
Abstract
Background:
The ability to accurately recall specific reproductive health events is an integral aspect of medical decision making and evaluating a female's overall health and wellness across their lifespan. The Health and Reproductive Survey (HeRS) was developed to recall reproductive events and environmental influences on reproductive characteristics throughout the lifespan of a female. This study aimed to determine how reliably women recall certain events during menarche and early reproductive years. It was hypothesized that age at menarche, hormonal contraceptive use, and physical activity would be recalled reliably among all age ranges, while the recall reliability for cycle regularity and length would be more inconsistent with advancing age.
Materials and Methods:
A total of 144 participants (age: 32.73 ± 11.92), completed the HeRS on two occasions spaced 4 months apart to investigate recall reliability. Cohen's kappa coefficient was used to assess the consistency of categorical responses and 95% limits of agreement were used for continuous data.
Results:
Although physical activity changes had greater variability than anticipated (0.79), the recall reliability among the youngest (1) and oldest (0.89) age groups was high, and females were able to consistently recall the age of menarche (0.83), physical activity level (0.9), cessation of period during early reproductive years (0.91), and birth control use following menarche (0.85) and during the early reproductive years (0.9).
Conclusions:
The HeRS is a useful tool for reliably recalling reproductive history and physical activity participation across multiple age ranges and can be utilized to gather crucial information throughout the reproductive lifespan.
Introduction
To thoroughly understand longitudinal health outcomes, it is imperative that individuals recall important health data throughout the lifespan with reasonable reliability. Although the gold standard method for assessing recall data in medical environments involves comparing responses with medical records, 1 it is not always possible to obtain these for every reproductive-related concern that transpires across a woman's reproductive lifespan. As such, the ability of an individual to recall specific health events throughout their lifespan allows for a more well-informed approach to medical decision making. Matteson articulated the importance of patient-reported outcome measures by assessing the impact of illness and symptomatology among women with reproductive-related health issues. 2 However, the reliability of recall data and the retention of memory about specific medical events largely relies on the subject matter being recalled. 1
The recall of a salient event, such as the onset of menarche, has been extensively studied and shown to have high recall reliability when compared with medical records or status quo interviews. 3,4 Moreover, when instructed to recall age at menarche about 4 years postmenarche, 63% of errors made by respondents were less than 3 months off at recall, 5 and when recall was about 39 years following the event, about 50% of the errors made by respondents were less than 6 months from the actual value. 4 Thus, the ability to recall the age at menarche appears to be relatively stable many years following the actual event. It would be extremely useful for women to reliably recall other menstrual cycle-related history or circumstances surrounding critical reproductive-related health events since it may provide crucial preliminary insight regarding current or potentially long-term health consequences. Yet, it is unclear how reliably women recall these reproductive events (i.e., missed menstrual cycles, contraceptive use) or the circumstances surrounding these events (i.e., changes in physical activity patterns).
Other reproductive-related events (i.e., history of pregnancy or breastfeeding) also have a high rate of recall when compared with medical records due to the saliency of such events. 6 –8 Yet, complications that transpire throughout a reproductive lifespan could be attributed to menstrual-related disorders, such as primary or secondary amenorrhea, irregular menstrual cycles, underlying health issues, or environmental factors (i.e., physical activity status) that may cause variability in menstrual cycle length and regularity. Previously, recall reliability of menstrual cycle length and regularity was observed as age and regularity dependent, with greater accuracy in recall among younger respondents compared to older respondents, and among those with more regular cycles. 9,10 Nonetheless, the ability to consistently recall hormonal contraceptive use, age of menarche, menstrual regularity and length, and physical activity status across the early reproductive years has yet to be established. Linking reproductive history to physical activity or lifestyle factors associated with given time frames throughout a lifespan could greatly improve the recall accuracy of these constructs. 11
A regular menstrual pattern typically indicates a properly functioning endocrine system, however, the menstrual cycle is highly susceptible to volume and pattern changes on a regular basis, which is largely due to hormonal and environmental factors (e.g., physical activity). 12 Variations in environmental or other factors (i.e., dieting, stress) could promote irregular menstrual cycles, characterized by longer or shorter bleeding patterns, an absence of bleeding for months at a time, or inconsistent month-to-month bleeding. Irregular menstrual cycles throughout adolescence and/or adulthood can result in a greater risk of premature mortality and chronic disease. 13 –16 The amount of significant behavioral and/or environmental perturbations to the normative pattern of the menstrual cycle may provide clinically relevant information for lifespan health and wellness. Thus, it is important to identify if women can reliably recall information beyond the more salient reproductive events.
