
Abstract
Background:
Antidepressants are among the most prescribed medications in the United States. The aim of this study was to explore the prevalence of antidepressant prescriptions and investigate sex differences and age-sex interactions in adults enrolled in the Right Drug, Right Dose, Right Time: Using Genomic Data to Individualize Treatment (RIGHT) study.
Materials and Methods:
We conducted a retrospective analysis of the RIGHT study. Using electronic prescriptions, we assessed 12-month prevalence of antidepressant treatment. Sex differences and age-sex interactions were evaluated using multivariable logistic regression and flexible recursive smoothing splines.
Results:
The sample consisted of 11,087 participants (60% women). Antidepressant prescription prevalence was 22.24% (27.96% women, 13.58% men). After adjusting for age and enrollment year, women had significantly greater odds of antidepressant prescription (odds ratio = 2.29; 95% confidence interval = 2.07, 2.54). Furthermore, selective serotonin reuptake inhibitors (SSRIs) had a significant age-sex interaction. While SSRI prescriptions in men showed a sustained decrease with age, there was no such decline for women until after reaching ∼50 years of age. There are important limitations to consider in this study. Electronic prescription data were cross-sectional; information on treatment duration or adherence was not collected; this cohort is not nationally representative; and enrollment occurred over a broad period, introducing confounding by changes in temporal prescribing practices.
Conclusions:
Underscored by the significant interaction between age and sex on odds of SSRI prescription, our results warrant age to be incorporated as a mediator when investigating sex differences in mental illness, especially mood disorders and their treatment.
Introduction
Antidepressant use has steadily increased over several decades to the point that antidepressants now represent third most commonly prescribed medication class in the United States after analgesics and antihyperlipidemics. 1 –5 Overall, ∼30 medications have been approved by the Food and Drug Administration as antidepressants, spanning at least eight different mechanisms of action. 6 Aside from their wide utilization as the first-line choice of pharmacotherapy for major depressive disorder (MDD), 7 antidepressants are also used on- and off-label for a number of other psychiatric conditions, including bipolar disorder (BD), 8 anxiety disorders, 9 eating disorders, 10 obsessive-compulsive and related disorders, 11 post-traumatic stress disorder, 12 and multiple general medical conditions such as pain syndromes, 13 –15 smoking cessation, 16 sexual dysfunctions, 17 and postmenopausal vasomotor symptoms. 18
As highlighted by data from the 2013 Medical Expenditure Panel Survey, women are prescribed antidepressants at double the rate than men (15.9% vs. 7.7%). 19 National Health and Nutrition Examination Survey data from 2009–2010 through 2017–2018 showed that the significant increase in antidepressant use among adults only remained significant for women after sex stratification. 4 Moreover, the disparity grows with age, and older age groups show the widest gap in rates of antidepressant use by sex. 4,20 Our own work from the Rochester Epidemiology Project (REP) identified a peak antidepressant prevalence rate of 29.8% in 50- to 64-year-old women among a geographically-defined population. 21 Despite MDD being the primary indication for antidepressants and women having twice the risk of MDD than men do, 22 the myriad conditions for which antidepressants are used suggest that such sex disparities may not be solely explained by the different rates of MDD between sexes, or even just psychiatric conditions.
