
Abstract
Background:
Separate lines of research have linked hypertension and alcohol use disorder to cognition among adults. Despite known sex differences in both of these conditions, studies examining associations on cognition are limited. We aimed to determine whether hypertension impacts the relationship between alcohol use and everyday subjective cognition and whether sex moderates this relationship in middle-aged and older adults.
Materials and Methods:
Participants (N = 275) 50+ years of age, who reported drinking, completed surveys measuring alcohol use (Alcohol Use Disorder Identification Test consumption items), self-reported history of hypertension, and everyday subjective cognition (Cognitive Failures Questionnaire [CFQ]). Regression was used to test a moderated moderation model examining independent and interactive roles of alcohol use, hypertension, and sex on cognition (CFQ scores: total, memory, distractibility, blunders, and names). Analyses controlled for age, years of education, race, body mass index, smoking status, depressive symptoms, global subjective sleep quality, number of prescription medication used, and number of comorbid medical conditions.
Results:
Sex moderated the interactive associations of hypertension and alcohol use frequency on CFQ-distractibility. Specifically, in women with hypertension, more alcohol use was associated with greater CFQ-distractibility (B = 0.96, SE = 0.34, p = 0.005).
Discussion
: Sex moderates the interactive association of hypertension and alcohol use on some aspects of subjective cognition in mid-to-late life. In women with hypertension, alcohol use may exacerbate problems with attentional control. Further exploration of sex- and or gender-specific mechanisms underlying these is warranted.
Introduction
Cognitive decline has been linked with both alcohol consumption 1 and hypertension, 2 –4 defined as chronic elevation of systemic atrial pressure. 3 Despite sex differences in the prevalence of both cognitive impairment 5 and hypertension 6,7 in aging populations, research to date has not examined sex differences in the relationship between alcohol use, hypertension, and cognition. Understanding these interactive relationships will facilitate precision medicine approaches to cognitive aging by identifying potential targets for treatment before cognitive decline.
The prevalence of hypertension in middle-aged and older adults ranges from 32% to 70%. 8,9 Across the lifespan, hypertension is more common in men than women. 6 However, older women (75+ years of age) are more likely to have hypertension than older men. 10 Findings regarding the link between hypertension and cognition are inconsistent. For instance, hypertension has been proposed as a risk factor for neurocognitive disorders, 2,11,12 specifically for mild cognitive impairment (MCI) 11 and Alzheimer's disease and related pathology. 13,14 In objective tests of cognitive functioning, hypertension in older adults has been linked with worse global cognition, executive function, 15 –17 memory, 15 attention, and processing speed. 16 In contrast, other studies indicate no association between hypertension and cognitive function. 18,19 Cardiovascular diseases are also associated with subjective cognitive failures, 20 and hypertensive older adults experience greater subjective memory complaints. 21 These complaints are linked with worse global cognition 21,22 and memory performance. 20
Research testing sex differences in the relationship between hypertension and cognition is limited. 11 Given sex differences in both cognitive impairment 5 and hypertension, 23 sex may be one factor confounding associations between hypertension and cognition in studies to date. Of the few studies that have been conducted, women with hypertension experience worse objective cognition 24 and a higher risk for dementia 25 compared to men.