To address these gaps in the literature, Duffy et al. (2021) established the Health and Reproductive Survey (HeRS), which accounts for menstrual onset and early reproductive history related to menstrual cycle length and regularity, hormonal contraceptive use, and physical activity status across different life stages. 17 This survey was developed to identify recall ability of less salient reproductive history events, such as menstrual history regularity and environmental influences, on these characteristics throughout a female's reproductive lifespan. Recalling such information is imperative for proper diagnoses of primary or secondary amenorrhea, infertility-related conditions, and long-term reproductive disorders. This survey is designed to gather crucial knowledge on menstrual cycle regularity and contraceptive use throughout the reproductive lifespan and determine how reliably females can recall this information.
The purpose of this study is to determine how reliably women recall events during menarche and their early reproductive years, including menstrual onset, cycle length and regularity, hormonal contraceptive use, and physical activity status using the HeRS survey at two time points separated by 4 months. Furthermore, the accuracy of recall between women stratified by their age at the time they completed the survey was compared. It was hypothesized that questions regarding age of menarche, hormonal contraceptive use, and physical activity during menarche and the early reproductive years would be recalled reliably among all age ranges. We also hypothesized that recall reliability for questions regarding menstrual characteristics, such as menstrual cycle regularity and length, both postmenarche and during the early reproductive years, would be more inconsistent across all age ranges due to the interindividual variation of these characteristics and the environmental context of the experiences.
Materials and Methods
Experimental design
This study used a retrospective self-reported online survey in a test–retest design across a 4-month time span to investigate recall reliability from the HeRS survey. HeRS was designed to capture reproductive and health history, as well as physical activity experience, across varying stages within the lifespan. 17 The survey was separated into sections to reflect this: (1) Menarche, (2) Early Reproductive Years (ages 13–18), (3) Mid Reproductive Years (ages 18–24), (4) Late Reproductive Years (ages 25–40), and (5) Advanced Reproductive Age (ages 40+). Based on their age at the time respondents completed the survey, they filled out each section up to and including the section that included their current age (e.g., if a 25-year-old participated, they would fill out sections 1–4). For this study, only survey sections 1 and 2 of the original survey 17 (i.e., menarche and early reproductive years) were included in the analyses to best address the aims of the current study (Supplementary Data). Participants were not compensated for completing the survey. Institutional Review Board approval was sought and granted exempt status by the University of North Carolina, Greensboro (IRB No. 19-0378).
Subject characteristics
The survey was available to all women at or above the age of 18. The survey is designed to be completed within 12–15 minutes for native English speakers, with at least a third-grade literacy rate in the United States.
Testing procedures
The HeRS was first opened on August 9, 2020. Recruitment emails with a link to the HeRS were sent to a convenience sample of groups, organizations, and individual contacts believed to have broad access to women within the University setting (i.e., coaches, athletes, medical students, business students, etc.). However, community members were also potential participants since the recruitment email included a request to forward the survey to any other women that may be inclined to participate. Reminders were administered 1 week later to all those who opened the link but did not complete the survey. The survey was closed on September 1, 2020.
The survey was opened again on December 1, 2020, and emails were distributed to all those who participated in the previous round. Those who did not fill out the survey immediately were sent reminder emails 1, 2, and 3 weeks following. The survey was closed on January 1, 2021.
Statistical analyses
All descriptive data analyzed in the study were presented as mean ± standard deviation. An a priori statistical significance was set at p < 0.05. HeRS questions included for analysis provided valuable information about reproductive health recall at menarche and during the early reproductive years following menarche. The specific questions of interest can be found in Tables 1 and 2. Respondents were grouped into one of four age ranges based on current age at the time of survey completion: 18–24, 25–29, 30–39, and 40+. Comparison between Time point 1 (T1) and Time point 2 (T4mo) was used to determine test–retest recall reliability. Depending on the question type, analyses were completed as a Cohen's kappa (Kappa) coefficient or as a 95% limit of agreement (LOA). Cohen's kappa was used for all yes/no and categorical questions, which took into account the probability of respondents answering the same way at each time point by chance. Limits of agreement were used on all questions of value (i.e., questions with number ranges) to determine how reliable responses were between T1 and T4mo by subtracting T4mo from T1 for all continuous variables.