Despite data showing smaller differences between active drugs compared to placebo, head-to-head comparison of antidepressants shows more variability in efficacy and acceptability in the treatment of depression. 23 There is considerable pharmacokinetic and pharmacodynamic variation among antidepressants, causing differences in side effects, interactions, and tolerability. 24 Despite conflicting evidence, data show age related sex differences in antidepressant response in depression. 25 However, taken together, these differences may be facilitating treatment selection in specific situations (e.g., an agent with few interactions for patients with polypharmacy). 26 Beyond the data on difference in treatment outcomes among different antidepressants and possible underlying biological reasons, there is considerable variation in antidepressant availability and cost, in addition to differences in prescribing practices across regions and among demographic groups. 27 –32 Previous reports have described differences in the likelihood of being prescribed different classes of antidepressants by sex or age—particularly in older age groups. 31,33
Our primary aim was to assess the cross-sectional prevalence of antidepressant use and investigate potential sex-related differences utilizing prescription data from the Right Drug, Right Dose, Right Time: Using Genomic Data to Individualize Treatment (RIGHT) study. Our secondary aim was to investigate age-dependent differences in antidepressant prescriptions by sex. We hypothesized that (1) the prevalence rates of antidepressant prescriptions would differ by sex, (2) that these differences would vary among individual antidepressants and antidepressant classes, and (3) that age would significantly impact the sex-related differences in antidepressant prescriptions. To our knowledge, this is the first study to evaluate sex differences in the rate of antidepressant prescriptions as a function of age in a naturalistic setting.
Materials and Methods
Study design and participants
This is a retrospective study involving participants enrolled in the RIGHT study, including its pilot and final cohorts. 34,35 The RIGHT study was originally developed to explore how preemptive pharmacogenomic testing influenced clinical and patient outcomes, expand research into genetic variants of unknown significance, and analyze changes in patient–clinician interactions. Adult community volunteers with primary care set up in Mayo Clinic and previously stored DNA samples at the Mayo Clinic Biobank (previously described in detail 36 ) were invited to participate in the RIGHT study in two waves. Prior enrollment and sample donation to the Mayo Clinic Biobank occurred between 2009 and 2017. The first wave of RIGHT invitations took place between 2012 and 2013 (n = 1,013) and the second wave during 2016–2017 (n = 10,085). The RIGHT study is a collaboration between Mayo Clinic and Baylor College of Medicine. This project identified 11,098 participants that consented to clinical pharmacogenomic testing of their previously stored samples and subsequent deposit of these results into their electronic health records (EHRs) for clinical use. EHRs were linked through the REP, a medical records-linkage system of different regional health care providers from southern Minnesota and western Wisconsin. 37
The RIGHT study was approved by the Mayo Clinic and Olmsted Medical Center Institutional Review Boards (Mayo Clinic IRB #12-003371) and was conducted in accordance with the Declaration of Helsinki. For this retrospective analysis focused on antidepressant prescriptions (Mayo Clinic IRB #16-006077), to obtain a cross-sectional view of cohort participants, we targeted the immediate 12-month period preceding each participant's date of enrollment and sample donation to the Mayo Clinic Biobank (hereafter “enrollment year”). Eligibility criteria followed those outlined in the RIGHT cohorts 35 with no additional criteria defined for this investigation.
Data collection and quality control
REP electronic prescription data from 1 year before enrollment to the Mayo Clinic Biobank were analyzed. Data were coded using RxNorm and classified using the National Drug File-Reference Terminology coding system. 38 We focused on commonly used antidepressants, including monotherapy and adjunctive interventions, resulting in a list of 37 drugs of interest classified into 11 drug classes (Supplementary Table S1). Inclusion was not limited to any specific diagnosis to obtain overall prescription rate for all antidepressants. However, as an exploratory assessment, International Classification of Diseases code sets for MDD, BD, and anxiety disorders (Supplementary Table S2) were pulled for the 5-year period preceding cohort enrollment for all participants.
Statistical analysis
The 12-month prevalence rates of participants receiving antidepressant prescriptions were determined by the presence of any prescription in participants' EHRs during the period of interest and presented using counts and percentages. To avoid double counting prescriptions, we collapsed prescription counts on three levels. When collapsing counts at the individual drug level, prescriptions were counted once for each of the 37 drugs of interests for each unique participant. At the class level, instances where a participant had been prescribed more than one antidepressant within the same class (e.g., two selective serotonin reuptake inhibitors [SSRIs]) were only counted once. Finally, at the antidepressant level, participants with any antidepressant prescription were counted once.