Alcohol use is the most commonly used psychoactive substance in aging populations 26,27 and is linked to an increased risk of cardiovascular diseases, disability, and mortality. 28,29 However, findings regarding alcohol use and cognition are also inconsistent. 1 Some studies in aging adults report links between alcohol use and greater objective cognitive deficits (attention, learning, memory, motor function, executive function, and global cognition), 30 as well as worse overall subjective cognitive function (i.e., greater cognitive complaints). 31 –33 Other work has shown no association between alcohol use and a range of cognitive functions (attention, semantic fluency, verbal memory, and global cognition) among middle-aged adults, 34 and some findings suggest long-term alcohol use does not impact cognitive decline during aging. 35
Sex differences in the link between alcohol use and cognitive function in aging adults have been reported, but these are also inconsistent. Some studies suggest that, relative to women, men in mid-to-late life experience greater deficits in visuospatial ability 36 and overall cognitive impairment, 37 and faster cognitive decline with greater alcohol use. 38,39 Other studies in middle-aged and older men have found either no association between alcohol use and objective cognition 40 or a positive association between higher drinking levels and cognitive abilities (attention, verbal memory, and global cognition). 41 For women in these age groups, most studies link moderate alcohol use to better global cognition, 37,40,41 executive function, attention, 40,41 and verbal memory. 36,40,41 Studies regarding sex-specific patterns of alcohol use and subjective cognition in aging adults are limited. However, those that exist link alcohol use to more subjective cognitive complaints in men relative to women. 42,43
Despite independent lines of research linking alcohol use and hypertension to cognition, interactive relationships remain relatively unexplored. Hypertension and alcohol use have also been associated, 7,44 although the pattern and strength of associations vary across studies. Some findings have shown a linear relationship between alcohol use and cardiovascular risk. 45 Other findings suggest a J-shape relationship, such that light-to-moderate alcohol use may provide cardiovascular protection, while heavy alcohol use increases cardiovascular risk. 46,47 There is some evidence that this curvilinear relationship is sex specific, in that it is more evident in women compared to men. 46 Thus, investigating how alcohol use and presence of hypertension may interact in their relationship with cognition in sex-specific manner is warranted.
This study tested hypertension as a moderator of the association between self-reported alcohol use and subjective cognition, and evaluated whether sex further moderates this relationship in middle-aged and older adults. We hypothesized that greater alcohol use would be associated with worse subjective cognition (worse ratings of everyday cognition) and that this relationship would be strongest in those with hypertension compared to those without hypertension. We also expected that sex would moderate these interactive associations. However, given inconsistent findings regarding the sex-specific impact of hypertension and alcohol on cognition, we did not have explicit hypotheses regarding which sex would show the strongest associations.
Materials and Methods
Participants
Participants were recruited through Qualtrics market research panels. Qualtrics research panels use digital fingerprinting technology with IP address checks to ensure the validity and reliability of data collected. Participants provided informed consent before completing survey measures. Inclusion criteria were as follows: (1) 50 years of age or older, (2) currently residing in the United States, (3) no neurological disorder or cognitive impairment (e.g., MCI, Parkinson's Disease, dementia, Amyotrophic Lateral Sclerosis, Epilepsy, etc.), (4) reported alcohol use, and (5) normal or corrected vision and hearing (e.g., glasses, contacts, hearing aids). Exclusion criteria included current treatment for cognition, mood, fatigue, or substance use or nonpharmacological treatment for sleep. Participants who received pharmacological treatment for sleep were included in the study and medication usage was treated as a potential covariate. After completing the online survey, participants were compensated $6.50. All study procedures were approved by the University of Missouri Institutional Review Board.
