
Abstract
Background:
Evidence of post-traumatic stress disorder (PTSD) symptoms related to the COVID-19 pandemic during the perinatal period and the associated risk factors are still limited. Thus, we aimed to investigate the PTSD symptoms associated with the COVID-19 pandemic in a large sample of both pregnant and postpartum women.
Methods:
A cross-sectional study was conducted on 3319 pregnant and up to 6-month postpartum women from Spain. An online survey was completed between June 2020 and January 2021. The assessment included measures of PTSD symptoms associated with COVID-19 (evaluated with 10 questions from the PTSD checklist for Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition), pandemic-related concerns and health background (assessed by the Coronavirus Perinatal Experiences—Impact Survey), and demographic characteristics.
Results:
We found that >40% of women suffered from symptoms of PTSD associated with the COVID-19 pandemic. Difficulty concentrating and irritability were the most common symptoms, showing marked alterations in arousal and reactivity associated with the traumatic event. Being younger, suffering from pandemic concerns and distress, changes due to the pandemic and previous mental health problems were risk factors associated with PTSD symptoms in perinatal women. In addition, whereas being an immigrant (non-Spanish) was a risk factor for pregnant women, having other children and financial problems were risk factors for postpartum women. COVID-19 infection did not appear to be a risk factor for symptoms of PTSD in perinatal women.
Conclusions:
The increased risk of PTSD in pregnant and postpartum women highlights the importance of early detection and treatment of PTSD for pregnant and postnatal women, both during and beyond the pandemic.
Trial Registration:
Introduction
Post-traumatic stress disorder (PTSD) is a significant and poorly recognized mental health problem for women during the perinatal period (from pregnancy to 1-year postpartum). PTSD during the perinatal period can develop after experiencing or witnessing interpersonal violence, natural disasters, or infectious diseases (e.g., Ebola and Zika). 1 Furthermore, PTSD can be caused by a traumatic birth or dissatisfaction with intrapartum care. 2 PTSD includes symptom clusters of intrusion, avoidance, and arousal lasting at least 1 month and leading to clinically relevant distress or functional impairment. A fourth cluster, “negative alterations in cognitions and mood,” has been added to the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5). 3 Numerous studies have shown that both subthreshold and full-blown post-traumatic stress symptoms have a devastating impact on women, partners, and their children. 4 –6
The COVID-19 pandemic represents a threatening and potentially traumatic event, as it can lead to hospitalization and even death in women during pregnancy and postpartum. 7,8 Some previous studies have reported an increase in post-traumatic stress symptoms during the COVID-19 pandemic. 9 –14 The reported rates are highly variable, ranging from 6.1% 10 to 53%. 13 However, previous studies are affected by several limitations. Most studies only included samples of pregnant 9,13,15,16 or postpartum women 11 ; some of these studies were limited by their small sample sizes (N < 300) 9,13,17,18 or were conducted in a single center or a single city 9,13,16,19 ; and only one of them included an assessment of losses and grief due to the pandemic. 20
Furthermore, although having a history of psychiatric disorders, 10,15,16,18 presenting higher levels of COVID-19 health worries and grief, 10 developing COVID-19-related symptoms, 9 having a lower educational level, 9 and being younger 11 have been associated with the presence of higher levels of PTSD symptoms, none of the previous studies analyzed them in both pregnant and postpartum women during the COVID-19 pandemic. To the best of our knowledge, no previous research has investigated PTSD symptoms related to the COVID-19 pandemic and the factors associated with a large sample of pregnant and postpartum women, so the evidence in this field is still limited.
Thus, we aimed to investigate the PTSD symptoms associated with the COVID-19 pandemic in a large sample of both pregnant and postpartum women in Spain. Specifically, the objectives of this study were (1) to assess PTSD symptoms associated with the COVID-19 pandemic; (2) to study the association between PTSD symptoms and demographic, pandemic-related, and health variables; and (3) to identify which factors predict PTSD symptoms in both pregnant and postpartum women.