Differences in prescription rates by sex were investigated using multivariable logistic regression, adjusted for age and enrollment year. The latter to avoid confounding by trends over time in antidepressant prescription patterns. 1 Odds ratio (OR) estimates and standard errors are reported. Given the low overall rates of prescription across drugs and drug classes, analyses were performed using the Firth penalized likelihood approach. Statistical significance was determined based on the Wald test of the sex effect. Testing was restricted to antidepressants/classes where the absolute number of participants with a positive prescription status was ≥30.
Flexible recursive smoothing splines were used to investigate age-dependent sex differences in prescription rates. Specifically, flexible spline effects of age and enrollment year were included along with sex, and an age-sex interaction was evaluated using a likelihood ratio test. Visualizations of age/secular effects were generated from sex-stratified models. Testing was restricted to antidepressants/classes where the absolute number of participants with a positive prescription status was ≥100. Significance of statistical testing was determined based on a Holm-corrected p-value <0.05 to account for multiple testing based on the total number of eligible analyses.
Results
Demographic characteristics of the sample are summarized in Table 1. The final sample consisted of all participants enrolled in the RIGHT cohorts (n = 11,087) excluding 11 participants that withdrew consent after enrollment. Overall, mean age was 57.7 years (standard deviation = 13.7), and ∼60% of all participants were women (n = 6,682). Participants were predominantly white (94.14%), non-Hispanic (98.9%), and endorsed at least some college education at enrollment (87.44%). Among all participants, 15.3%, 9.5%, and 2.1% had diagnostic codes for MDD, anxiety disorders, and BD in their EHRs, respectively (Table 2).
Demographic Characteristics of Participants Enrolled in the RIGHT Study
Participant age is based on date of enrollment and sample donation (enrollment year) to the Mayo Clinic Biobank.
GED, General Educational Development Test; RIGHT, Right Drug, Right Dose, Right Time: Using Genomic Data to Individualize Treatment; SD, standard deviation.
Age and Presence of Diagnostic Codes for Major Depressive Disorder, Bipolar Disorders, and Anxiety Disorders Among RIGHT Participants Stratified by Sex and Prescription Status
Code sets are inclusive for their respective diagnostic codes, but not exclusive of other code sets, resulting in overlap.
ICD, International Classification of Diseases; Rx, participants with at least one antidepressant prescription.
After collapsing prescription counts for the presence of any drug of interest (i.e., antidepressant level), hence avoiding double counting, the 12-month prevalence rate of antidepressant prescriptions was 22.24% (n = 2,466). Women had a higher crude proportion of antidepressant prescriptions during the period of interest (27.96%; n = 1,868/6,682) than men (13.58%; n = 598/4,405). Among participants with at least one antidepressant prescription, distribution of prescription counts (i.e., having one, two, or three to six prescriptions) was similar for both sexes (Supplementary Table S3).
At the class level, SSRIs had the most prescriptions among participants (13.64%; n = 1,512); this held true when stratifying by sex. The second most prescribed class overall was norepinephrine and dopamine reuptake inhibitors (NDRIs)—comprised only of bupropion (4.02%; n = 446). When stratified by sex, the proportion of women with serotonin and norepinephrine reuptake inhibitor (SNRI) use (5.06%; n = 338) was second to SSRIs, followed by NDRIs (4.97%, n = 332) and tricyclic antidepressants (TCAs) (4.55%; n = 304), whereas for men, NDRIs were the second-most prescribed class (2.59%; n = 114) followed by TCAs (2.16%; n = 95) and SNRIs (1.73%; n = 76). The complete 12-month prevalence rates are shown in Table 3.
RIGHT Study 12-Month Prevalence of Antidepressant Prescriptions by Drug, Class, and Overall, Stratified by Sex
Prescription counts for antidepressant classes were collapsed at the class level. Instances where a participant had prescriptions for two or more antidepressants belonging to the same class were only counted once.
At the antidepressant level, participants with antidepressant prescriptions were only counted once irrespective of the number of different prescriptions.
