
Abstract
Objective:
To examine claims for reversible prescription contraceptives and chlamydia and gonorrhea testing among commercially and Medicaid-insured adolescent and young adult (AYA) females in the United States.
Methods:
Using IBM MarketScan Research Databases, we identified sexually active, nonpregnant AYA (15- to 24-year-old) females enrolled in 2018. We examined claims for reversible prescription contraceptives and chlamydia and gonorrhea testing, using drug names and diagnosis/procedure codes, by age-group in commercially and Medicaid-insured separately and by race/ethnicity in Medicaid-insured.
Results:
Among 15- to 19-year-old and 20- to 24-year-old females, 67.2% and 67.9% of commercially insured and 57.3% and 54.0% of Medicaid-insured, respectively, had claims for reversible prescription contraceptives in 2018. Across insurance types among both age-groups, the most common claim for contraceptives was prescription for combined oral contraceptives. Among Medicaid-insured 15- to 19-year-olds, claims for contraceptives ranged from 42.6% for Hispanic females to 63.4% for non-Hispanic White females; among Medicaid-insured 20- to 24-year-olds, claims ranged from 50.4% for non-Hispanic Black females to 57.0% for non-Hispanic White females. Approximately half of the commercially and Medicaid-insured females had claims for chlamydia and gonorrhea testing. Non-Hispanic Black females had the highest percentages of claims for chlamydia testing (56.3% among 15- to 19-year-olds and 61.1% among 20- to 24-year-olds) and gonorrhea testing (61.6% among 15- to 19-year-olds and 64.9% among 20- to 24-year-olds).
Conclusion:
Approximately, two-thirds of commercially insured and more than half of Medicaid-insured, sexually active, nonpregnant AYA females had claims for reversible prescription contraceptives. Race/ethnicity data were available for Medicaid-insured females, and there were differences in claims for contraceptives and chlamydia and gonorrhea testing by race/ethnicity. Half of the AYA females had claims for chlamydia and gonorrhea testing suggesting missed opportunities.
Introduction
Sexual and reproductive health (SRH) is an important facet of normal adolescent growth and development, and therefore, experts recommend comprehensive, evidence-based and developmentally appropriate SRH-related education and barrier-free access to services such as contraceptive services and screening and treatment of sexually transmitted infections (STIs). 1 –3 Recognizing the importance of SRH on adolescents, the United Nations Committee on the Rights of the Child advocates comprehensive sexual health information and services as basic rights for adolescents and supports adolescents’ freedom to make choices to control one’s health and body. 4 In addition to adolescent autonomy, the United Nations calls for equal access to SRH services so that every child can attain the highest standards of health. To improve health and well-being of adolescents in the United States, the objectives of Healthy People 2030 include reducing pregnancies and rates of STIs among adolescents and increasing the proportion of adolescents getting sex education, effective birth control, and screening for STIs. 5
Adolescents and young adults (AYAs) (15- to 24-year-olds) have the highest percentage of unintended pregnancy in the United States. 6 Adolescent birth rates have been shown to be higher in the United States than in other countries, for which complete pregnancy estimates were available. 7 Racial and ethnic differences exist in adolescent birth rates in the United States, with at least twofold higher rates among non-Hispanic Black, Hispanic, non-Hispanic American Indian or Alaska Native (AI/AN), and non-Hispanic Native Hawaiian or Other Pacific Islander adolescents compared with non-Hispanic White adolescents. 8 Over the years, increased use of contraceptive services, including intrauterine devices (IUDs) and implants, and decreased sexual activity have contributed to decreasing pregnancy rates among those aged 15–19 years in the United States. 9,10
Among all people of reproductive age, AYAs bear a disproportional burden of STIs. 11 Rates of chlamydia and gonorrhea in 2019 were at an all-time high since 2000 in the United States, with half of all new cases among AYAs. 12 In response to the present STI epidemic, the STI National Strategic Plan was created and recognizes AYAs, men who have sex with men, and pregnant women as priority populations. 11 Disproportionately affected groups within these populations are certain racial and ethnic minority communities such as Black, AI/AN, and Hispanic. 11 Chlamydia screening and partner notification have been found to reduce chlamydia prevalence among females. 13 The U.S. Preventive Services Task Force (USPSTF) has concluded that screening for chlamydia is associated with reduced risk of pelvic inflammatory disease and early detection and treatment of gonorrhea in women at increased risk is beneficial. 3 The USPSTF therefore recommends annual screening for chlamydia and gonorrhea in all sexually active females ≤24 years. 3