Methods
Participants and procedure
Participants were part of the international and longitudinal survey “Riseup-PPD-COVID-19” (
The survey was conducted between June 15 and December 31, 2020. Women were recruited through social media advertising (e.g., Twitter), networks of organizations (e.g., universities), policy-makers, local organizations, and other stakeholders. After confirming the inclusion criteria, participants were given informed consent and completed the survey through the project website link (
The Strengthening and Reporting of Observational Studies in Epidemiology guidelines were adopted for reporting. 22 Before the analysis, the survey data were carefully examined for consistency and accuracy. We recruited 3356 eligible women. We removed 37 records because of missing data in the outcome variables. Therefore, this gave a final sample of 3319 women.
Measures
PTSD checklist associated with COVID-19
PTSD symptoms associated with COVID-19 were evaluated with 10 questions from the PTSD checklist for DSM-5 (PCL-5) (namely PTSD-COVID checklist). 23,24 The selection of the 10 questions was part of the Coronavirus Perinatal Experiences—Impact Survey (COPE-IS). 25 The questions were all related to the event of the COVID-19 pandemic (e.g., the extent to which they have experienced repeated disturbing dreams about the COVID-19 outbreak). The subset of questions was selected to reduce the participants' burden and avoid redundancy with other questionnaire items. Each question represents an item of the DSM-5 criteria for PTSD (two items of Cluster B, one of Cluster C, two of Cluster D, and five of Cluster E).
We analyzed two different methods to quantify the PTSD-COVID checklist: (1) Total scores: the sum of the items scored on a Likert scale (from 0, not at all, to 4, extremely). The total scores ranged from 0 to 40. Higher scores meant greater PTSD symptomatology; (2) possible PTSD diagnosis following DSM-5 criteria diagnostic rule; (3) presence of symptoms of PTSD was accepted when the items were rated as “Moderately” or higher (scores >2) in the PTSD-COVID checklist. Clusters B–C and D–E need one and two symptoms to be categorized as possible PTSD, respectively.
The PTSD-COVID checklist's reliability (internal consistency) was good. Cronbach's alpha was 0.88 for the entire sample (95% confidence interval [CI] 0.87–0.88) and both pregnant (95% CI 0.87–0.89) and postpartum (95% CI 0.87–0.89) women. The Kaiser–Meyer–Olkin test (>0.7) and Bartlett's test (p < 0.001) indicated the adequacy of the use of exploratory factor analysis (principal axis factoring and varimax rotation). The one-factor solution was extracted based on parallel analyses. The one-factor solution accounted for 43% of the variance for the entire sample. Similar results were found for pregnant (variance: 43%) and postpartum (variance: 44%) women. For the entire sample and both pregnant and postpartum women, all items reached positive loadings, which varied between 0.25 and 0.78. The items on the PTSD checklist are shown in Table 1.
Characteristics of the Participants and Comparisons Between Pregnant and Postpartum Women
Likert scale ranging from 1 (no concern) to 7 (highly concerned).
Likert scale ranging from 1 (worsened my sleep/energy significantly) to 5 (improved my sleep/energy significantly).
PTSD, post-traumatic stress disorder; SD, standard deviation.
Pandemic-related concerns and health background
The Spanish version of the COPE-IS 25 was administered to assess the women's experiences in the perinatal period during the COVID-19 pandemic. In this study, the variables included were as follows.
COVID-19 exposures and symptoms
(1) Diagnosis and/or symptoms compatible with COVID-19, (2) contact with someone who tested positive for COVID-19, and (3) death of a close person due to COVID-19.