Measures
Hypertension
Participants completed a brief online medical history questionnaire assessing history of neurological diseases, psychological disorders, and gastrointestinal problems. Hypertension was assessed using the item, “Do you have high blood pressure?” (0 = no, 1 = yes). In middle-aged and older adults, self-reported hypertension diagnosis has an 86% agreement rating with objective hypertension diagnosis, 48 with sensitivity rates ranging from 75.5% to 91% and specificity rates ranging from 91% to 96.4%. 49 –51
Alcohol use disorder identification test
The consumption items of the Alcohol Use Disorder Identification Test-C (AUDIT-C) assess typical drinking quantity and frequency over the past year. 52,53 The three items include, “How often do you have a drink containing alcohol?” ranging from 0 (never) to 4 (4+ per week), “How many containing alcohol do you have on a typical day when you are drinking?” ranging from 0 (not applicable/1 or 2 drinks) to 4 (10+ drinks), and “How often do you have six or more drinks on one occasion?” ranging from 0 (never) to 4 (daily). 52,53 Scores are summed, with higher scores indicating more alcohol use. The cutoff score for potential hazardous drinking in older adults is five for men and four for women. 54 The AUDIT-C has good internal psychometric properties. 55 Importantly, self-reported alcohol use is comparable with objective alcohol measures, with sensitivity rates ranging from 82.6% to 100% and specificity rates ranging from 72% to 81.3%. 53,56,57
Everyday subjective cognition–Cognitive Failures Questionnaire
In the Cognitive Failures Questionnaire (CFQ), participants reported the degree to which they experienced 25 everyday failures over the past month in four CFQ subscores 58 : CFQ-memory (8 items measuring memory errors and forgetfulness, e.g., “Do you forget appointments?”; scores ranging from 0 to 32), CFQ-distractibility (9 items measuring disruption in attentional control, e.g., “Do you forget why you went from one part of the house to other?”; scores ranging from 0 to 36), CFQ-blunders (7 items measuring social blunders and poor motor control, e.g., “Do you leave important letters unanswered for days?”; scores ranging from 0 to 28), and CFQ-names (2 items measuring proper names memory, e.g., “Do you find you forget people's names?”; scores ranging from 0 to 8).
Responses range from 0 (never) to 4 (always), with possible scores ranging from 0 to 100. 59 The CFQ has demonstrated high internal validity (α = 0.91), along with addition exceptional psychometric properties. 58 The individual overall score for CFQ-total and subscores was used in analyses, with higher scores indicating greater everyday cognitive failures (i.e., worse subjective cognition).
Statistical analysis
Moderated regression analyses were conducted in R. 60 The five subjective cognition criterion variables (CFQ-total, CFQ-memory, CFQ-distractibility, CFQ-blunders, and CFQ-names) were tested in separate models. Independent variables included alcohol use (AUDIT-C), hypertension (0 = no and 1 = yes), sex (0 = male and 1 = female), all two-way interactions, and the three-way interaction (alcohol × hypertension × sex). Analyses controlled for age, years of education, race, body mass index, smoking status (ever smoked a cigarette; 0 = no; 1 = yes), depressive symptoms (measured by Hospital Anxiety and Depression Scale subscale), 61 global subjective sleep quality (measured by Pittsburgh Sleep Quality Index total score), 62 number of prescription medications used, and number of medical conditions (excluding hypertension).
Regression coefficients and η 2 for the interaction terms (by anova_stats) 63 were used as effect sizes (small = 0.02, medium = 0.13, and large = 0.26). 64 –66 In the case of significant interactions, simple slopes were conducted in reghelper 67 to further evaluate the strength of associations between alcohol use and subjective cognitive performance at different levels of the moderator (with/without hypertension), separately for men and women. Due to the limited research regarding interactive relationships between subjective cognition, hypertension, and alcohol use in older adults, family-wise error corrections were not conducted and we accepted the false-positive risk in our analyses. 68 Alpha levels of p < 0.05 were used for all analyses.
Results
Participant demographics and descriptive values for alcohol, hypertension, sex, and cognition variables are provided in Table 1. A total of 275 participants (M Age = 64.66 years, SDAge = 7.87; 151 men/124 women) completed all measures and were included in analyses. Given that participants self-selected to complete online survey measures, demographic characteristics were compared to the US Census Bureau 69 reports for similar age ranges. Most participants reported at least some college education (65%) or graduate/professional school (14%). This is a slight overestimate from national data, where ∼50% reported at least some college and 14% completed graduate/professional schooling. 69 However, other demographic characteristics were consistent with those reported in the US census. Thus, this sample can be considered appropriately generalizable to other community-dwelling middle-aged and older adults in the United States.
Participant Characteristics
Hypertension was parsed out from number of medical conditions.