MAOI, monoamine oxidase inhibitor; NDRI, norepinephrine and dopamine reuptake inhibitor; NRI, norepinephrine reuptake inhibitor; SNRI, serotonin and norepinephrine reuptake inhibitor; SSRI, selective serotonin reuptake inhibitor; TCA, tricyclic antidepressant; TeCA, tetracyclic antidepressant.
After adjusting for age and enrollment year, men and women had significant differences in prescription rates of several individual antidepressants and antidepressant classes (Table 4). Overall, women had significantly higher relative odds of being prescribed any antidepressant in comparison to men (OR = 2.29; 95% confidence interval [CI] = 2.07, 2.54; p < 0.0001). This held true for SSRIs as a class (OR = 1.97; 95% CI = 1.74, 2.24; p < 0.0001), SNRIs (OR = 2.80; 95% CI = 2.18, 3.64; p < 0.0001), TCAs (OR = 2.29; 95% CI = 1.81, 2.92; p < 0.0001), and NDRIs (OR = 1.65; 95% CI = 1.32, 2.06; p = 0.00007), as well as multiple individual antidepressants.
Age- and Enrollment Year-Adjusted Differences in Antidepressant Prescription Rates by Sex
The analysis models sex such that women = 1 and men = 0 (i.e., odds of women relative to men). The results present the number of prescriptions by sex, along with the log(OR) and its SE, the transformed OR, and finally the Wald p-value. Significant results are presented in bold. Rx = prescription status.
Adjusted for age and calendar year at time of enrollment. Adjusted p-values consider the complete set of analysis results (individual drugs and drug categories).
Prescription counts for antidepressant classes were collapsed at the class level. Instances where a participant had prescriptions for two or more antidepressants belonging to the same class were only counted once.
At the antidepressant level, participants with antidepressant prescriptions were only counted once irrespective of the number of different prescriptions.
CI, confidence interval; OR, odds ratio; SE, standard error.