COVID-19-related concerns and distress
(1) Concerns about one's own COVID-19-related symptoms or potential illness, (2) concerns about a child's health as a result of the COVID-19 outbreak, (3) concerns about COVID-19-related symptoms or potential illness in friends and family, (4) distress related to employment and financial impacts due to the COVID-19 outbreak, (5) distress about disruptions of social support due to the COVID-19 outbreak, (6) overall level of impact on daily life due to the COVID-19 outbreak, and (7) overall level of distress about COVID-19. All of the items were rated with a Likert scale ranging from 1 (no concern) to 7 (highly concerned).
Changes due to the COVID-19 outbreak
(1) Changes in sleep and (2) changes in daily energy levels. These items were rated on a Likert scale ranging from 1 (worsened my sleep/energy significantly) to 5 (improved my sleep/energy significantly).
Physical and mental health background
(1) Health complications during pregnancy (e.g., gestational diabetes or hypertension), (2) history of mood and/or anxiety disorder, and (3) current treatment for mental health problems.
Demographic characteristics
Demographics were assessed by a subset of questions about the date of birth, country of origin (Spain vs. others), primigravida/primiparous status, marital status or living with a partner, and educational level.
Statistical analysis
First, an exploratory analysis of the data was performed to detect abnormal values and missing data. Descriptive data analyses were conducted for the total sample and for pregnant and postpartum women. Frequencies and percentages and means and standard deviations (SDs) were calculated for categorical data and continuous variables, respectively.
Differences between pregnant and postpartum women were examined using the chi-squared statistic (between categorical variables) or Student's t-test (when the dependent variable was continuous). In addition, we calculated differences in the total score of the PTSD-COVID (dependent variable) by demographics, pandemic-related, and mental health variables using Pearson's correlation and chi-squared tests. Welch's correction was applied if the data did not meet the assumption of homogeneity of variance. Effect sizes were calculated using Crammer's V and Cohen's d, following interpretation: 0–0.19, negligible; 0.20–0.49, small; 0.50–0.79, medium; 0.80 and over, high. 26
Multiple linear regression analyses were performed to determine how demographics, pandemic-related variables, and health variables were associated with the PTSD symptom scores. Two models were calculated for the pregnant and postpartum subsamples. Following the instructions of Jaccard et al, 27 all of the continuous predictive variables were centered.
All p-values were two-sided and considered significant below 0.05. All CIs were reported at 95%. SPSS version 26.0 statistical software was used to perform all of the analyses.
Results
Descriptive statistics
The characteristics of the participants and comparisons between pregnant and postpartum women are shown in Table 1. The mean age of the participants was 33.6 years. We found higher rates of primiparous/primigravida status (64.20% vs. 59.61%) and primary/secondary education level (23.68% vs. 20.46%) among postpartum women than among pregnant women. Furthermore, postpartum women showed higher rates of health complications during pregnancy than pregnant women (36.36% vs. 26.82%).
Regarding pandemic-related concerns and changes, pregnant women reported more distress about their and their children's health and worsening sleep. However, the results indicated that postpartum women were more concerned about employment and financial impact, daily life impact, and general level of distress. More pregnant than postpartum women reported being under current treatment for mental health problems (5.19% vs. 3.17%). The mean total score for PTSD symptoms was 9.97 (SD = 7.53), and no significant differences were identified between pregnant and postpartum women (Table 1).
Figure 1 shows the percentage of women with moderate symptoms (>2) on the PTSD-COVID questionnaire by DSM-5 cluster. Approximately 40% of pregnant and postpartum women reported difficulty concentrating and irritability. Changes in arousal were the most prevalent PTSD cluster, followed by avoidance and intrusion. A total of 242 women (7.29%) might meet criteria for possible PTSD diagnosis following DSM-5 criteria diagnostic rule.