Despite recommendations, multiple barriers to adolescents’ health care access and utilization exist across all five levels of the socioecological model. Barriers are encountered at the intrapersonal level (e.g., limited knowledge of and poor previous experiences with health care services), the interpersonal level (e.g., cultural and linguistic barriers), the organizational level (e.g., structural barriers in health care systems), the community level (e.g., social stigma), and the policy level (e.g., inadequate insurance coverage). 14 Structural and interpersonal racism are known to adversely affect access and utilization of reproductive health care services and reproductive care experiences among Black women and other women of color by providing diminished and coercive contraceptive experiences and delayed reproductive health screenings leading to poor health outcomes. 15 In addition to multiple barriers, provider preferences toward certain clinical services and provider biases based on the patient’s race may lead to coercive practices. 16 –18 These barriers and biases might create gaps in knowledge and counseling from adolescent health providers about contraceptives and STIs, and therefore affect utilization of these services by AYAs. Routine contraceptive care could be a potential avenue for counseling about STI screening and care, and STI screening and care could be an opportunity to counsel on contraceptives, thus increasing counseling and providing better health care. Therefore, in this analysis, we examine both the receipt of contraceptive services and screening for STIs among AYAs.
Much of what is known about receipt of SRH services among AYAs comes from population-based surveys that rely on participant self-report. 19 Compared with older age-groups, adolescent females aged 15–19 years participating in the 2017–2019 National Survey of Family Growth (NSFG) reported the lowest current contraceptive use at 38.7%, with use increasing to 60.9% among 20- to 29-year-olds. 19 Given that the survey was conducted among all females regardless of whether they were sexually active, the differences may reflect that 15- to 19-year-olds are less likely than older women to be sexually active. Another analysis using NSFG data found that from 2011 to 2015, 50% of females aged 15–25 years reported receipt of contraceptive services during the prior year, including counseling, checkup, birth control method or prescription for birth control method, sterilization, or emergency contraception. 20 Insurance claims offer an alternative data source, not based on self-report, that can provide estimates of service receipt of reversible prescription contraceptive methods among insured populations. However, insurance claims data are unable to provide estimates on nonprescription contraceptive methods, such as condoms. Reversible prescription contraceptives include IUDs, implantable subdermal contraceptives, injectable contraceptives, combined oral contraceptives (COCs), transdermal patches, vaginal rings, progestin-only pills (POPs), and emergency contraception. Studies have used insurance claims data to evaluate the use and cost of contraceptives. 21,22 However, these studies did not estimate contraceptive use among females aged 15–24 years. Previous studies have examined chlamydia testing and screening in AYA females using both claims and survey data. 23 –25 In 2013, in a study using claims data, 50% of Medicaid-insured, sexually active women aged 15–25 years were tested for chlamydia. 23 Similarly, in a study using NSFG survey data from 2013 to 2019, which provides national estimates for both insured and uninsured individuals, approximately half of the sexually active women aged 15–24 years received STI testing in the previous 12 months. 24
To provide comprehensive estimates from before the COVID-19 pandemic for surveillance, we examine claims for reversible prescription contraceptive services and chlamydia and gonorrhea testing among commercially and Medicaid-insured, sexually active, nonpregnant AYA females in 2018, reporting estimates separately according to insurance type and stratified by age-group (15–19 years and 20–24 years), and further stratified by race/ethnicity in the Medicaid-insured population.
Methods
Data source
For this study, we used IBM MarketScan Research Databases. MarketScan databases include claims for patient-specific utilization of clinical services that capture the full continuum of care for patients. These data, however, do not identify clinical services provided if those services are not billed to insurance. MarketScan databases include fully adjudicated claims from inpatient, outpatient, prescription drug, and carve-out services. 26 The data are derived from a large convenience sample, obtained from large employers, health plans, and government and public organizations. We used the 2018 Commercial Claims and Encounters Database (commercial) and the 2018 Multistate Medicaid Database (Medicaid). 27,28 The commercial database comprises information about employees and their dependents insured by employer-sponsored plans. The Medicaid database comprises pooled health care experience of approximately 7 million Medicaid enrollees from 8 to 12 geographically dispersed states.