Heavy alcohol use was defined as a general cutoff score of ≥4, 100 while sex-specific cutoff score for women was ≥4 and ≥5 for men 54 for the AUDIT-C.
Significant differences between men and women (p's < 0.05).
AUDIT-C, Alcohol Use Disorder Test-C; BMI, body mass index; CFQ, Cognitive Failures Questionnaire; HADS, Hospital Anxiety and Depression Scale; Med, Medication; PSQI, Pittsburgh Sleep Quality Index.
Differences between men and women were evaluated by independent sample t-tests and chi-square tests for continuous and categorical variables, respectively. As shown in Table 1, there was no sex difference for most variables (p's > 0.05), except for men reporting more CFQ-blunders (p = 0.049) and CFQ-name errors (p = 0.01) compared to women.
Regression results
All models explained a significant amount of variance (7%–23%) in subjective cognition: CFQ-total (Full Model R 2 adjusted = 0.23, p < 0.001), CFQ-memory (Full Model R 2 adjusted = 0.19, p < 0.001), CFQ-distractibility (Full Model R 2 adjusted = 0.20 p < 0.001), CFQ-blunders (Full Model R 2 adjusted = 0.20, p < 0.001), and CFQ-names (Full Model R 2 adjusted = 0.07, p = 0.003). Alcohol use and hypertension were not significantly associated with CFQ-total or any of the subscores in conditional models (Table 2). Sex was also not associated with CFQ-total and subscores in conditional models, with the exception of the CFQ-distractibility model. Specifically, women reported higher CFQ-distractibility scores than men (Table 2).
Moderated Regression Results of Associations Between Alcohol Consumption on Subjective Cognition, and Moderated by Hypertension and Sex in Middle-Aged and Older Adults
Bold values indicate statistically significant finding (p < .05).
AUDIT-C = Alcohol measured by Alcohol Use Disorder Test-C. HADS = Depressive symptoms measured by Hospital Anxiety and Depression Scale. PSQI = Global sleep quality measured by Pittsburgh Sleep Quality Index total score.
Alc, alcohol use; HTN, hypertension.
As presented in Table 2, there was a small, but significant three-way interaction between alcohol use, hypertension, and sex in the prediction of CFQ-distractibility (p = 0.01, η 2 = 0.02). In follow-up tests of simple slopes, greater alcohol use was associated with higher CFQ-distractibility scores, but only in women with hypertension (B = 0.96, SE = 0.34, p = 0.005; Fig. 1). Alcohol use was not associated with CFQ-distractibility among women without hypertension (B = −0.73, SE = 0.47, p = 0.12), men with hypertension (B = −0.19, SE = 0.22, p = 0.41), or men without hypertension (B = −0.16, SE = 0.27, p = 0.55). The three-way interaction was not significant in the prediction of CFQ-total (p = 0.06), CFQ-memory (p = 0.20), CFQ-blunders (p = 0.22), and CFQ-names (p = 0.08).