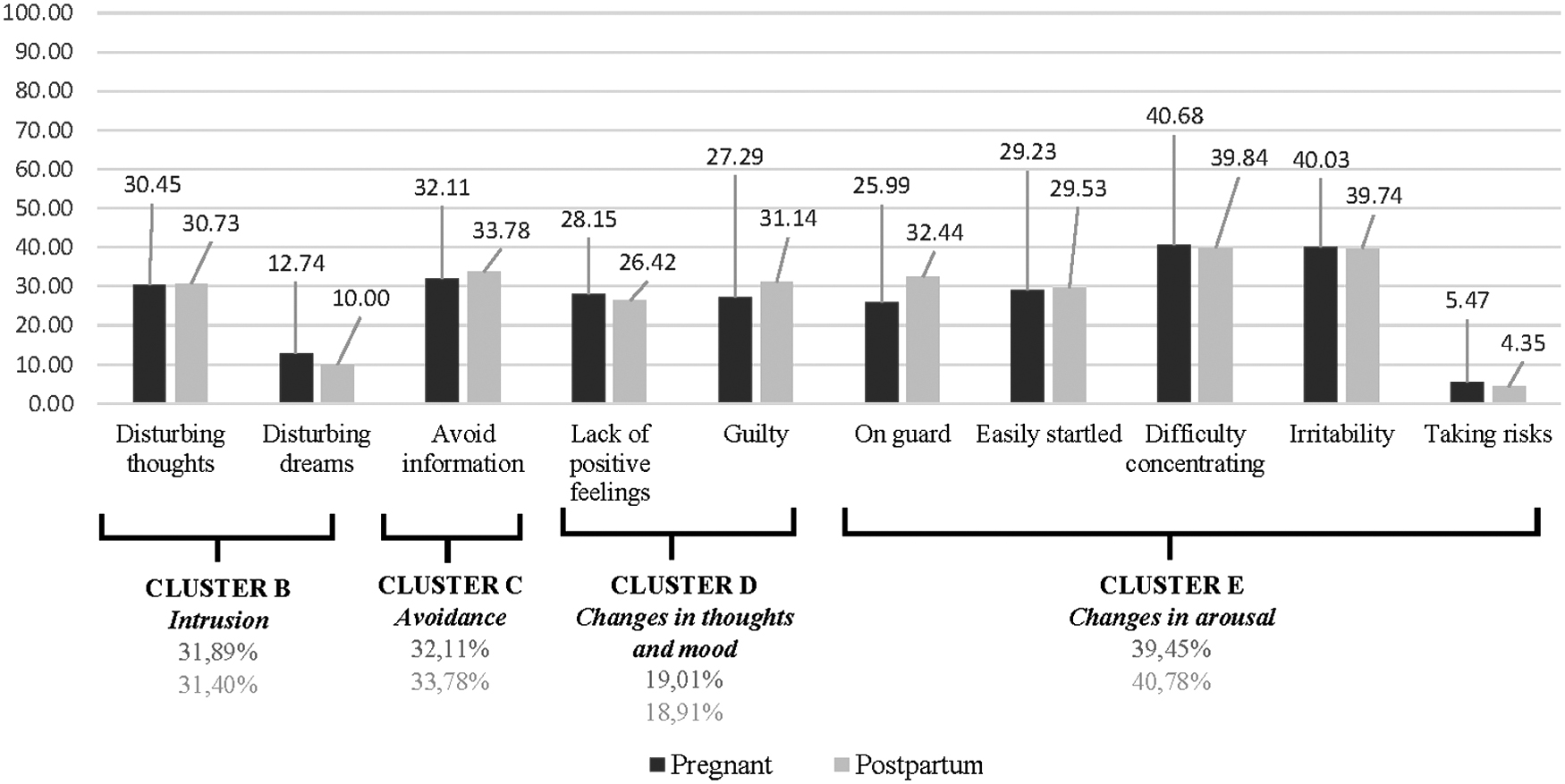
Percentage of pregnant and postpartum women with a moderate score (>2) on each item of the post-traumatic stress disorder-COVID questionnaire by DSM-5 cluster. DSM-5, Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition.