When testing age-dependent sex differences, only SSRI prescription rates showed a significant age-sex interaction (p < 0.05) (Table 5). To visualize this effect, adjusted log-odds of SSRI prescription were plotted for age and stratified by sex (Fig. 1). Men had a sustained reduction of SSRI prescriptions as a function of age. In contrast, women showed a slight increase of SSRI prescriptions until ∼50 years of age, when prescriptions began a gradual decline like that of men. The maximum difference in estimated probability of SSRI prescription by age occurred at 55 years [Prob(M) = 0.084; Prob(F) = 0.169; Diff = 0.085]. The only class for which we did not observe prescription decline with age at any point in time was TCAs in women, although these observations were not significant for age-sex interactions. All age-sex interaction model plots are available in the Supplementary Material.
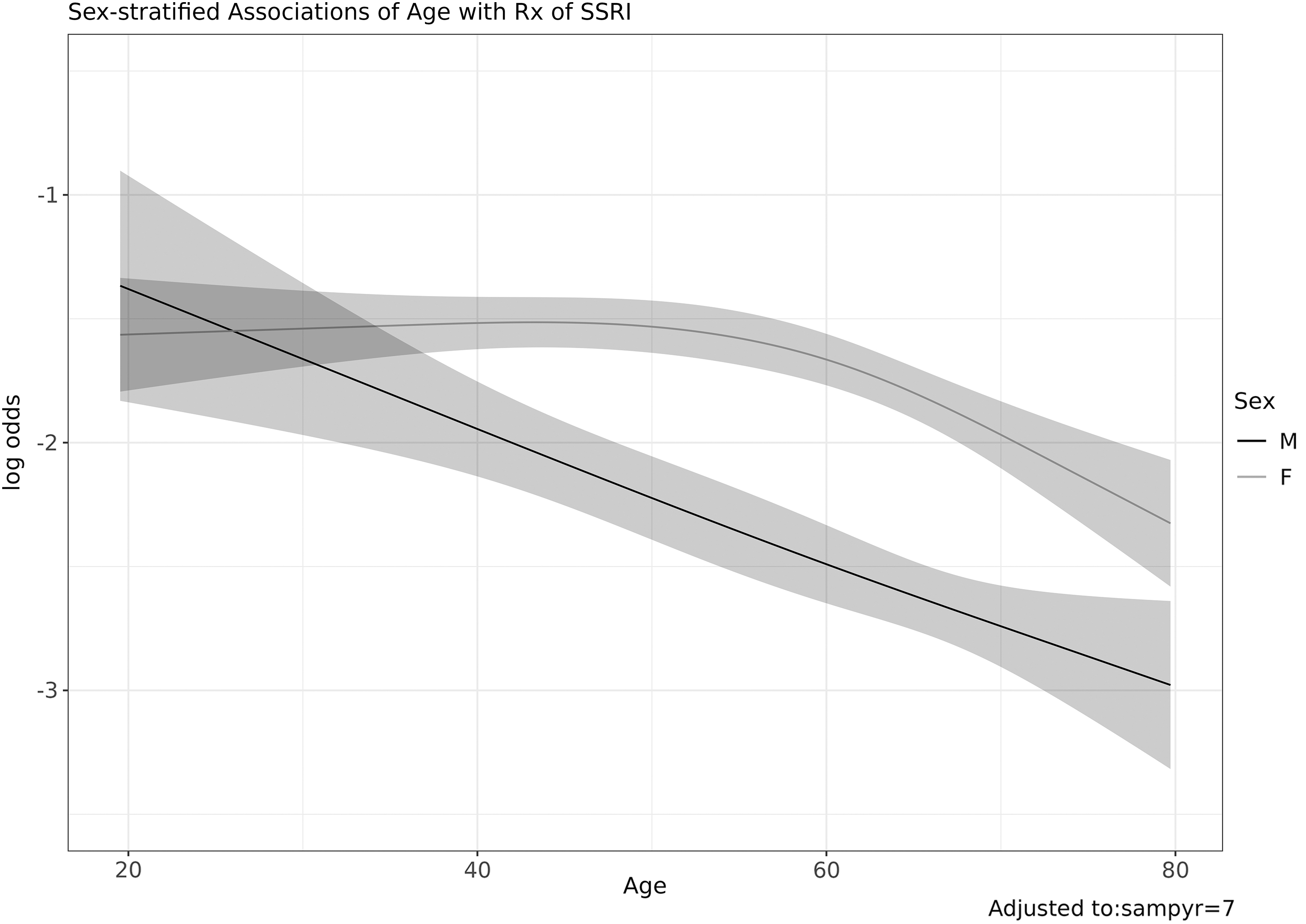
Log odds of prescription for SSRIs by sex. Models the log odds of antidepressant prescriptions of the SSRI by age of cohort participants, stratified by sex and adjusted for year of enrollment. SSRI, selective serotonin reuptake inhibitors.
Age-Dependent Differences in Antidepressant Prescription Rates by Sex, Adjusted for Calendar Year
The analysis models effects of age and sample collection year (modeled as year-2004) using restricted cubic splines to flexibly allow for nonlinearity. The results present the number of prescriptions by sex, as well as the likelihood ratio test p-value (unadjusted and adjusted for multiple testing). Rx = prescription status.
Significant results are presented in bold.
Adjusted for age and calendar year at time of enrollment. Adjusted p-values consider the complete set of analysis results (individual drugs and drug categories).
Prescription counts for antidepressant classes were collapsed at the class level. Instances where a participant had prescriptions for two or more antidepressants belonging to the same class were only counted once.
At the antidepressant level, participants with antidepressant prescriptions were only counted once irrespective of the number of different prescriptions.