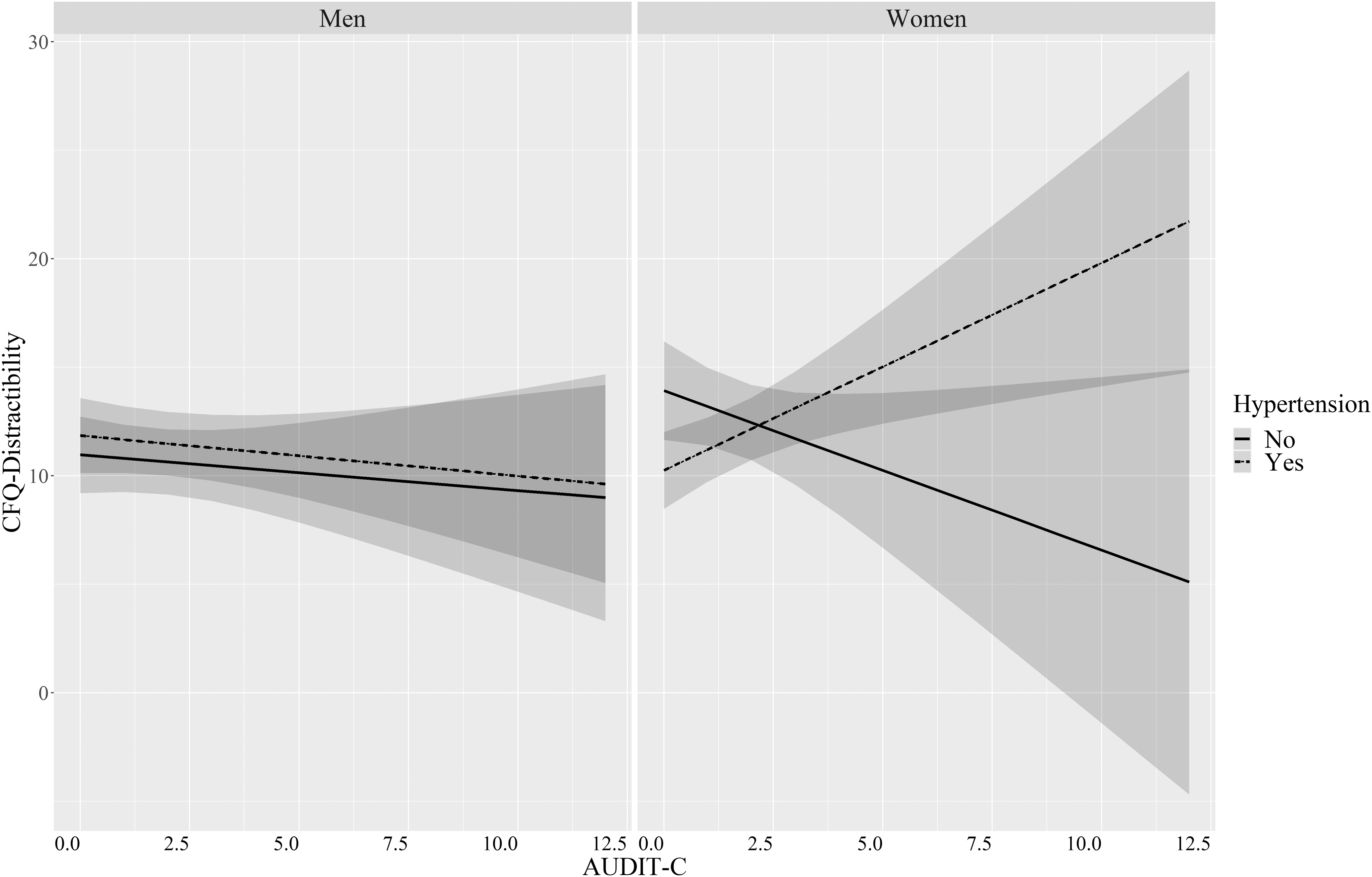
Simple slope regression analyses demonstrate that greater alcohol use is associated with higher CFQ-distractibility scores (i.e., worse attentional control) in middle-aged and older adult women with hypertension, but not men. In women without hypertension, there was no significant relationship observed. AUDIT, Alcohol Use Disorder Identification Test; CFQ, Cognitive Failures Questionnaire; Error bands, standard error.
Several significant two-way interactions between hypertension and sex are also worth noting (Table 2). Interactions between hypertension and sex were significantly associated with CFQ-total (p = 0.009, η 2 = 0.009, small effect), CFQ-memory (p = 0.02, η 2 = 0.01, small effect), and CFQ-blunders (p = 0.02, η 2 = 0.01, small effect). Specifically, presence of hypertension was associated with worse CFQ-blunders among men (B = 1.49, SE = 0.75, p = 0.049), but not women (p = 0.53).