Comparison of PTSD symptoms in pregnant and postpartum women
Table 2 compares the association between the scores of PTSD symptoms and demographic, pandemic-related, and health variables in pregnant and postpartum women. Pregnant and postpartum women with higher scores of PTSD symptoms were younger and had lower educational levels (p < 0.005). However, among pregnant women, higher scores were associated with another country of origin (other than Spain), but in postpartum women, they were higher in women who did not cohabitate with their partner and did not have primiparous status (p < 0.05).
Comparison of Post-Traumatic Stress Disorder Symptoms and Variables of the Study in Pregnant and Postpartum Women
In both pregnant and postpartum women, the death of a close person due to COVID-19 and all concerns, distress, and changes related to the pandemic were positively and significatively correlated with PTSD symptoms (p < 0.001). Furthermore, pregnant and postpartum women with health concerns during pregnancy, a history of mood and/or anxiety disorder, and current treatment for mental health problems had significantly higher scores for PTSD symptoms (p < 0.001). The diagnosis of and/or symptoms of COVID-19 was only associated with higher scores of PTSD symptoms among pregnant women (Table 2).
Factors associated with PTSD symptoms in pregnant and postpartum women
Multiple linear regression models to determine factors for predicting PTSD symptoms in pregnant and postpartum women are presented in Table 3. Both models were significant and provided explained variance rates of 48.7% [F(17; 1335) = 76.633; p < 0.001] and 46.1% [F(17; 1846) = 94.580; p < 0.001] for pregnant and postpartum women, respectively.
Multiple Linear Regression on Prediction of Post-Traumatic Stress Disorder During the COVID-19 Pandemic
Note: Spanish nationality (0 = non-Spanish; 1 = Spanish); educational level (0 = primary or secondary education; 1 = college degree or higher); health complications during pregnancy (0 = no; 1 = yes); diagnosis of and/or symptoms of COVID-19 (0 = no; 1 = yes); death of a close person due to COVID-19 (0 = no; 1 = yes); history of mood and/or anxiety disorder (0 = no; 1 = yes); current treatment for mental health problems (0 = no; 1 = yes); primiparous (0 = no; 1 = yes).
95% CI, 95% confidence interval; LL, lower limit; SE, standard error; UL, upper limit.
The following factors predicted higher PTSD symptoms in both pregnant and postpartum women: being younger, having greater concerns about the disruption of social support, having higher overall levels of stress, having worse sleep and daily energy levels, having a history of mood and/or anxiety disorders, and being under treatment for mental health problems. Being non-Spanish was a risk factor for PTSD among pregnant women, whereas being nonprimiparous and having higher concerns about a child's health and the financial impact due to COVID-19 were risk factors for PTSD symptoms among postpartum women (Table 3).
Discussion
Main findings
In this large sample of 3319 pregnant and postpartum women, we found that >40% of the women suffered from symptoms of PTSD associated with the COVID-19 pandemic. Difficulty concentrating and irritability were the most common symptoms, showing marked alterations in arousal and reactivity associated with the traumatic event. Being younger, suffering from pandemic concerns and distress, and experiencing changes due to the pandemic and previous mental health problems were risk factors associated with PTSD symptoms in perinatal women. In addition, whereas being an immigrant (non-Spanish) was a risk factor for pregnant women, having other children and financial problems were risk factors for postpartum women. COVID-19 infection did not appear to be a risk factor for symptoms of PTSD in perinatal women.
Strengths and limitations
This is the first study conducted in a large sample that compares the results of pregnant and postpartum women and identifies the most critical risk factors for each type of population.
Despite the large sample size, the findings must be interpreted with caution. First, the academic level of the participants was higher than expected. 28 Women with lower educational levels may have less access to technology and are likely to be underrepresented in the sample, given that data collection occurred using an online survey. Second, this is an observational cross-sectional study design, which restricts causal inference. However, it allowed us to compare many different variables simultaneously to identify the risk factors for PTSD symptoms associated with the COVID-19 pandemic among pregnant and postpartum women. Third, a formal diagnosis of PTSD cannot be made based on just the administration of a subset of questions from the PCL-5 questionnaire focused only on the COVID-19 pandemic. This questionnaire has been previously used for investigating PTSD during the pandemic 29 and its psychometric properties in our sample are good.