Recall Reliability of Menarche-Related Survey Questions Across Age Groups
Recall Reliability of Early Reproductive Age-Related Survey Questions Across Age Groups
Kappa analyses were completed according to the following cut points: 0 = agreement equivalent to chance; 0.1–0.2 = slight agreement; 0.21–0.40 = fair agreement; 0.41–0.60 = moderate agreement; 0.61–0.80 = substantial agreement; 0.81–0.99 = near-perfect agreement; and 1 = perfect agreement.
Results
Subject characteristics
A total of 308 respondents completed the survey during the initial recruitment period (T1), with a total of 144 respondents (47.75%) fully participating in all aspects of the study by completing the HeRS at both time points (the initial survey [T1] and 4 months later [T4mo]). The average age of the respondents was 32.73 ± 11.92. The frequency of HeRS respondents by current age, reported at T4mo can be found in the frequency histogram (Fig. 1).
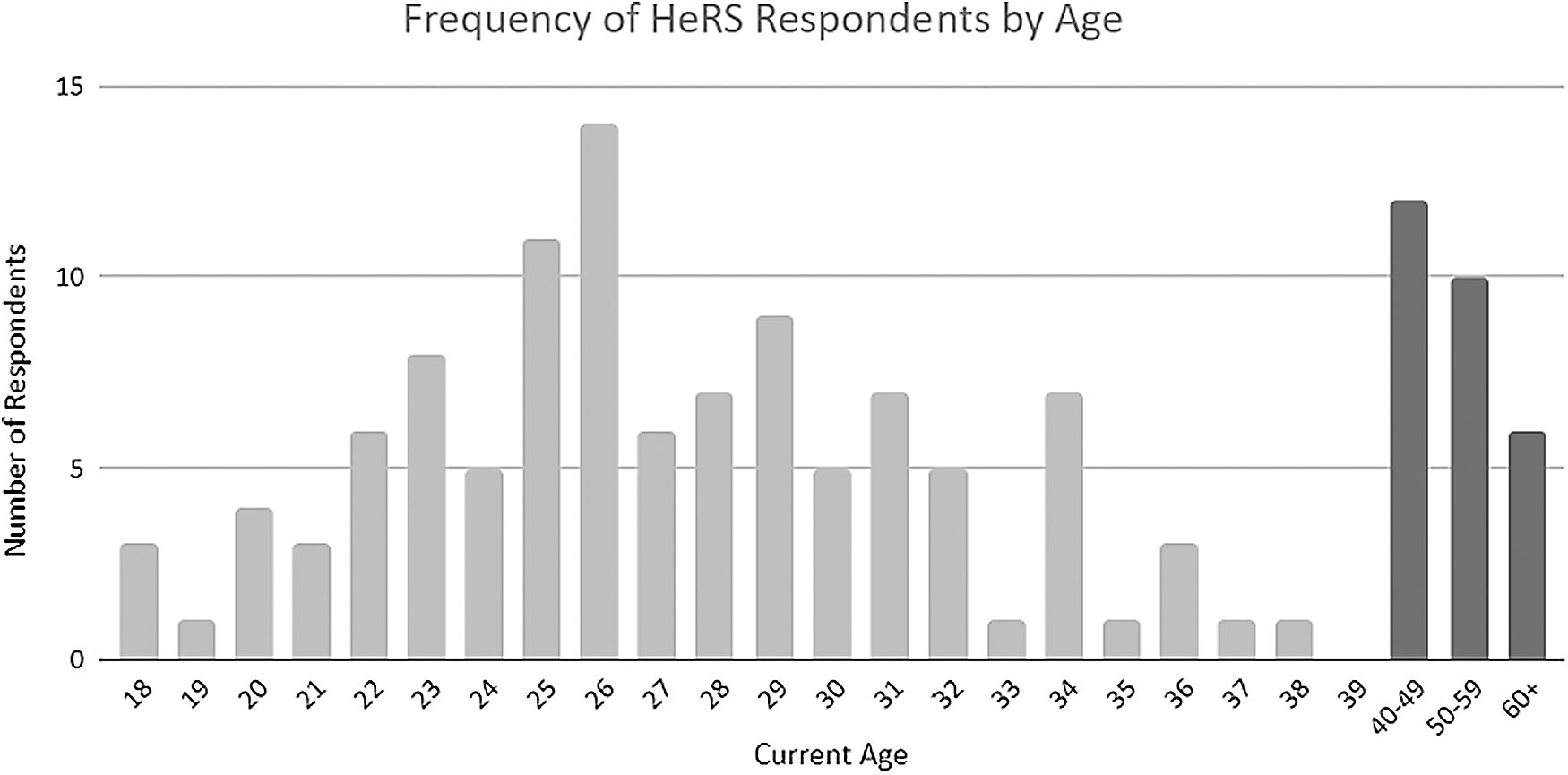
Frequency of HeRS respondents by current age reported at T4mo. HeRS, Health and Reproductive Survey.
