of 7.66 (95% CI 2.75–21.29); Matsumura et al. 55 used CAC score >400 as assessment outcome in their cross-sectional study among 202 women and found a strong link between CAC and BAC with an OR of 22.6 (95% CI 2.1–237.1).
It is important to note that these previous studies simply focused upon the presence or absence of BAC but not the severity of BAC. When semiquantitative techniques were used to measure the extent of BAC in, for example, 2,100 asymptomatic women, a positive relationship between the severity of BAC with CAC score >0 was found with an OR of 2.87 (95% CI 1.67–4.93). 24 Margolies et al. 54 conducted a retrospective study of 292 women using semiquantitative methods and showed a positive relationship between BAC and CAC score >0 with an adjusted OR of 3.2 (95% CI 1.8–5.9). It is important to acknowledge another study 57 that found no significant association between BAC severity and CAC score; however, this study only included a small number of symptomatic women (n = 150).
Coronary Artery Disease-Reporting and Data System (CAD-RADS) is another approach to reporting CT angiography and serves as clinical management guidelines of CAD. 58 It has grading systems ranging from 0 to N, where a CAD-RADS score from 0 to 2 indicates no CAD, and a CAD-RADS score ≥3 indicates CAD. 58,59 Kelly et al. 59 conducted a study to evaluate the association between the presence and severity of BAC with CAD-RADS ≥3 on 104 women who reported chest pain (aged between 50 and 65 years) and underwent both a coronary CT angiography (CCTA) and a breast screening.
The study concluded that the presence and severity of BAC linked with CAD-RADS ≥3 in asymptomatic women. To evaluate if the previous study's findings can be generalized to the broader screening mammograph population, Huang et al. 60 performed a study on 213 asymptomatic women aged between 40 and 85 years to investigate the relationship between BAC and CAD-RADS based on deep learning (DL)-CT angiography. In their multivariate analysis, they found that the presence of BAC is significantly associated with CAD-RADS ≥3 with an OR of 10.22 (95% CI 2.86–36.49, p < 0.001).
BAC and peripheral arterial disease
Peripheral arterial disease (PAD) is a progressive and debilitating form of CVD, which is often only diagnosed when a patient becomes symptomatic, resulting in underestimation of disease burden and delays in early intervention. 61 Iribarne et al. 62 conducted an extensive study (n = 3,800) of menopausal women aged between 60 and 79 years to assess the association between BAC and PAD. They use the ankle–brachial index (ABI) as a measuring metric of PAD. An ABI <0.9 is considered a low ABI and indicates the presence of PAD, an ABI between ≥0.9 and <1.3 is normal and no PAD, and an ABI ≥1.3 is a high ABI and indicates stiff arteries. Their result showed that the presence of BAC is significantly associated with ABI <0.9 with an adjusted OR of 1.36 (95% CI 0.99–1.85; p = 0.05). Also, they found no correlation between the presence and severity of BAC with ABI ≥1.3. The main drawback of this study is that the findings may not generalize to younger women.
Furthermore, three more studies with smaller populations focusing on populations greater than 100 women have shown a clear association between BAC and PAD, where BAC can be used as a marker of peripheral arterial disease: Dale et al. 63 conducted a study on 121 women who underwent both mammography and have history of PAD, retrieved from their medical records, and found a significant relationship between the presence BAC and PAD with an OR of 3.09 (95% CI 2.1–4.7); Abou-Hassan et al. 64 conducted a study on 202 women with end-stage renal disease (ESRD) and identified a strong correlation between BAC and PAD with an OR of 4.56 (95% CI 1.20–17.3); Markopoulos et al. 65 in 110 women also identified a strong relationship between BAC and PAD (femoral and carotid disease). These works suggest that BAC may reflect an individual's risk of MAC; however, given the paucity of studies, small sample sizes, 63 –65 and heterogeneous study populations, there may be confounders. Therefore, a large prospective study is needed to confirm the association of BAC with systemic arteriosclerosis or peripheral arterial disease.