Comparison with previous research
More than 40% of the women in our sample experienced PTSD symptoms associated with the COVID-19 pandemic. These observations are consistent with previous studies suggesting the presence of PTSD symptomatology between 43% and 53% of the population during the pandemic. 9,11,13 Furthermore, 7.29% of them might meet criteria for possible PTSD diagnosis following DSM-5 criteria diagnostic rule. These rates represent a large increase compared with previous studies conducted in Spain. Previous evidence showed that about 1.5% of pregnant women 30 and about 1% of postpartum women 31 suffered PTSD during the perinatal period.
Difficulty in concentrating and irritability were the most prevalent symptoms. Alterations in arousal showed that pregnant and postpartum women were more overly alert. The specificity of the findings in the clinical sample corroborates the clinical importance of altered regulation of fear-enhanced startle in response to the COVID pandemic. 32
Kinser et al 29 analyzed the concerns and coping strategies associated with PTSD symptoms in perinatal women during COVID-19 pandemic. They found that increased time on social media, helping others, and using a meditation/mindfulness practice were risk factors for PTSD for perinatal women, but instead higher resilience scores, getting a good night's sleep, and decreasing time watching the news were protective factors of PTSD symptoms.
However, one of this study's key findings was identifying specific sociodemographic, mental health, and COVID-19-related predictors of PTSD for pregnant and postpartum women. We found that being younger, suffering from pandemic concerns and distress, experiencing changes due to the pandemic, and suffering from previous mental health problems were shared predictors of PTSD for both pregnant and postpartum women, confirming the findings of previous studies. 10,15,18 PTSD symptoms are associated with depression and anxiety, suggesting the comorbidity of perinatal mental health problems during the pandemic. 29
There were differences between pregnant and postpartum samples in specific risk factors. Immigration was a unique risk factor for pregnant women. 33 Immigrant populations could differ in profile from native women in Spain; differences in sociodemographic variables (e.g., married) and a higher prevalence of mental health problems can explain the higher vulnerability of immigrant women to PTSD during pregnancy. 33 This finding stresses the need to study the experiences of pregnant immigrants who suffer from PTSD.
Finally, having other children and financial problems places postpartum women in a vulnerable situation to experience PTSD. 20 This may be a result of pandemic-related stressors. Women during the postpartum period are probably experiencing concerns about the child's health (e.g., fear of transmitting the virus to the baby), lack of support for caring for their other children, and uncertainty about the future. 34
Conclusions
PTSD symptoms were common in perinatal women during the COVID-19 pandemic. PTSD symptoms were associated with factors specifically related to the COVID-19 pandemic. Immigrant status was a unique risk factor for pregnant women, whereas having other children and financial problems were risk factors for postpartum women. Future studies should follow the course of PTSD over time. Given the negative impact of PTSD symptoms during the perinatal period on the entire family system, early detection and treatment of PTSD are warranted.
Footnotes
Acknowledgments
The authors would like to thank all women who participated in the survey.
Authors' Contributions
E.M. is the principal investigator of the study from which the data for this analysis are drawn. E.M. and S.D.S. were involved in the recruitment of participants for the survey. E.M. conceived the research question, and E.M. and S.D.S. designed the study analysis plan. All authors approved the data analysis plan. S.D.S., C.R.D., and I.G.G. conducted the data analyses. E.M. and T.G.L. wrote the first draft of the article. All authors critically revised this draft and approved the final version.
Author Disclosure Statement
The authors declare no conflicts of interest.
Funding Information
The project is part of the COST Action Riseup-PPD CA 18138 and was supported by COST under COST Action Riseup-PPD CA18138.