Analytic samples
For both databases, the study sample was restricted to enrollees aged 15–24 years who self-reported as female at the time of enrollment into a health coverage plan or Medicaid. In the MarketScan databases, enrollees are classified as either males or females. In addition, to be included in the study, the female enrollees needed to be continuously enrolled each month in 2018 and their outpatient drug claim information had to be recorded in the databases (Fig. 1). Next, the sample was restricted to include only sexually active AYA females based on Health Plan Employer Data and Information Set (HEDIS) specifications. 29 The HEDIS measure identifies sexually active females who are eligible for chlamydia screening. AYA females were identified as sexually active if they had a diagnosis or procedure code in 2018 for Papanicolaou test, pelvic examination, pregnancy or delivery, pregnancy-related service, contraceptive service, infertility-related service, or STI-related service (see Supplementary Table S1 for specific coding). 30 Finally, the sample was restricted to females who were not pregnant anytime in 2018. Demographic information, including gender and race/ethnicity, comes from data suppliers such as employers, health plans, and Medicaid states based on their enrollment information. It is assumed that this demographic information is self-reported by the enrollees when they sign up for coverage or employment. Pregnancy was identified using pregnancy and delivery diagnosis and procedure codes (see Supplementary Table S1 for specific coding). Characteristics of the sample were described by age-group, race/ethnicity (available in Medicaid database only), and region (available in commercial database only). We categorized the sample into two age-groups: 15–19 years and 20–24 years. We used race/ethnicity categories to classify the Medicaid sample as non-Hispanic White, non-Hispanic Black, Hispanic, or non-Hispanic Other enrollees. The MarketScan database does not specify races included in the non-Hispanic Other category. Region is reported as northeast, north central, south, west, and unknown for individuals in the commercial database.
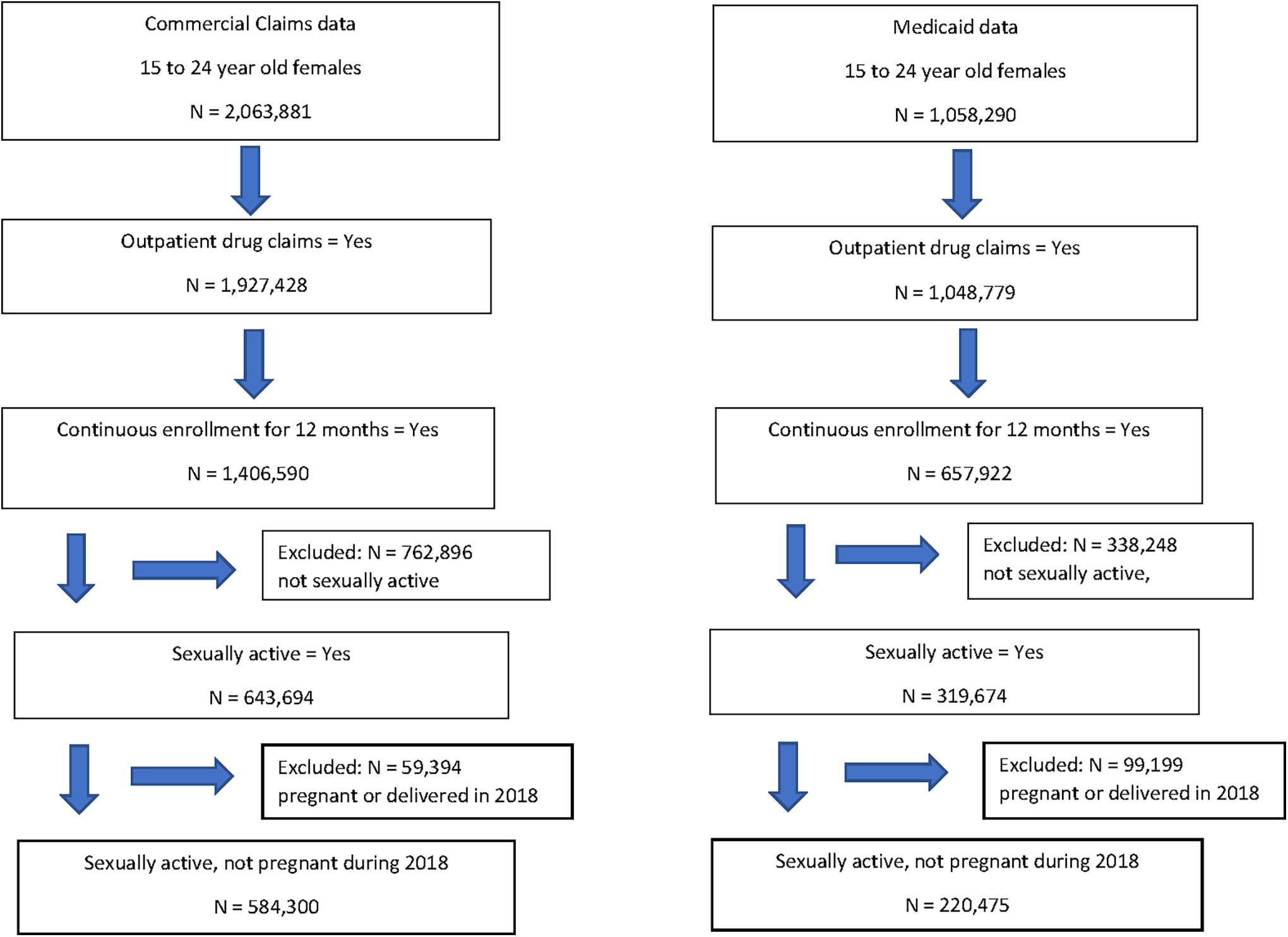
Flowchart showing inclusion and exclusion criteria to create analysis dataset.
Contraceptive and STI testing measures
We identified claims for receipt of services for all reversible prescription contraceptive methods (including IUDs, subdermal implants, injectables, pills, transdermal patches, vaginal rings, and emergency contraception) by female enrollees during 2018 using a combination of International Classification of Diseases-10 diagnosis and procedure codes, Current Procedural Terminology (CPT) procedure codes, Healthcare Common Procedure Coding System (HCPCS) procedure codes, and generic or product names of drugs. 