Discussion
The present study provides a retrospective estimate of antidepressant use among RIGHT study participants with a special focus on sex differences and age-sex interactions. We assessed the prevalence of participants receiving antidepressant prescriptions in a 12-month period before cohort enrollment using EHRs and evaluated sex-related differences and age-sex interactions. Overall prevalence of antidepressant prescriptions was 22.24%. After controlling for confounders, women had a significantly higher likelihood of being prescribed any antidepressant than men. Age was found to significantly interact with the sex-related differences in prevalence rates of SSRI prescriptions, such that odds of prescription for women increased with age until ∼50 years of age, whereas for men they decreased as a function of age.
This cohort was part of the REP catchment area, for which the age-standardized prevalence of antidepressant prescriptions in 2019 was 15.38% overall (19.91% for women, 10.62% for men); the highest rate was seen in women aged 40–64 years (27.74% prevalence). 39 Furthermore, antidepressant prescriptions appear to have been increasing in the REP as evidenced by the rise observed between the periods of 2005 to 2011 and 2012 to 2019, 21,39 much like what we have seen in population-based studies across the country. In the RIGHT cohorts, we observe higher overall and sex-stratified prevalence rates of antidepressant prescriptions than in REP, although during a broad period not necessarily representative of a longitudinal increase in prescriptions. A plausible explanation for the higher number of antidepressant prescriptions observed in this sample could be due to the enrichment of the cohort for participants with primary care established in Mayo Clinic, thus not reflective of the regional population but a more selective population.
Even though MDD is the primary indication for antidepressants, recent years have seen relatively little variation in MDD prevalence rates or in the percentage of adults being treated for MDD. 40 –42 In addition, MDD only accounts for roughly half of all antidepressant prescriptions in primary care, where most antidepressants are prescribed. 7,43 Therefore, the growing rate of antidepressant use may be due to other indications, a third of which may be off-label, 7 highlighting the need to understand antidepressant use in general in addition to specific indications. Comparably, in this study we observed that 51.6% of participants with at least one antidepressant prescription had a diagnostic code for MDD in their EHR. Anxiety disorder diagnostic codes were present in 28.2% and BD in 6.6% of participants with antidepressant prescriptions. However, code sets were not mutually exclusive, and overlap between diagnoses is expected. As our research questions did not pertain to a specific condition, we neither pursued ascertainment of these diagnoses nor incorporated these in our statistical models, as their exploration would be best suited for disease-oriented research.
We found SSRIs to be the most frequently prescribed antidepressant class, accounting for 49.8% of all prescriptions at the class level, in line with previous reports. In the United States, for the past 25 years, SSRIs have been the most prescribed class of antidepressants 1,2,44,45 ; also topping antidepressant prescriptions across Europe and in Qatar. 31,32 In this study, SNRIs were the second most prescribed class for women, but the fourth for men. Even though we did not find a significant age-sex interaction for SNRIs in our data, or for individual SNRI antidepressants, we observed an interesting behavior in SNRI prescriptions. Prescription rates for SNRIs constantly increased until women approached 54 years of age, when they showed a sharp decline. In contrast, men showed a steep decline in SNRI prescriptions after age 50. The observed sex-related differences in frequency and age distribution of SNRI prescriptions could be influenced by prescribing practices during peri- and postmenopause, given the older age distribution of our sample and the higher overall prevalence of depressive symptoms during these life stages. 46 In addition, SNRIs, particularly venlafaxine, have demonstrated efficacy in reducing the frequency and intensity of the vasomotor symptoms of menopause. 18,46 –48 Similarly, chronic neuropathic pain, a routine indication for SNRI treatment, 15 and stress urinary incontinence, for which duloxetine is used off-label, 49 occur most frequently in women over 50 and 40 years of age, respectively. 50,51