BAC and stroke
Several studies have shown that the presence of BAC is a marker of the incidence and prevalence of stroke. 10,13,50,66 –69 While most of these studies looked at stroke as part of the definition of CVD/CAD or as a secondary outcome, 27 only one cohort study 66 focused specifically on the association between BAC and stroke. Iribarren et al. 66 studied a population of 12,761 women all of whom had attended multiphasic health checkups and screening mammography. Such multiphasic checkups gather comprehensive medical and laboratory tests results as well as patient histories, all of which are used to assess a variety of outcomes, including ischemic stroke, hemorrhagic stroke, and transient ischemic attack (among other CVD-related outcomes).
All these patient data were extracted from the beginning of 1971 until the end of 2000 with a median follow-up period of 24.8 years. The authors found a positive relationship between BAC and ischemic stroke, hemorrhagic stroke, and transient ischemic attack with an age-adjusted HR of 1.41 (95% CI 1.1–1.8), 1.43 (95% CI 0.79–2.60), and 1.44 (95% CI 0.77–2.70), respectively. Iribarren et al. 46 investigated the association between BAC and global CVD in 5,035 postmenopausal women. They included ischemic stroke and hemorrhagic stroke as part of the definition of global CVD. The authors found that the prevalence of ischemic stroke and hemorrhagic stroke is higher among women with BAC compared with those without and statically significant with a p value of 0.048.
Schnatz et al. 67 studied 1,454 individuals, where the relationship between the BAC and stroke was reported as a secondary outcome. The authors used a self-reported survey to understand patient history, including self-reported personal history of CAD, and concluded that BAC was a significant indicator of increased risk of CAD and stroke. However, the study did not specify differences between ischemic and hemorrhagic strokes. The relationship between BAC and stroke has been confirmed in other cross-sectional studies 10,13,68,69 involving self-reporting of stroke: Kataoka et al. 13 and van Noord et al. 69 reported adjusted ORs for stroke of 2.02 (95% CI 0.61–6.69) and 1.4 (95% CI 1.1–1.9), respectively, for patients with BAC; Crystal et al. 10 and Rotter et al. 68 showed a significant relationship between BAC and stroke with crude ORs of 4.9 and 4.4, respectively; Shah et al. 27 in their meta-analysis involving 7 investigations studied 30,673 participants and found that 5 of these studies reported a statistically strong association between BAC and stroke concluding that BAC could serve as a predictor of stroke.
BAC and cardiovascular mortality
Kemmeren et al. 70 investigated the relationship between BAC and CVD mortality in a population of 12,084 women aged 50–68 years who underwent breast screening mammography and were followed up for a period of 16–19 years. The authors found that BAC was associated with CVD and CAD mortality with HRs of 1.22 and 1.36, respectively. In addition, the study showed that diabetic women with BAC have a higher risk of CVD and CAD mortality compared with those individuals with BAC but nondiabetic with HRs of 1.71 and 1.76, respectively. The association between BAC and CVD mortality was also investigated in the study of Iribarren et al., 46 which showed a strong association between BAC and the prevalence of CVD mortality among postmenopausal women.
Hendriks et al. 71 conducted a study on 163 women who underwent CT scans to investigate the associations of BAC, splenic, and internal and external iliac arteries with CVD-related and non-CVD-related mortality; however, the number of women who had BAC in this study was very small (n = 6). The authors found a strong association between BAC on CT and CVD mortality and total mortality with age-adjusted HRs of 12.30 (95% CI 2.84–53.37) and 4.67 (95% CI 1.57–13.88), respectively. 71
Literature focusing on the relationship between BAC and CVD/CAD mortality is scarce; however, several studies suggested that calcification of arteries from different parts of the body such as the pelvis, thigh, and spleen can increase the risk of CVD mortality. 34,72 –74 MAC in the pelvis and thigh in ESRD patients was found to be a strong independent predictor of cardiovascular mortality. 34 Furthermore, MAC in femoral arteries among diabetic patients was also found to have a strong association with mortality from CVD and CAD. 75 These results are understandable as MAC causes reduced elasticity in the arteries, increasing systolic blood pressure and reducing diastolic blood pressure, which in turn may lead to increased cardiac afterload, hypertrophy, and increased risk of myocardial infarction and heart failure. 72,74
Methodological Heterogeneity
Limited sample size
Although many studies have demonstrated an association between BAC and CVD/CAD, there are a few studies that have reported no relationship between BAC and CVD/CAD. For example, two studies conducted by Penugonda et al. 47 and Zgheib et al. 48 investigated the relationship between BAC and CVD/CAD and reported that BAC is not associated with CVD/CAD. However, the sample sizes were very small in both studies with only 94 in Penugonda et al. 47 and 104 in Zgheib et al. 48 Furthermore, Moradi et al. 57 studied the association between BAC and CAC scores and the severity of coronary artery stenosis and found no association. Again, the number of participants in this study was relatively small, with only 150 participants. These conflicting results around the association between BAC and CVD/CAD have highlighted the need for a larger sample size or robust systematic reviews to increase study power and thus give a better understanding of the association between BAC and CVD/CAD.