Simple slopes of the association between hypertension and subjective cognition were nonsignificant for CFQ-total for men (p = 0.09) and women (p = 0.59). Likewise, simple slopes between hypertension and subjective cognition were nonsignificant for CFQ-memory in men (p = 0.06) and women (p = 0.52). The interaction between hypertension and sex was not associated with CFQ-names (p = 0.08). Interactions between alcohol use and sex, as well as alcohol use and hypertension were not associated with CFQ-total or subscores (p's ≥ 0.05).
Discussion
This study tested the impact of hypertension and sex on the association between alcohol use and everyday subjective cognition in middle-aged and older adults. Findings show that in women (not men) with hypertension, greater alcohol use was associated with more cognitive failures related to distractibility.
Our first hypothesis that greater self-reported alcohol use would be associated with worse everyday subjective cognitive performance and would be exacerbated in those with hypertension was not supported. Rather, our findings point to a unique sex-specific consideration in this relationship, in support of our second hypothesis that sex moderates this relationship for specific subjective cognitive domains. Alcohol use and hypertension were also not associated with everyday cognitive health in middle-aged and older adults, in agreement with some prior studies regarding alcohol use 34,35,40 and hypertension. 18,19
There are several potential explanations regarding our sex-specific findings. Unlike men, postmenopausal women (like many of the women in this sample; women M age = 65.1) experience decreased estrogen and progesterone levels relative to their nonmenopausal counterparts. 70 These hormonal decreases have been linked with increased oxidative stress, 71 which is also observed in women with hypertension 72 and alcohol use disorders. 73,74 Importantly, oxidative stress is especially high in women (relative to men) with alcohol use disorders. 73 Since oxidative stress is linked with cognitive dysfunction in older adults, 75 it is one potential mechanism by which hypertension and sex may modify the impact of alcohol on subjective cognition.
Brain mechanisms may also play a role in the patterns of cognitive domains impacted by alcohol and hypertension. Loss of estrogen and progesterone in postmenopausal women has been linked with morphological changes in gray matter volume in prefrontal cortex regions, 76,77 which may contribute to poor executive functioning. Reduced connectivity in frontoparietal pathways is associated with poor top-down attention control. 78 The self-reported distractibility complaints in this study are also associated with parietal cortex function. 79 The interplay of increased alcohol use and hypertension on distractibility in women may reflect disruption to frontoparietal neural networks. This is important information as early Alzheimer's patients, who are twice as likely to be women, 80 experience early impairments in attention control and morphological changes in these top-down attentional control networks. 78
Further, gender-specific alcohol use motives may contribute to these findings. For instance, some recent studies suggest that women are more likely than men to use alcohol when experiencing negative emotions (e.g., psychological distress, external and internal conflict). 81,82 Medicinal alcohol use is also greater in women (19.30%) than men (18.90%) and has been linked to hypertension (19%) and mood impairment (23%). 83 It is possible that drinking motives may be a contributing factor to this interactive association between hypertension, alcohol use, sex, and cognition, and prospective studies are warranted to determine the impact of drinking motives on this sex-specific interactive relationship.
Although older women have an increased risk for hypertension 10 and this was reflected in our study sample (62% of women had hypertension compared to 51% of men), the independent impact of hypertension on cognitive functioning related to social/motor blunders (as reflected in the two-way interaction) was more apparent in men. It is possible the hypertensive inflammatory response may be a contributing factor to the damage of dopaminergic neurons in substantia nigra leading to motor deficits 84 and poor cognition, 85 while estrogen in women may provide some neuroprotective effect on dopaminergic neurons. 86 An abundant amount of estrogen receptors has been found in forebrain regions (i.e., substantia nigra and ventral tegmental area) 87,88 and is linked with motor function, 89 potentially explaining estrogen-specific neuroprotective effects in specific brain regions.
