
Abstract
Objective:
Limited population-based data examines racial disparities among pregnant and postpartum Veterans. Our objective was to determine whether Black/white racial disparities in health care access, use, and Veteran and infant outcomes are present among pregnant and postpartum Veterans and their infants using Veterans Health Administration (VA) care.
Methods:
The VA National Veteran Pregnancy and Maternity Care Survey included all Veterans with a VA paid live birth between June 2018 and December 2019. Participants could complete the survey online or by telephone. The independent variable was self-reported race. Outcomes included timely initiation of prenatal care, perceived access to timely prenatal care, attendance at a postpartum check-up, receipt of needed mental health care, cesarean section, postpartum rehospitalization, low birthweight, preterm birth, admission to a neonatal intensive care unit, and breastfeeding. Nonresponse weighted general linear models with a log-link were used to examine associations of race with outcomes. Cox regression was used to examine the association of race with duration of breastfeeding. Models adjusted for age, ethnicity, urban versus rural residence, and parity.
Results:
The analytic sample consisted of 1,220 Veterans (Black n = 916; white n = 304) representing 3,439 weighted responses (Black n = 1,027; white n = 2,412). No racial disparities were detected for health care access or use. Black Veterans were more likely than white Veterans to have a postpartum rehospitalization (RR 1.67, 95% CI: 1.04–2.68) and a low-birthweight infant (RR 1.67, 95% CI: 1.20–2.33).
Conclusion:
While no racial disparities were detected for health care access and use, we identified disparities in postpartum rehospitalization and low birthweight, underscoring that access is not sufficient for ensuring health equity.
Introduction
Racial disparities in pregnancy care and outcomes in the U.S. are well documented. 1 –5 Compared with white people, Black people are less likely to have timely prenatal care (initiated before 13 weeks gestation), less likely to have a vaginal birth versus a cesarean section, less likely to breast/chestfeed, and more likely to experience postpartum depression. 1 –5 As a result of such inequities, there are stark racial disparities in pregnancy-related mortality, with Black and American Indian/Alaska Native (AI/AN) birthing people having two and three times higher maternal mortality rates than white birthing people. 6 –8 Collectively, racial disparities in access to care and outcomes reflect the cumulative impact of current and historical racism, including policies and practices that directly or indirectly limit access to resources and health care. 9 –11
Racial disparities in perinatal care access and subsequent outcomes are of particular concern for the Veterans Health Administration (VA) as it cares for a rapidly growing group of young Veterans, among whom Black individuals are overrepresented relative to the nonveteran population. 12 –14 The most recent data show 25% of VA-covered births are by Veterans who identified as Black or African American (hereafter referred to as Black), compared with ∼15% of all births in the U.S. 12,13,15 VA pregnancy benefits cover perinatal care, including prenatal, birth, and postpartum care and have been part of the VA medical benefits package for eligible Veterans since 1996, with demand for this care increased ∼14-fold between 2000 and 2015. 13,16,17 Nearly all Veteran perinatal care is purchased by VA from non-VA community providers, although Veterans may continue to see VA providers throughout pregnancy for other types of medical care (e.g., mental health). 18 –20 To ensure that pregnant and postpartum Veterans get the care they need and to address challenges related to navigating multiple health care systems, VA has invested in maternity care coordination.
Nevertheless, Black pregnant Veterans are exposed to and impacted by the same racist systems and practices that their nonveteran peers are exposed to across the life course, including throughout pregnancy and birth. 9,21 –24 Therefore, it is perhaps not surprising that emerging evidence suggests some of the same racial disparities observed among the U.S. general population may be present among pregnant service members and Veterans. 25 –29
As a learning health care system, VA requires data to inform policy and program development and to achieve health equity among Veterans using VA pregnancy benefits. 30,31 However, to date, limited population-based data are available to assess racial disparities in health care access, use, and Veteran and infant outcomes among those using VA pregnancy benefits. Therefore, the objective of this analysis was to determine whether Black/white racial disparities in health care access, use, and outcomes are present among pregnant and postpartum Veterans and their infants using VA care in a population-based sample. We hypothesized that racial disparities in health care access and use might be minimized due to the maternity care coordination program and based on evidence from studies indicating that racial disparities in process measures are frequently reduced or eliminated within VA. 32 We further hypothesized that we would still observe racial disparities in Veteran and neonatal outcomes.
Methods
Survey development
The VA National Veteran Pregnancy and Maternity Care Survey (VETPRAMS) was developed based in part on the U.S. Centers for Disease Control and Prevention (CDC) Pregnancy Risk Assessment Monitoring System (PRAMS) survey. 33 VETPRAMS adapted questions from CDC PRAMS for measuring health, health behaviors, and outcomes. Additionally, a series of questions were developed to assess care access and barriers, specifically to prenatal care, mental health care, physical therapy, medications, medical supplies, and postpartum care. 34 –36 These questions specifically addressed different domains of access both in terms of prevalence of access barriers and to what extent barriers prevented access. The initial survey instrument was piloted among 60 Veterans in Washington, Oregon, and Idaho before finalizing. Based on pilot data and feedback from participants and interviewers, minor changes to question wording and order were made.