Age of menarche recall
When asked to recall age at menarche, all age groups had either perfect (30–39), near-perfect (18–24, 40+), or substantial (25–29) agreements (see Table 1).
Hormonal contraceptive use recall
When asked to recall hormonal contraceptive use following menarche, the three oldest age groups had near-perfect agreement, while the youngest age group had substantial agreement (see Table 1). Yet, when asked to recall the use of hormonal contraceptives during early reproductive years, the three youngest age groups had near-perfect agreement, while the oldest age group had substantial agreement (see Table 2). When asked to recall the type of hormonal contraceptive used, the oldest age group had moderate agreement, while the youngest age group had fair agreement (see Table 2).
Physical activity status recall
When asked to recall physical activity level at the time of menarche, the youngest and oldest age groups had perfect agreement, with high agreement among the remaining groups. However, when asked to recall the average amount of physical activity hours performed per week around the time of menarche, recall reliability was low among all groups—with the highest agreement being moderate among the 30–39 age group (see Table 1). On the other hand, when asked if menstrual cycle changes occurred during early reproductive years due to sport or physical activity participation, the youngest age group had perfect agreement, followed by the oldest age group with near-perfect agreement (see Table 2).
Cycle length recall
When asked to recall first period cycle length, the oldest age group surprisingly recalled this information nearly perfectly, followed by the two youngest groups with moderate agreement (see Table 1) When respondents were asked to recall the average number of periods per year during the early reproductive years, the 25–29 age group had substantial agreement, however, when asked to input the average number of periods per year, in 68% and 95% of the participants who answered this question (n = 130), their recall was within 0.04 ± 0.78 and 1.5 years, respectively (see Table 2).
Cycle regularity recall
When asked to recall the timing of their second period in relation to their first period, the 25–29 and 40+ age groups had moderate agreement, yet, when asked to recall regularity following their second period, the youngest age group had substantial agreement (see Table 1). When asked to recall period cessation for 2 or more months during the early reproductive years, the youngest and oldest age groups had perfect agreement, while the remaining groups had near-perfect or substantial agreement, and when asked to recall age of period cessation, the youngest age groups had substantial agreement. In 95% of the cases, those who answered this question (n = 43) had a recall reliability within 0 ± 0.85 and 1.7 years, respectively. Lastly, when asked to recall the longest length of time without a period, the LOA varied greatly compared with the other continuous variables analyzed in this data set (−1.455 ± 6.704), indicating both large systematic and random error in recall among the 44 participants who answered this survey question (see Table 2).
Discussion
The purpose of this study was to establish how reliably women of varying age groups recall specific incidences during menarche and their early reproductive years, including menstrual onset, cycle length and regularity, hormonal contraceptive use, and physical activity status. We hypothesized that age of menarche, hormonal contraceptive use, and physical activity status during menarche and the early reproductive years would be recalled reliably among all age ranges, while cycle regularity and length following menarche and throughout the early reproductive years would have high variability among all age groups due to interindividual differences in menstrual history. Our findings related to the primary hypotheses aligned with findings from previous studies. The notable exception was the recall of physical activity changes in relation to menstruation during the early reproductive years, which displayed more variability than expected. Additionally, our secondary hypotheses were almost perfectly aligned with our findings, with some variability observed among the recall of cycle length and regularity during both menarche and the early reproductive years.