It is also possible that gender-specific adherence to antihypertensive treatment may impact hypertension on cognitive functioning. For instance, adherence to antihypertensives is generally lower in men (56%) compared to women (68%). 90 Older men also tend to have worse awareness, detection, and management of blood pressure, 91 while women tend to have a higher level of care-seeking behavior compared to men. 90 Further examining the sex-specific adherence to hypertension treatment is warranted to further understand the relationship between hypertension and poor cognitive health in older men.
Although more research is warranted to delineate sex-specific associations of hypertension and alcohol use on everyday subjective cognition over time, findings may inform underlying sex- and/or gender-specific factors that can contribute to cognitive decline. Subjective cognitive complaints are associated with the risk of future cognitive impairment 92 and more women than men are diagnosed with Alzheimer's disease. 5,80 Thus, our findings suggest that monitoring alcohol intake and hypertension (both blood pressure and potentially treatment), and assessing individuals' distractibility in everyday life (i.e., attentional control) may be particularly important during clinical assessments in women to identify potential risk of cognitive decline and provide early intervention.
This study has several limitations. First, the survey was completed anonymously online at one time point. We followed recommended procedures to mitigate concerns regarding data quality and reliability (i.e., prescreening questions, only one response per IP address). 93 However, the cross-sectional design precludes understanding of whether hypertension preceded regular alcohol use or vice versa; and the temporality of these associations is important for understanding etiology and informing prevention and treatment. Second, we only included self-report measures. Although objective measures have high agreement with self-reported measures of hypertension (agreement rate of 86%) 48 and alcohol use (sensitivity rates ranging 82.6%–100% and specificity rates ranging 72%–81.3%), 53,56,57 patterns of associations may differ when using objective measures. Third, we did not assess the duration/severity of hypertension or history of treatment, or include objective measures of blood pressure. Controlling for the number of prescription medications (including any hypertension medications) did not impact the pattern of results, providing some indication that associations may be robust to clinical management with medication. Future investigators are encouraged to consider these variables as moderators of associations between alcohol use and cognition, given that neurocognitive effects of hypertension vary as a function of duration, 8,94 severity, 2 and treatment of the disorder. 95 Fourth, although we excluded for neurological disorders and controlled for medical conditions (including heart disease and diabetes), we did not explicitly assess histories of transient ischemic attacks (TIAs) or other potential vascular complications of hypertension. Given known associations between alcohol use 96 –98 and TIAs, investigators are encouraged to consider these alternative endpoints in future work. Finally, although a notable strength of the study was that a comparable number of men and women older adults were included (55% men; 45% women), the study sample lacked racial and ethnic diversity (88% White/Caucasian) and future studies should examine these findings in a more racially and ethnically diverse sample. Likewise, rates of cardiovascular diseases 45 –47 and poor cognition 99 may be higher—and patterns of association may differ—in heavier drinking samples.
Conclusion
To our knowledge, this is the first study to examine sex-specific associations between hypertension, alcohol use, and subjective cognition in middle-aged and older adults. In women with hypertension, greater alcohol use is negatively associated with attentional control. Exploration of sex- and/or gender-specific mechanisms underlying this relationship is warranted, especially in prospective studies. Continued research in this area is expected to inform sex-specific treatments that mitigate risk of cognitive decline in middle-aged and older adults.
Footnotes
Acknowledgments
We would like to acknowledge Jacob Wilhelm for assisting with the preparation of the Institutional Review Board application. Study data, analytical methods, and study materials can be made available upon request of the corresponding author. This study was not preregistered.
Authors' Contributions
M.M.: conceptualization (lead); writing—original draft (lead); formal analysis (lead); visualization (lead); and writing—review and editing (equal). A.N.C.: writing—original draft (equal) and writing—review and editing (equal). V.S.: writing—original draft (equal) and writing—review and editing (equal). M.-B.M.: writing—review and editing (equal). A.F.C.: conceptualization (supporting); writing—original draft (supporting); writing—review and editing (lead); formal analysis (supporting); and supervision (lead).
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.