Since 2014, five systematic reviews and meta-analyses have been performed, providing insight into the correlation between BAC and CVD/CAD. 4,8,27,76,77 Lee et al. 8 included 31 studies (n = 35,583) in their meta-analysis defining CAD as any CV events that were reported by participants, retrieved from medical records, or obtained through direct diagnostic procedures, such as coronary angiography, myocardial perfusion scan, and CT. Their results suggested a strong association between BAC and CAD with a pooled OR of 2.61 (95% CI 2.12–3.21). 8 Mohammed et al. 76 included 18 studies in their meta-analysis with a total of 33,494 women, and they found a significant relationship between BAC and CAD with a crude OR of 2.14 (95% CI 1.63–2.81). In addition, they were able to extract the adjusted OR for 10 studies, and the relationship between BAC and CAD for these 10 studies was still significant with an adjusted OR of 2.39 (95% CI 1.68–3.41).
A further meta-analysis by Hendriks et al. 77 analyzed the medical history and records used in 52 studies assessing the relationship between BAC and CVD/CAD, traditional CV risk factors, and reproductive factors. The authors reported that BAC was linked to the increased risk of CVD with adjusted HRs ranging between 1.32 (95% CI 1.08–1.60) and 1.44 (95% CI 1.02–2.05). However, the authors acknowledged that the diversity of study designs and scarcity of longitudinal studies, which make the conclusions less certain. Even with these reviews, however, it is still unclear if BAC measurements can be used reliably as a screening tool for CAD in asymptomatic women since the previous work was predominantly of cross-sectional design and did not specifically target a primary prevention cohort.
Biased populations
There are similar studies that found positive 78 or no relationship 25 between BAC and CAD, but many of these were limited by selection bias, which makes generalizing results from symptomatic to asymptomatic patients difficult. An ideal method of investigating the relationship between BAC and CAD would only involve asymptomatic women undergoing routine screening mammograms and direct diagnostic procedures such as coronary angiography and CT angiography for diagnosis of CAD. 27 However, it is extremely difficult to perform or find both routine mammogram and coronary imaging data on a primary prevention cohort since direct diagnostic procedures of CAD are expensive, generally involve ionizing radiation and risk, and not being covered by private health insurance in many countries. Therefore, medical practitioners usually do not refer patients for these procedures unless they have symptoms of CAD.
Mostafavi et al. 78 performed a cross-sectional study among 100 women undergoing CT angiography and concluded that BAC is associated with CAD. However, this study had two major limitations: the number of participants was very small, and most participants had intermediate to high CVD risk. In contrast, McLenachan et al. 25 conducted a cross-sectional study among 405 women and their study showed that BAC was not an adequate indicator of the presence of CAD on CT angiography. However, a significant portion of the studied population suffered from typical angina episodes, which means that the conclusion of this work was again limited to symptomatic women. Furthermore, Fathala et al. 79 investigated the relationship between BAC and myocardial ischemia on stress myocardial perfusion scanning by conducting a study on 435 women divided into 2 groups: 177 without BAC and 255 with BAC.
Their results showed no relationship between myocardial ischemia and BAC. Again, selection bias was a major limitation of this study, where the prevalence of CAD and BAC among the participants was high. Also, the prevalence of BAC in this study was significantly high (59%), especially compared with the prevalence of 15.2% in the study of Shobeiri et al., 80 which was conducted on 400 women and reported a positive relationship between BAC and myocardial ischemia. Yoon et al., 24 however, found a positive relationship between BAC and CAD and that the severity of BAC was strongly associated with CAD. Their study was conducted on 2,100 Korean women who underwent mammography and CT angiography as part of health checkup in Korea every 2 years: thus focusing on women without symptoms of CAD potentially yielding more generalizable findings.