In contrast, we observed a steady increase in TCA prescriptions for women as a function of age, without any decline, unlike other antidepressant classes where we observed drops in the prescription rates for women after periods of slow increase—except for adjunctive medications, in which there were no rises in the prescription rates. Interpretation is limited, as these results did not reach statistical significance. Nevertheless, TCAs may be more efficacious than other antidepressant classes among elderly women. Contrary to the deficient response to TCAs compared to SSRIs in premenopausal women, response rate to TCAs is higher compared with SSRIs in postmenopausal women. 52 –54 Interestingly, poor response to SSRI among postmenopausal women is reduced by hormone replacement therapy, 55 suggesting that female sex hormones may have a role in such differences. However, the safety of TCAs in older individuals is controversial. Despite recommendations from the American Geriatrics Society to avoid TCA prescription in those over 65 years old due to their strong anticholinergic effect, 56 studies exploring their effect on cognitive impairment have had conflicting results. 57,58 In addition, two reports found them protective against dementia, possibly through modulation of glial inflammatory activation 59 or inhibition of TNF-α and amyloid beta accumulation, 60 whereas other antidepressant classes increased the risk of dementia. 61,62
The sex-stratified raw prevalence of antidepressant prescriptions in women was approximately double than it was for men. No single antidepressant medication or class was prescribed more frequently to men. To better understand sex differences, in subsequent regression modeling, we adjusted for age and enrollment year and corrected for multiple testing. Women had a significantly greater likelihood of being prescribed any antidepressant and multiple antidepressant classes (NDRIs, SNRIs, SSRIs, and TCAs). SSRIs were the only antidepressant class where we observed a significant age-sex interaction in prescriptions. Unlike men's constant reduction in odds of SSRI prescription as a function of age, women showed a slight increase in prescriptions until approximately age 50, whereafter odds of SSRI prescription gradually declined. A possible reason could be peri-menopause, as menopause slows MDD recovery and decreases response to SSRIs, as discussed earlier, increasing the need to switch to different antidepressant classes. 63,64
Although women have a well-documented higher risk of anxiety and depressive disorders, 41,65,66 male-specific behaviors or clinical characteristics could also be contributing to this disparity. Men may be less willing to seek mental health treatment than women are. Using nationally representative data, Blumberg et al. reported that less than one-third of men with daily anxious or depressive thoughts had talked to a mental health professional in the past year. 67 Moreover, only 40% received any type of mental health treatment, 67 even though data suggest that sex might not influence treatment response significantly. 68 However, men endorsing cultural norms related to “masculine toughness” or “anti-femininity” appear to engage less with mental health services. 69 In addition, the clinical presentation of mental illnesses may be dissimilar between sexes. Men appear to be at a higher risk of externalizing disorders 70 and report more externalizing symptoms when diagnosed with internalizing disorders such as MDD. 71 Thus highlighting the need to consider sex differences when tailoring public health efforts in any given population.
Our study has several key strengths. First, the statistical modeling used in this study was deliberately conservative to avoid overestimating the effect of sex or age in the results. Second, the availability of detailed medical records for participants of the RIGHT cohorts facilitates further exploration by allowing for flexibility when building phenotypes of interest. Finally, focusing on pharmacogenomic-naive antidepressant prescription rates in the RIGHT study will be of added value as groundwork for understanding the impact of genotyping on prescription patterns in future studies. As an example, a recent report revealed that the average RIGHT participant has 3 clinically actionable gene variants for any of 13 pharmacogenes of interest, 72 supporting the utility of using such data in decision-making support tools at point-of-care.
There are important limitations to consider in this study. First, cross-sectional electronic prescription data cannot inform researchers whether any one participant was exposed to a specific antidepressant, the treatment duration, or if they maintained proper treatment adherence (e.g., a participant may be prescribed a medication and decide not to take it). Second, the RIGHT cohorts are composed of a mostly White and older population, hampering their generalizability to younger populations or other demographic groups. Consequently, differences in antidepressant prescriptions in an earlier-born population may not necessarily be an effect of age or comorbidities, but may in fact be a cohort effect, given that antidepressants have been approved at different times and that trends in prescription change through time. Finally, targeting a distinct 12-month period of interest for each participant determined by their time of enrollment in the cohort results in confounding by time-related changes in health care utilization and prescription patterns. By adjusting for enrollment year and age, we attempted to mitigate confounding by time and trends in antidepressant use and still evaluate each participant's pharmacogenomic-naive period.