The majority of these changes were to the questions related to access domains. For example, we changed the question, “Did you have difficulty getting prenatal care appointments at convenient times?” to be more specific, “Did you have difficulty getting prenatal care appointments at times when you did not have work, school, or family responsibilities?”
VETPRAMS study population and participants
The sample for VETPRAMS included all Veterans with a VA paid live birth from June 2018 to December 2019 who were no more than 18 months postpartum at the time of recruitment. The sample was constructed using discharge data from the VA Corporate Data Warehouse (CDW), which includes administrative records for all VA paid or provided care. VA paid births were identified using a previously refined and validated algorithm that relies on International Classification of Disease codes, Tenth Revision (ICD-10) and Diagnosis-Related Group (DRG) codes. 37 –39 Veterans with a code consistent with an inpatient stay for childbirth during the study time frame (ICD-10: Z37.0, Z37.2, Z37.9, Z37.50-Z37.54, Z37.59, O60-O77, O80-O82; DRG: 765, 766, 774, 775, 767, 768) were eligible for inclusion. We excluded those who were identified as not Veterans; who had died; those whose sex in the electronic health record was not female; and those whose age was listed as less than 18 years old, 50 years or older, or missing; who had a flag indicating that the address listed in CDW was no longer active; or whose pregnancy did not result in a livebirth (ICD-10: Z37.1, Z37.3–4, Z37.60–4, Z37.69, Z37.7).
Many patients use VA on an ongoing basis, and so an individual patient may have given birth more than once during our 18-month study time frame; however, the sample was restricted to include only the most recent birth discharge date during the study time frame.
Potential participants were mailed a recruitment packet that contained an invitation explaining the nature of the project and provided contact information for answering questions about the study, an information sheet addressing the essential elements of informed consent, a prepaid opt-out card, and a letter of endorsement from the head of the VA's Office of Women's Health (OWH) designed to assure all potential recipients of the legitimacy of the study and its relevance to VA's efforts to improve care for women Veterans. Additionally, study invites included an individual URL (survey link) and instructions for online completion by the participant and a dedicated 800 number for opting out of or providing a time for scheduling an interview, if they preferred to complete the survey by phone. Two weeks after the initial packet was sent, a second identical packet was sent to those who had not completed the survey online, completed a telephone interview, or opted out (i.e., nonresponders) and again, 2 weeks later, a third packet was sent to nonresponders. Twenty-one days after the initial mailing, interviewers had made up to 12 attempts to contact a potential participant by phone, including up to three voicemails.
If, after the 12th attempt, contact was not made, a Veteran was considered a nonresponder. Participants received a $15 gift card upon completing the survey. All study procedures were approved by the VA Puget Sound and VA Greater Los Angeles Institutional Review Boards.
A total of 4,000 Veterans were selected for participation in VETPRAMS; Figure 1 shows exclusions and our final analytic sample. Among those reached, VETPRAMS had a response rate of 58.4%. For purposes of the primary analysis, we excluded an additional 185 respondents who did not self-identify as Black or white race. Our final analytic sample consisted of 1,220 Veterans (Black n = 916; white n = 304) representing 3,439 weighted responses (Black n = 1,027; white n = 2,412; see below for details on weights) and was ∼30% of those in the original sample.