Two early meta-analyses 22,81 assessing the association between BAC and CAD showed a positive relationship between BAC and CVD or CAD with ORs of 3.86 (95% CI 3.24–4.59) and 1.59 (95% CI 1.21–2.09), respectively. However, it has been highlighted that the populations studied in these two meta-analyses 22,81 were biased as the selection criteria were limited to studies that used coronary angiography as a measurement tool of CAD. 8 Coronary angiography is usually undertaken in patients who have a higher likelihood of CVD/CAD based on symptoms; hence, it could be inaccurate to conclude from these data that BAC is useful as a screening tool for CVD/CAD on asymptomatic women without prior CVD events or symptoms.
Definition of CV events
Differences in the methods used to identify and measure CVD/CAD outcomes are apparent across studies investigating the association of BAC. CAD and CVD definitions ranged from major adverse cardiovascular events (MACE) outcome including stroke, myocardial infarction, peripheral vascular disease arterial ischemia, and CVD mortality to the presence of CAD on coronary imaging. Others only included one CV outcome, a subgroup of CV outcomes, or only CVD mortality, which may have led to an underestimation of the association between BAC and CVD/CAD.
In addition, methods for determining the presence of CAD differed among studies, including self-reporting, coronary angiography, CT, and carotid intima-media thickness ultrasound test, which is a well-known predictor of CAD and cardiovascular morbidity and mortality. 82 Lee et al. 8 in their meta-analysis demonstrated that the association between BAC and CVD/CAD was strongest when based on CT, self-reporting may be inaccurate and biased, and invasive coronary angiography can underestimate calcification and nonobstructive coronary plaque burden. The ORs were 2.16 (95% CI 1.83–2.55), 2.14 (95% CI 1.40–3.29), and 3.90 (95% CI 2.53–6.03) for self-reporting, coronary angiography, and CT, respectively.
Differences when considering confounding factors
BAC and CAD increase with advancing age, making age a major confounding factor when exploring associations between the two clinical conditions. Most studies, including recent systematic reviews and meta-analyses, 4,8,27,76,77 have shown that the BAC/CAD association remains significant after stratifying or adjusting for age. However, Henkin et al. 49 argued that this association might also be due to other confounding variables associated with CAD risk and reported that the association of BAC and CAD, after adjusting for other CV risk factors including age, diabetes, and hypertension, to be diminished to a multivariate-adjusted OR of 0.96 (95% CI 0.56–1.64). This result is incongruent with other multivariate analyses, 10,15,18,23,53,68 which still reported a robust independent relationship between BAC and CAD after adjustment of confounding CV risk factors.
Several studies 54,55,64,78 controlled their findings based on smoking history—a significant risk factor for early onset and CV disease and still reported a strong association between BAC and CAD. However, Lee et al. 8 suggested that simply controlling for smoking may not be enough to draw a conclusion about this association and studies need to stratify their finding based on smoking history more robustly to test this association.
Differences in the BAC assessment methodologies
BAC is usually assessed manually by radiologists when reading mammograms as present or absent, which only allows classification of a primary prevention cohort of women into two CVD risk categories. The ability to assess BAC severity can improve the accuracy of predicting the risk of developing CVD in asymptomatic women using standard mammography and allows to classify patients into various CVD risk groups. 3 Several recent studies have proposed various methods for grading and assessing the severity of BAC, including a 3-point scale, 51 4-point scale, 18,25,57,78,83 –85 and 12-point scale. 54,79,86,87 Different criteria were considered for grading BAC in these studies such as the density of calcium, length of vessel, and number of affected vessels. 8
Despite these efforts, the variation in grading scales indicates the absence of standardized criteria for quantifying BAC. Furthermore, there are other challenges preventing BAC assessment from being part of the clinical routine such as that radiologists may not have the adequate knowledge to assess BAC and it is time-consuming to do so. Thus, developing an automated method of detecting and quantifying BAC may help address these challenges. Several such approaches have been used: Ge et al. 88 proposed an automated classifier that combined a set of image filtering techniques with a k-segments clustering algorithm and showed that the proposed method can detect BAC and identified the calcified vessels.