Similar to previous studies, 3 –5,9,18 the recalled age at menarche had either perfect, near-perfect, or substantial agreements for all age groups. Specifically, Bergsten-Brucefors compared the actual age at menarche at the time of occurrence versus being asked 4 years later and found high recall reliability (0.81), with most errors being less than 3 months apart (63%). 5 Meanwhile, Damon and Bajema observed a substantial recall reliability (0.61), with half of the errors being less than 6 months from the true date (50%) when women were asked to recall the age at menarche 39 years later. 4 This is remarkable given the extensive time lapse between the event and the recall. Although we were not able to ascertain the accuracy of the recall compared with the actual timing of menarche in our study, most of the age groups reliably recalled the age at menarche at the two time points separated by 4 months, which supports our inference regarding accuracy. It should be noted that in the current study, the classification of age of menarche utilized categorical groups (i.e., <11, 12–15, 16+).
Due to this aspect of the survey, as well as the short length of time between time points, respondents were responsible for identifying the correct categorical value and accurately doing so at both time points. Although this categorical metric is less specific, it is helpful in reducing the likelihood of error when asked the same question multiple times.
As hypothesized, recall reliability of hormonal contraceptive use during menarche revealed near-perfect agreement among all but the youngest age group (0.75). Similarly, when this question was asked during the early reproductive years, near-perfect agreement was achieved for all groups except the oldest age group (0.80). Yet, when asked to recall the form of hormonal contraception used, reliability was low among all age groups. Interestingly, 86.11% (n = 144) reported the use of some form of hormonal contraceptive during their lifetime, which aligns with previous reports of hormonal contraceptive use in women ages 15–44, 82% of which reported the use of a hormonal contraceptive pill at least once in their life. 19 The high recall reliability of hormonal contraceptive use across a female's lifespan likely reflects multiple aspects of contraceptive use, including the effort one must go to obtain and continue an active prescription, personal reasons behind using it, and side effects that may be prevalent at the start or throughout the use of the prescription. 20
However, the form of hormonal contraceptive was not reliably recalled by any age group, which is likely due to numerous stop/start patterns (i.e., for pregnancy, during lactation, lack of need for birth control during certain times, presence of side effects, switching birth control options) that many women undergo in their lifespan. Regarding side effects, Wigginton et al. observed that 258 women experienced irregular bleeding, weight changes, libido changes, skin-related issues, or headaches, which acted as a precursor to changing contraception types. 20 To our knowledge, this is the first study to demonstrate the recall reliability of hormonal contraceptive use and form over a short duration of time. Yet, no existing studies have considered the recall reliability of hormonal contraceptive use over long-term periods of time.
Similarly, recall reliability of physical activity status following menarche was relatively high among all age groups, displaying perfect agreement among the youngest and oldest age groups for physical activity status recall at menarche. Yet, recall reliability of the hours spent participating in physical activity was not as accurate, a common issue noted when asking individuals to recall their physical activity. Previous research established validity with test–retest reliability and long-term recall reliability for physical activity recall. 21 –23 Specifically, Brown et al. examined test–retest reliability in population samples for four self-report physical activity questionnaires, all of which concluded to have high test–retest reliability for assessing activity status and sedentariness, but had only moderate reliability for assessing total minutes of activity. 22 Blair et al. analyzed long-term recall reliability of physical activity 1–10 years after examination and observed an average of 60%–75% agreement in recall. Additionally, these researchers found that intensity of activity influenced recall reliability, with more accuracy recalling vigorous activity than less-intensive activities. 21
Falkner et al. investigated the quality of physical activity recall over 30 years and found females to have higher levels of reliability in more categories than males. 23 Thus, test–retest reliability and long-term recall reliability of physical activity status were deemed highly reliable, but the actual amount (e.g., in hours or minutes) is not as reliably recalled and these findings align with previous work on physical activity recall, although not specifically related to reproductive health, among the youngest and oldest age groups in the current study. Comparatively, recall of menstrual cycle changes due to physical activity participation during the early reproductive years was highest among the youngest and oldest age groups. This general idea was previously observed by Davis et al. (2015), with younger adults more accurately recalling details of certain events, while older adults more accurately recalled when the events occurred (along with minor details regarding the events), which could explain why certain categorical survey questions were most accurately recalled by these two age groups. 24
In terms of data recall reliability, Dex observed that the accuracy of memory retention largely depends on the subject matter being recalled, with higher accuracy in the recall of more traumatic or salient events when compared with less significant events. 1 Specifically, when considering menstrual cycle length and regularity over certain periods of time, the recall reliability of this information is most likely dependent on the disruptiveness, or lack thereof, of the events being recalled. For example, the onset of menarche is a memorable event that has been accurately recalled over a short or long period of time, as displayed in the current study and previous literature. Questions regarding menstrual cycle length and regularity following menarche and during the early reproductive years revealed that age at survey completion appeared to play a minimal role in recall reliability between time points. Recall reliability of menstrual cycle regularity and length during the early reproductive years had better agreement than regularity and length following menarche among all age groups.