31,32 We identified specific contraceptive methods using the following codes and claims information: encounter for initial prescription, insertion, routine checking, and removal with reinsertion of IUDs; encounter for initial prescription, surveillance, insertion, and removal with reinsertion of implantable subdermal contraceptives; encounter for initial prescription or surveillance of injectable contraceptives; outpatient pharmaceutical claim for COCs; outpatient pharmaceutical claim for POPs; encounter for initial prescription; surveillance or outpatient pharmaceutical claim for vaginal ring or transdermal patch; and outpatient pharmaceutical claim for emergency contraception (see Supplementary Table S1 for specific coding). An individual could have received contraceptive services for more than one method during 2018, and therefore, the results for specific contraceptive services are not mutually exclusive. In addition to measures of services related to specific types of contraceptives, we calculated a composite measure that identified any contraceptive service received. We used a combination of CPT and HCPCS procedure codes to identify screening or testing for chlamydia and gonorrhea (see Supplementary Table S1 for specific coding). 33 Because screening codes and testing codes are the same, we could not distinguish between screening (as part of annual testing) and testing (for a clinical indication) but refer to all as testing in this report. An individual could have received one or more testing claims for chlamydia or gonorrhea but still be counted only once for chlamydia or gonorrhea testing in 2018.
Analysis
We estimated percentage of nonpregnant, sexually active AYA females receiving reversible prescription contraceptive services and chlamydia and gonorrhea testing by age-group in the two databases separately. We calculated estimates by race/ethnicity within each age-group, using Medicaid-insured data. Within each age stratum, Pearson’s chi-squared testing was performed to assess homogeneity in claims across racial/ethnic groups. Data management and analysis were performed using SAS software version 9.4 (SAS Institute, Cary, NC, USA). Statistical significance was determined using a two-side alpha of 0.05 and the Holm–Bonferroni adjustment for multiple comparisons. Because the data are deidentified, the Centers for Disease Control and Prevention deemed this study to be research not involving human subjects and did not require review by an institutional review board.
Results
Our study identified 584,300 commercially insured and 220,475 Medicaid-insured, sexually active, nonpregnant AYA females who were continuously enrolled in 2018. Among the commercially insured, 216,693 (37.1%) were aged 15–19 years, and 367,607 (62.9%) were aged 20–24 years (Table 1). Among the Medicaid-insured, 143,195 (65.0%) were aged 15–19 years, and 77,280 (35.1%) were aged 20–24 years; 48.6% were non-Hispanic White, 40.0% non-Hispanic Black, 1.4% Hispanic, and 3.6% non-Hispanic Other.