However, this method cannot detect some common appearances of BAC such as highly curving shape. Cheng et al. 89,90 developed a two-step method using a tracking algorithm to detect the BAC paths, followed by a linking algorithm to connect and extract the generated paths of BACs from mammograms, demonstrating that BAC can be detected, and calcified vessels identified. The authors tested their method with 40 mammograms and achieved performance of 93.8 ± 1.3% for sensitivity and 84.7 ± 3.9% for specificity. However, the proposed method failed to deal with the variation of breast compositions where the distribution of fat and fibroglandular tissues differed in each breast. 41 Nonetheless, precise and automated method for detecting BACs in mammograms continues to be a task worth pursuing particularly if size, shape, and contrast can be taken into account.
DL in medical imaging is a rapidly growing research area used to predict, diagnose, and classify a disease for automated decision making. The application of DL in medical imaging is to assist computers extract features from medical images that may provide useful descriptions and characterizations of the data for a particular medical application. High-level features can be extracted by passing the features of medical images across number layers of the DL model, which are then transformed into useful outputs for this particular medical application.
Several recent studies have investigated the potential of applying DL for assessing BAC from digital mammograms and showed that DL algorithms can achieve or even outperform human experts in identifying BAC from mammograms, which is an encouraging step for predicting this CVD risk factor in women: 38,40,91 Wang et al. 38 proposed a DL model that identified BAC from mammograms at a level comparable to radiology experts but it required high computational cost; AlGhamdi et al. 40 proposed an automated model to detect BACs from mammograms called DU-Net and claimed that their model matched human expert performance; however, BAC was only described as present or absent with no grading presented; Guo et al. 91 developed a lightweight model named (Simple Context U-Net), which requires less computational cost compared with the traditional DL segmentation models, and can be integrated to identify, quantify, and measure the progression of BAC over time in women and showed accurate segmentation of BAC on routine screening mammograms.
However, their model only evaluated data from one institution and a single brand of scanners, which questioned the generalizability of their approach. As a result of the aforementioned limitations, none of these approaches has yet been deployed into clinical practice or validated against clinical outcomes in patients.
BAC Cardiovascular Risk Factors and Other Conditions
BAC cardiovascular risk factors
Several studies have suggested that there is an association between BAC and traditional cardiovascular risk factors, such as diabetes mellitus, hypertension, hypercholesterolemia, chronic kidney disease, and smoking. 11,20,28,92 –94 However, data supporting the association between BAC and some cardiovascular risk factors including hypertension and hypercholesterolemia are inconsistent. 42 To better understand the association between BAC and cardiovascular risk factors, Lee et al. 8 conducted a large meta-analysis of 59 studies and found a positive relation between BAC and diabetes mellitus, hypertension, and hypercholesterolemia with ORs of 2.17 (95% CI 1.82–2.59), 1.80 (95% CI 1.47–2.21), and 1.28 (95% CI 1.06–1.55), respectively.
Furthermore, another independent cardiovascular risk factor is chronic kidney disease (CKD) as women with CKD has higher CVD events compared with women without; 95 Hassan et al. 92 conducted a cross-sectional study and compared women with stage 3 CKD, stage 4 CKD, and ESRD against a control group of women without renal disease, all of which have had screening mammograms. The work found that women with stage 3 CKD, stage 4 CKD, and ESRD had a higher prevalence of BAC compared with the control group with ORs of 1.48 (95% CI 0.43–5.12), 1.99 (95% CI 0.82–4.80), and 1.97 (95% CI 0.98–3.97), respectively.
However, there is an inverse relationship between BAC and smoking, 8,27,42 this is not surprising given that peripheral vascular calcification, which is another form of arterial calcification of the media, is less prevalent among smokers, 4 although the reasons for this inverse relationship are still unknown. 42 One explanation could be that smoking is associated with a higher level of estrogen in postmenopausal women, 96 which is in line with a study from Schnatz et al., 44 where they concluded that women who receive estrogen hormone replacement therapy have lower prevalence of BAC.
BAC and other conditions
Low bone mineral density (BMD) is a condition that often occurs concurrently with CVD/CAD and a shared number of risk factors, including age, hypertension, and smoking. 97 This link between BMD and CVD/CAD has motivated Iribarren et al. 98 to investigate if there is also an association between BAC and BMD. The authors conducted a study on 1,273 postmenopausal women who undertook dual-energy X-ray absorptiometry and screening mammography and found no relationship between the presence and severity of BAC with BMD. There was another study conducted by Nasser et al. 99 that also investigated the relationship between BAC and BMD among 211 postmenopausal women and found no correlation between the presence of BAC and BMD. However, both studies were cross-sectional studies that only focused on women aged 60 years and older. Therefore, prospective studies that include younger women are required to confirm and generalize this finding.