Considering the widening gap in antidepressant use between sexes and the increasing number of on- and off-label indications resulting in antidepressant prescriptions, future studies must consider the influence of age on the interaction between sex and risk of disease and the subsequent sex differences in antidepressant exposure. In addition, as indirectly highlighted by our findings, hormonal change milestones in women such as the menopausal transition may be contributing to age-dependent antidepressant prescription sex differences. As such, objective markers of reproductive health and status should be included as covariates.
Conclusions
In summary, our study found a higher 12-month prevalence of antidepressant prescriptions in women among participants of the RIGHT study. Subsequently, in adjusted analyses, we observed a significantly higher likelihood of being prescribed any antidepressant in women which extended to specific antidepressant classes: SSRIs, NDRIs, SNRIs, and TCAs. Finally, upon evaluation of the effect of age on these sex differences, SSRIs showed a significant age-sex interaction. Odds of SSRI prescription in men declined with age, whereas they only declined in women after reaching ∼50 years of age, which corresponds to the typical age range for menopausal transition. 73 Further studies are needed to understand the effect of age- and sex-dependent patterns of antidepressant use in the context of lifetime hormonal stages as an underlying biological difference between women and men.
Footnotes
Authors' Contributions
J.A.S.R.: Conceptualization, Methodology, Validation, Investigation, Writing—Original draft, Writing—Review and editing, Visualization. N.I.L.: Conceptualization, Methodology, Validation, Investigation, Writing—Review and editing. N.B.L.: Conceptualization, Methodology, Software, Validation, Formal analysis, Investigation, Resources, Data curation, Writing—Original draft, Writing—Review and editing, Visualization, Supervision. G.D.J.: Software, Validation, Formal analysis, Investigation, Data curation, Writing—Review and editing. A.T.A.: Conceptualization, Validation, Investigation, Writing—Review and editing. N.A.N.: Conceptualization, Validation, Investigation, Writing—Review and editing. J.M.B.: Conceptualization, Validation, Writing—Review and editing, Supervision. S.J.W.: Conceptualization, Validation, Writing—Review and editing, Supervision. R.M.W.: Conceptualization, Methodology, Investigation, Resources, Validation, Formal analysis, Data curation, Writing—Review and editing, Supervision, Project administration. L.W.: Conceptualization, Methodology, Investigation, Resources, Validation, Formal analysis, Data curation, Writing—Review and editing, Supervision, Project administration. M.A.F.: Conceptualization, Methodology, Validation, Investigation, Resources, Data curation, Writing—Original Draft, Writing—Review and editing, Supervision, Project administration. A.O.: Conceptualization, Methodology, Validation, Investigation, Writing—Original Draft, Writing—Review and editing, Supervision, Project administration. All authors have contributed to and approved the final article. This article has not been published elsewhere and is not currently being considered by another journal. Partial and preliminary results of this research study were presented in-person as a poster presentation at the 2022 Annual Meeting of the American Psychiatric Association held in May.
Author Disclosure Statement
R.M.W. and L.W. are cofounders of and stockholders in OmeOme, LLC. M.A.F. reports the following conflicts of interest: grant support from Assurex Health and Mayo Foundation; CME/travel/honoraria from Carnot Laboratories, American Physician Institute; and financial interest/stock ownership/royalties in Chymia LLC. All the other authors declare no competing interests.
Funding Information
This research study was supported by: Mayo Clinic Center for Individualized Medicine, Mayo Foundation for Medical Education and Research, National Institute of General Medical Sciences and National Institute of Child and Health and Human Development grant GM008685 (Nicole I. Leibman), National Institute of General Medical Sciences of the National Institutes of Health under award number T32 GM008685 (Nicolas A. Nunez), and Mayo Clinic School of Graduate Medical Education (Jorge A. Sanchez-Ruiz).
Supplementary Material
Supplementary Table S1
Supplementary Table S2
Supplementary Table S3
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.