AYA females were identified as sexually active if they had a diagnosis or procedure code in 2018 for any of the following, Papanicolaou test, pelvic examination, pregnancy or delivery, pregnancy-related service, contraceptive service, infertility-related service, or sexually transmitted infection-related service.
Females who were not pregnant or had not delivered in 2018.
AYA, adolescent and young adult; NH, non-Hispanic; NA, not available.
Among the commercially insured, sexually active, nonpregnant females, 67.2% of 15- to 19-year-olds and 67.9% of 20- to 24-year-olds had a claim for any reversible prescription contraceptive service (Table 2). Among females aged 15–19 and 20–24 years, 51.9% and 51.7% had claims for COCs, 8.9% and 6.1% for injectable contraceptive services, 5.6% and 7.8% for IUD services, 5.3% and 4.0% for implantable subdermal contraceptive services, 51.4% and 59.5% for chlamydia testing, and 55.6% and 61.6% for gonorrhea testing, respectively.
Percentage of Sexually Active, Nonpregnant Adolescent and Young Adult Females (Aged 15–24 Years) with Claims for Sexual and Reproductive Health Services by Age, Insurance Type, and Race/Ethnicity in IBM MarketScan Commercial Claims and Encounters Database and IBM MarketScan Multistate Medicaid Database, 2018 a
An individual female could have a claim for more than one reversible prescription contraceptive method or more than one type of STI testing in 2018.
At the 0.05 significance level and using the Holm–Bonferroni adjustment for multiple comparisons, all Pearson chi-square tests are statistically significant to assess homogeneity across different race groups.
IUD, intrauterine device; COCs, combined oral contraceptives; NH, non-Hispanic; POPs, progestin-only pills; STI, sexually transmitted infection.
Among Medicaid-insured sexually active nonpregnant females aged 15–19 and 20–24 years, 57.3% and 54.0% had claims for any reversible prescription contraceptive service, 30.7% and 23.3% for COCs, 21.7% and 18.9% for injectable contraceptive services, 3.4% and 7.2% for IUD services, 7.4% and 7.1% for implantable subdermal contraceptive services, 47.2% and 50.5% for chlamydia testing, and 54.7% and 56.0% for gonorrhea testing, respectively.
Among Medicaid-insured, sexually active, nonpregnant females, the percentage with a claim for reversible prescription contraceptive services differed by racial/ethnic group. For those aged 15–19 years, the percentage with a claim for any reversible prescription contraceptive service was 63.4% for non-Hispanic White females, 52.5% for non-Hispanic Black females, and 42.6% for Hispanic females. Among those aged 20–24 years, the percentage with a claim for any reversible prescription contraceptive service was 57.0% for non-Hispanic White females, 50.4% for non-Hispanic Black females, and 56.7% for Hispanic females. Non-Hispanic White females had the highest percentage of outpatient pharmaceutical claims for COCs (37.8% among 15- to 19-year-olds and 27.6% among 20- to 24-year-olds), and non-Hispanic Black females had the highest percentage of claims for injectable services (24.7% among 15- to 19-year-olds and 23.0% among 20- to 24-year-olds). Among 20- to 24-year-olds, Hispanic females had the highest percentage of claims for IUD (11.8%) and implant (10.7%) services. Claims for STI testing differed by racial/ethnic group among the Medicaid-insured. Non-Hispanic Black females had the highest estimates for claims for chlamydia testing (56.3% among 15- to 19-year-olds and 61.1% among 20- to 24-year-olds) and gonorrhea testing (61.6% among 15- to 19-year-olds and 64.9% among 20- to 24-year-olds).
Discussion
This analysis found that, in 2018, about two-thirds of commercially insured and slightly more than half of Medicaid-insured, sexually active, nonpregnant female AYAs had a claim for any reversible prescription contraceptive service. As this study did not obtain estimates on nonprescription contraceptive methods, such as condom, the contraception use among commercially insured and Medicaid-insured, sexually active, nonpregnant female AYAs is underestimated. For both commercially insured and Medicaid-insured AYA females, the most common reversible prescription contraceptive service claim was prescription for COCs. Among the Medicaid-insured, differences in reversible prescription contraceptive service claims were observed by race/ethnicity. Among those aged 15–19 and 20–24 years, the highest estimates for any contraceptive service claims were among non-Hispanic White females. Among those aged 15–19 years, the lowest percentage of contraceptive service claims was among Hispanic females, whereas among those aged 20–24 years, the lowest percentage of contraceptive service claims was among non-Hispanic Black females. Across both commercial and Medicaid insurance, approximately half of sexually active, nonpregnant AYA females had claims for chlamydia and gonorrhea testing, suggesting possible missed opportunities to deliver recommended annual chlamydia and gonorrhea testing or screening. Our study also found chlamydia and gonorrhea testing differed by race/ethnicity among the Medicaid-insured.