Cognitive impairment is another condition that has also been shown to coexist with CVD/CAD, where patients with known CAD have a 45% increased risk of developing cognitive impairment. 100 Therefore, Iribarren et al. 101 suggested that BAC can be linked with cognitive impairment and dementia. They measured the cognitive function of (3,913) postmenopausal women who also underwent breast screening. After a median follow-up of 5.6 years, their analysis showed that there is no association between the presence and severity of BAC and cognitive impairment or development of all-cause dementia.
The metabolic syndrome is a group of conditions that include insulin resistance, hypertension, excess body fat around the waist, impaired glucose tolerance, and dyslipidemia that usually occur together and increase the risk of CVD. 102 Bae et al. 103 performed a study on 202 women aged 41 and 78 years who underwent a screening mammogram to evaluate the relationship between the presence and severity of BAC and metabolic syndrome and found that the presence and the severity of BAC were associated with an increased risk of metabolic syndrome among women. Another study investigating the association between BAC and metabolic syndrome was conducted by Yildiz et al. 104 and found a positive relationship between BAC and metabolic syndrome.
Other Mammographic Features and CVD
Mammographic images contain additional features, some of which can be important risk factors not only for breast cancer but also for CVD. One such feature is breast density, which describes the amount of glandular tissue and fibrous connective tissue compared with the amount of fatty breast tissue 105 and appears radiopaque on the mammographic examination while the fatty breast tissue appears more radiolucent. 106 It is well known that women with higher breast density have a greater risk of breast cancer; however, a recent study has revealed that women with a higher percentage of fatty tissue in the breast (lower breast density) might have a higher risk of developing CVD with a HR of 3.483 (95% CI 1.476–8.257). 107
Microcalcifications are another feature of mammographic images linked with CVD. These appear as small bright dots on the soft tissue background of the breast with a diameter of less than 1 mm. 108 They can be benign or a sign of malignant breast cancer. Microcalcifications in women are associated with increased age, a family history of breast cancer, and chronic renal failure. 109 –111 In addition to breast cancer implications, Grassmann et al. 108 also found that microcalcifications were associated with increased risk for subsequent cardiometabolic diseases in women with a pre-existing condition of cardiometabolic diseases. Cardiometabolic diseases were defined in this study as CVD, diabetes mellitus, chronic renal failure, and other related conditions.
The authors found that the absolute risk of developing subsequent cardiometabolic disease in women with pre-existing conditions cardiometabolic over 5 years is 57.92% for women with microcalcifications compared with 51.81% for women without. 108 Furthermore, they found that women with cardiometabolic diseases and microcalcifications had a higher risk of cardiometabolic mortality with a HR of 1.79 (95% CI 1.24–2.58) than women with cardiometabolic diseases but without microcalcifications. However, the method used in this study to identify microcalcifications did not distinguish between BAC and microcalcifications and is possible as both were included as microcalcifications. Also, this study did not find any association between microcalcifications and cardiometabolic diseases in asymptomatic women.
Conclusions
Previous research indicates that BAC is strongly correlated with CVD/CAD, hypertension, and diabetes. However, most of these studies are cross-sectional studies with small sample size and are not performed in a primary prevention cohort. Furthermore, the current methods of quantifying BAC and other mammographic features varied across these studies. Therefore, future research should focus more on: evaluating the association between BAC and all future CVD/CAD events for women without established CVD/CAD; stratifying the studies' findings based on different CAD risk factors such as smoking, hypertension, and diabetes mellitus; developing a standardized and automated approach to score or quantify BAC.
Furthermore, most of the existing studies predicting CVD/CAD events from mammographic appearances focus on BAC alone without consideration of other breast characteristics. Thus, future research should also focus on the relationship between CVD and other mammographic features such as breast density and macrocalcifications to confirm if they can also be used alongside BAC for predicting CVD/CAD.
Footnotes
Authors' Contributions
All authors have made equal contributions to this work, including conceptualization, methodology, writing the original draft, reviewing, and editing.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.