Also, recall reliability of menstrual cycle cessation during the early reproductive year accurately recalled among all age groups. Recall reliability of menstrual patterns 18 and cycle length 10 during the early reproductive years was similar to previous studies, displaying moderate-to-substantial agreements. Consequently, recall reliability of menstrual pattern and length tends to be largely reflective of individual experience. Whether a woman consistently experienced periods with great regularity or irregularity, deviations from their norm would be more likely to be recalled. Thus, if a menstrual cycle rarely ceased and was adequately regular throughout a lifespan, a lack of menses for 2 or more months would be suggestive of a memorable experience. Additionally, if consciousness of reproductivity or fertility efforts are heightened, absence of menses would also be memorable in this instance. In contrast, females with highly irregular cycles may have a difficult time recalling missing cycles or number of cycles per year.
In summary, our hypotheses were almost completely in line with the data, with the exception of physical activity changes due to menstruation during the early reproductive years having more variability than expected. Yet, physical activity recall reliability was highest among the youngest and oldest age groups, which was consistent in both survey sections of interest. Ultimately, this study provides many strengths—specifically in adding value to menstrual cycle history recall reliability research. Importantly, this study paired menstrual cycle history recall with physical activity status and hormonal contraceptive use, which has not yet been accomplished in prior retrospective surveys. Additionally, this is the first study to determine recall reliability of hormonal contraceptive use, which can be extremely useful to consider alongside other menstrual cycle history variables in understanding the trajectory of women's reproductive health throughout their lifespan. However, this study has some limitations as well.
Although 4 months is a reasonable time period between survey time points, asking respondents to complete this questionnaire twice without receiving results or feedback on previous responses could have caused them to believe that their input did not matter as much as they originally considered, 25 thereby deeming the accuracy of recall to be highly subjective. Additionally, the length of the HeRS survey could be deemed as a strength, however, the redundancy of survey questions may have caused survey fatigue in the respondents, as previous research deemed to be potentially problematic and may decrease accuracy in responses as an end result. 25 Moreover, because respondents' answers could not be compared with medical records or to a measure of status quo, room for potential error is apparent as a result of the lack of validity in answering the survey questions initially. 1 Although snowball sampling was executed, the convenience sample consisted largely of coaches, athletes, and students, which is only a small percentage of the female population.
Thus, this creates a limitation in terms of generalizing these findings to the entire general population. Similarly, because of the sampling pool, our study had a limited number of postmenopausal women. Therefore, the findings of the current study are most applicable to those similar to our convenience sample. In summary, the high recall reliability regarding age of menarche and hormonal contraceptive use in all age groups, as well as physical activity in the youngest and oldest populations, provide the current literature with novel findings for contraceptive recall reliability and additional evidence to support previous findings of recall reliability of age of menarche and physical activity status. Similarly, the variability regarding cycle length and regularity among all age groups provides additional evidence in support of previous findings, as these characteristics are based largely on interindividual experiences.
Footnotes
Acknowledgment
The authors would like to thank all participants who took the time to complete this survey.
Authors' Contributions
R.M.C. wrote, created the tables, completed data analytics, and provided conceptual contributions to the article. H.M.G. structured the design of the study, completed primary data analytics, created the histogram figure, and made significant contributions to the article. S.J.S., J.M.D., L.W., and D.M.D. contributed to revising the article, conceptual contributions, and final approval before publishing. D.M.D. also created the survey utilized within this article.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.
Supplementary Material
Supplementary Data
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.