Estimates obtained from our analysis are generally in agreement with previously published research. According to research published using the 2017–2019 NSFG data, which relies on self-report, oral contraceptive pills were the most common contraceptive method presently used in the month of interview by women 15–19 and 20–29 years, similar to our claims data study. 19 That study obtained estimates among all women compared with our study, which obtained estimates among sexually active nonpregnant females aged 15–24 years, at any time in 2018. Also in that study, 38.7% of females aged 15–19 years reported present contraceptive use (in the month of interview) in 2017–2019. In contrast, in our study, 67.2% of commercially insured and 57.3% of Medicaid-insured females aged 15–19 years had claims for receipt of any reversible prescription contraceptive service at any time in 2018. Another study using NSFG data from 2006 to 2010 estimated the receipt of any contraceptive service, including checkup for contraceptives, counseling, pregnancy test, or provision of a method or prescription for contraceptives among sexually experienced females aged 15–19 years at 70.2%. 34
Across age strata, differences in claims for receipt of various contraceptive services were observed by racial/ethnic groups. Claims for receipt of COCs were higher among non-Hispanic White females and for receipt of injectable contraception were higher among non-Hispanic Black females, similar to other studies. 35,36 In addition, higher percentages of claims for IUD and contraceptive implant services among Hispanic females aged 20–24 years documented in our study align with NSFG data. 37 These differences in claims may be explained by patients’ preferences and provider behavior. Previous studies indicate differences by race/ethnicity in women’s preferences for different features of contraceptive devices 38 and in attitudes about specific methods 39 that may influence the method ultimately chosen.
Provider knowledge, beliefs, and preferences may affect counseling about contraceptive methods, which may influence the receipt of various contraceptive services. Although a study of clinicians from community health centers concluded that most clinicians offer comprehensive contraceptive counseling and method choice and support AYA patient’s autonomous decision-making, the support of clinicians for higher efficacy methods may conflict with patient choices leading to coercive practices. 16 In addition, provider biases, based on the patient’s race/ethnicity, may lead to coercive practices resulting in improper and inadequate health care. A study that investigated the effect of patient’s race/ethnicity and socioeconomic status (SES) on health care provider recommendations for intrauterine contraception (IUC) concluded that providers perceive a higher risk of an STI in low SES patients compared with high SES patients, resulting in lower likelihood of recommendation for IUC in low SES patients. 17 However, the study also found that low SES Black and Latina women of reproductive age are more likely to have IUC recommended compared with low SES White women. Another recently published study based on individual interviews with 15 health care providers demonstrated how provider bias influences patient interaction and contraceptive counseling. 40 The health care providers attributed challenges of working with diverse patient populations to patients’ race/ethnicity, socioeconomic status, and age. The study concluded that health care adversely influenced by such biases may limit patients’ informed decision-making and autonomy with regard to initiating or continuing contraceptive use. To address coercive practices, the American College of Obstetricians and Gynecologists supports a shared decision-making approach for contraceptive services and access to the full spectrum of contraceptive services for all women. 41 In addition to providing high-quality contraceptive services, attention needs to be provided to multiple socioecological barriers to adolescents’ health care access and utilization such as limited knowledge of and poor previous health care service experiences, cultural and linguistic barriers, structural barriers in health care systems, social stigma, and inadequate insurance coverage. 14
The estimated chlamydia testing prevalence of approximately 50% in this analysis is similar to another analysis using MarketScan Medicaid data among sexually active female AYAs. 23 Our chlamydia testing prevalence is also similar to the overall STI testing in sexually active female AYAs in a recent study using NSFG data from 2013 to 2017. 24 As we cannot differentiate between recommended annual screening and symptomatic testing, this 50% estimate includes both types of testing. Our analysis aligns with several other studies that observed a higher prevalence of chlamydia testing or screening among Black persons compared with other racial and ethnic groups. 18,23 –25 This finding may be explained by racial bias about the greater sexual risk among Black individuals 18 and by the higher rate of chlamydia infection among non-Hispanic Black AYA females. 12 Given the recommendation that all sexually active AYA females be screened for chlamydia and gonorrhea at least once per year, it is important to ensure equitable implementation of screening recommendations, which are for annual screening of all sexually active AYAs regardless of race/ethnicity. 3 Although individuals may choose not to undergo screening, comprehensive counseling about the importance of screening can ensure that AYAs have the information needed when making such decisions. Ensuring that providers receive adequate training about STI testing and screening recommendations and how to conduct sexual risk assessment may help address the missed opportunities. 42
Efforts can support adolescent health care by reducing barriers to access STI-related services. A national study using the 2013–2015 NSFG data found that 12.7% of sexually experienced males and females aged 15–25 years on their parent’s insurance plans would not seek SRH services such as recommended sexually transmitted disease services, chlamydia testing, and sexual risk assessment because of confidentiality issues, including concerns that their parents might find out. 43 Among adolescent males and females aged 15–17 years, this percentage was even higher at 22.6%. Also, receiving a sexual risk assessment in both males and females and chlamydia test in females was higher among 15 to 17-year-olds who had time alone with a health care provider in the past 12 months compared with those who had not. Preservation of confidentiality of sensitive health information in insurance claims process can be promoted at the contract level of the claims process or with statutory or regulatory provisions. 44 Examples of regulatory provisions include providing confidentiality during billing related to minor’s STI services, not providing details on explanation of benefits (EOB) and not sending EOB when no balance is due from the policy holder. States that have adopted billing and insurance claims provisions to protect confidentiality of sensitive information include Connecticut, Delaware, Florida, Hawaii, Maine, New York, Washington, and Wisconsin. 44
A strength of this study is the large size of the databases. The 2018 commercial database includes 27 million enrollees, or approximately 13% of the commercially insured population in the United States, and the Medicaid database includes 11.6 million enrollees, or approximately 20% of the Medicaid-insured population in the United States. 45 However, this analysis has several limitations. First, despite large numbers, the databases are convenience samples, and thus, estimates of claims for contraceptive services and testing for STIs may not be generalizable to commercially and Medicaid-insured U.S. populations. Second, commercial and Medicaid populations are separate and not comparable samples because of potential geographic differences that we could not assess owing to unavailability of geographical data in the Medicaid database and because of differences in medical coverage for SRH services across commercial insurances and Medicaid insurance. Third, to ensure accurate estimation of receipt of services in 2018, we included only those enrollees who were continuously enrolled for all 12 months. As a result, we excluded 27% of the enrollees from the commercial database and 35% of the enrollees from Medicaid database because of gaps in coverage. As factors such as changes in income or the number of individuals in a household affect Medicaid eligibility and therefore enrollment, our analysis did not include experiences of females who had changes in coverage. 46 Fourth, the generalizability of results from the Medicaid database is limited because MarketScan collects Medicaid data from only 8–12 geographically dispersed states. There is varying eligibility by state for enrollment in Medicaid program by the state Affordable Care Act expansion status, varying implementation by states of Section 1115 family planning demonstration waivers, which provide Medicaid coverage for contraceptive services, and varying eligibility by states for Children’s Health Insurance Program, which provides services through Medicaid or separate programs. 47,48 The fifth limitation relates to the identification of sexually active AYA females. The HEDIS measure identifies sexual activity using diagnosis and procedure codes for a set of services as described in the Methods section. 49 If a sexually active AYA did not receive those services in 2018, then the AYA will not be identified as sexually active. Conversely, HEDIS specifications may overestimate the number of sexually active AYAs, as some may receive contraception for other medical indications and may not be sexually active. Sixth, long-acting contraceptives such as IUDs and implants, which are effective for 3–10 years, may not be captured in one year of claims if there are no maintenance codes for these contraceptives in the calendar year. Seventh, enrollees with confidentiality-related concerns might opt to not use their insurance but rather seek services at publicly funded clinics that do not file a claim for insurance purposes (e.g., public health clinics, family planning clinics, school-based clinics, or Title X clinics) where services are provided at no or low cost, 50 which may underestimate the proportion who received these services. Younger women (AYAs), lower-income women, racial and ethnic minorities (e.g., non-Hispanic Black and Hispanic females), foreign-born women, women with Medicaid coverage, and women who are uninsured are more likely to rely on publicly funded clinics for contraceptive services compared with other groups of women. 50 Eighth, Medicaid-insured Hispanic AYAs in our study may not be representative of the Medicaid-insured Hispanic AYAs in the population because the proportion in our study is small when compared with the proportion of Hispanic adults aged 18–64 years with a public health coverage such as Medicaid, CHIP, state-sponsored, or other government-sponsored health plan, Medicare, and military plans. 51 Ninth, because race/ethnicity information is not available in the commercial database, we could not examine the receipt of SRH services by race/ethnicity in these data. Tenth, certain claims such as outpatient prescription claims for COCs, POPs, emergency contraception, and vaginal ring or transdermal patch may not translate to use of these contraceptives. Finally, our study estimated claims for reversible prescription contraceptive services and did not track nonprescription methods, such as condom use, which is the most used method by adolescents and can also prevent STIs. 52
In summary, in 2018, approximately two-thirds of commercially insured and slightly greater than half of Medicaid-insured, sexually active, nonpregnant AYA females had a claim for reversible prescription contraceptive services. Among the Medicaid-insured, differences exist by race/ethnicity. Among 15- to 19- and 20- to 24-year-olds, the highest percentages of any claims for reversible prescription contraceptive services were observed among non-Hispanic White females. Among female aged 15–19 years, the lowest percentages were observed among Hispanic females and among 20- to 24-year-olds, lowest percentages were observed among non-Hispanic Black females. Among Medicaid-insured, chlamydia and gonorrhea testing differed by race/ethnicity, with non-Hispanic Black females having the highest percentages of claims. These differences by race/ethnicity may be attributable to disparities in access and utilization resulting from factors such as socioecological barriers, structural and individual racism, and provider biases. Approximately half of sexually active female AYAs were screened for chlamydia and gonorrhea in 2018. These findings suggest potential missed opportunities for recommended STI testing or screening among commercially and Medicaid-insured AYAs. Providers can implement strategies to ensure that opportunities to offer SRH services to AYAs in the clinic setting are not missed by implementing recommended services and youth-friendly practices, for example, routine sexual health assessment, providing the full range of contraceptive methods and in-depth counseling, providing education geared to adolescent’s level of development, ensuring time alone with the provider to support confidentiality, and providing social support. 53 –55 Future analysis may include the use of claims databases such as MarketScan for surveillance of contraceptive services and STI testing during the COVID-19 pandemic and post-COVID-19 pandemic. In addition to claims databases, future analyses may also use complex surveys such as NSFG to monitor access and utilization of SRH services and to explore associations between exposures such as SRH-related health education and receipt of SRH services.
Implications and Contributions
Race/ethnicity data were available for sexually active, nonpregnant, Medicaid-insured females aged 15–24 years, and there were differences in claims for reversible prescription contraceptives and chlamydia and gonorrhea testing by race/ethnicity. Only half of commercially and Medicaid-insured had claims for chlamydia and gonorrhea testing, suggesting missed opportunities for recommended services.
Footnotes
Authors’ Contributions
A.D.K. conceptualized and designed the study, carried out the analyses, drafted the initial article, and reviewed and revised the article. N.T. conceptualized and designed the study, reviewed and revised the article, and critically reviewed the article for important intellectual content. C.G.P. conceptualized and designed the study, reviewed and revised the article, and critically reviewed the article for important intellectual content. M.M. conceptualized and designed the study, assisted with the analysis, reviewed and revised the article, and critically reviewed the article for important intellectual content. H.D.T. conceptualized and designed the study, reviewed and revised the article, and critically reviewed the article for important intellectual content. A.W.B. conceptualized and designed the study, reviewed and revised the article, and critically reviewed the article for important intellectual content. M.W. conceptualized and designed the study, reviewed and revised the article, and critically reviewed the article for important intellectual content. E.H.K. conceptualized and designed the study, reviewed and revised the article, and critically reviewed the article for important intellectual content. All authors approved the final article as submitted and agree to be accountable for all aspects of the work.
Disclaimer
The findings and conclusions in this report are those of the authors and do not necessarily represent the official position of the Centers for Disease Control and Prevention.
Author Disclosure Statement
The authors have no financial relationships relevant to this article to disclose.
Funding Information
This work was completed as part of routine work conducted by government employees.