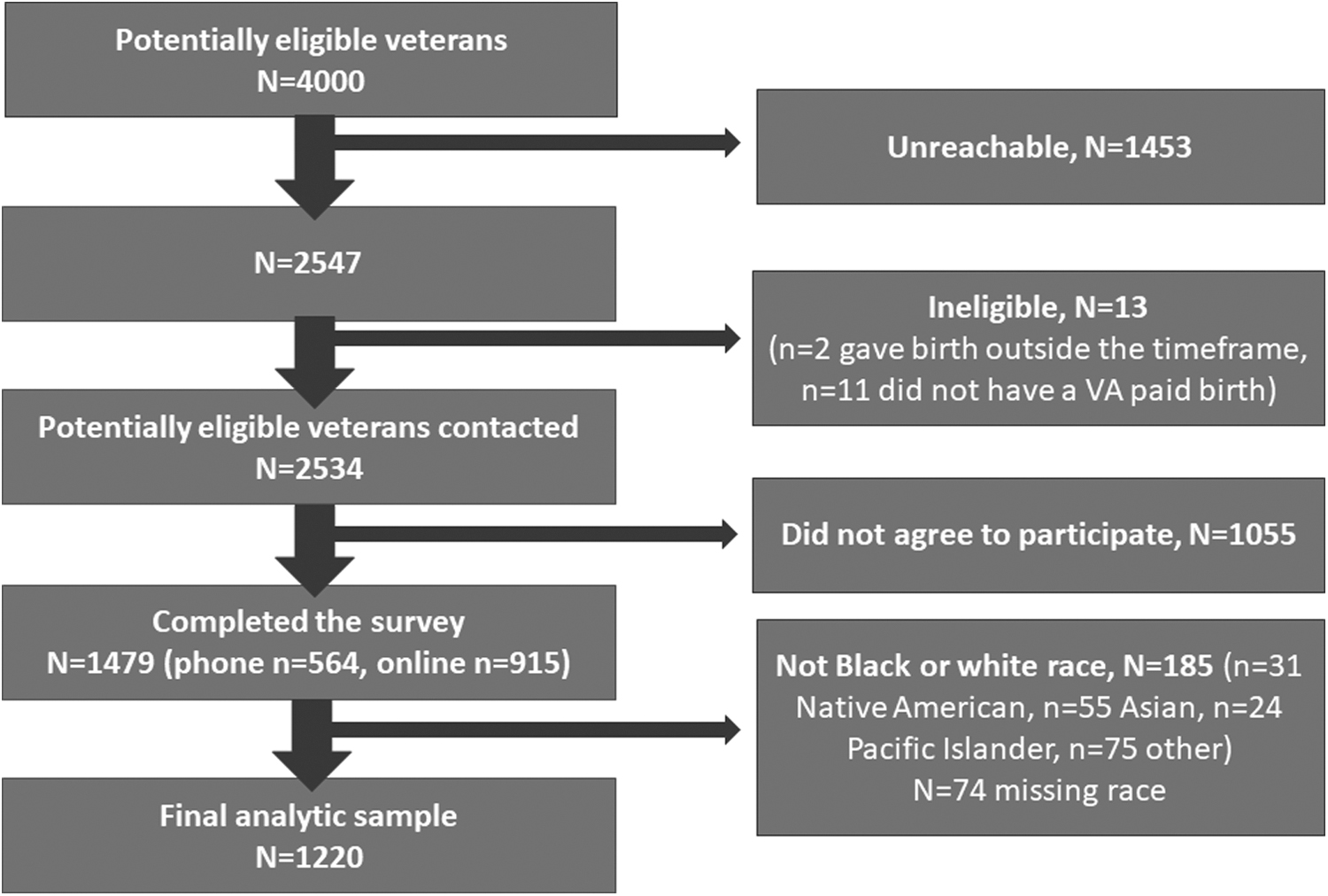
Survey response, exclusions, and final analytic sample.
Study measures
The primary independent variable was self-reported race. Participants were asked to indicate which of the following best represented their race [1] white, [2] Black or African American, [3] American Indian or Alaska Native, [4] Asian, [5] Pacific Islander, or [6] Other. Due to the relatively small numbers of participants identifying as American Indian/Alaska Native, Asian, Pacific Islander or Other, we excluded these participants from this analysis and dichotomized race as Black or white (Supplementary Table S1 for outcomes among those excluded). Self-reported ethnicity was assessed as a separate variable independent of race.
Dependent variables included self-reported access to and use of health care during and after pregnancy and clinical outcomes for the birthing Veteran and their infant. Access to and use of pregnancy-related care was operationalized as three outcomes: (1) timely initiation of prenatal care (initiation before 13 weeks gestation, yes/no), (2) perceived access to timely prenatal care (whether or not a participant got prenatal care as early in their pregnancy as they would have liked, yes/no), and (3) attendance at a postpartum check-up (yes/no). Given the high prevalence of mental health conditions documented among pregnant Veterans using VA pregnancy benefits, we also sought to measure access and use of mental health care during pregnancy. 40 –43 Participants were asked whether they needed mental health care during their pregnancy (yes/no). Those who answered yes were then asked where they received mental health care during pregnancy. Responses included combinations of VA and VA-paid care, non-VA care, and not getting the mental health care they needed. This was dichotomized into receipt of needed mental health care (yes/no) regardless of source of care.
Clinical outcomes for the Veteran and their infant were self-reported and included cesarean section, postpartum rehospitalization, low birthweight, preterm birth, admission to a neonatal intensive care unit (NICU) after birth, and breastfeeding. Participants were asked to indicate whether they gave birth vaginally or by cesarean section. In keeping with ongoing efforts to monitor and reduce cesarean section rates among low-risk nulliparous pregnancies, we also asked about parity and if this was their first cesarean section. 44,45 We then examined rates of primary cesarean, or first cesarean regardless of parity. 45 Postpartum rehospitalization was defined as having had any medical problems that caused them to go to the hospital and stay overnight in the 12 months following the birth of their infant (yes/no). Participants reported their infants' birthweight in grams or pounds and ounces. Low birthweight was defined as birthweight of <2,500 g or <5 lbs 8 ounces. Preterm birth was defined as birth before 37 weeks completed of gestation based on self-reported due date and Veteran discharge date for birth hospitalization.
NICU admission was defined based on asking participants whether their infant was put in an intensive care unit after birth. Breastfeeding was examined in terms of ever versus never breastfeeding and duration. Participants were asked if they had ever breastfed or pumped breast milk to feed their infant (yes/no). Those answering in the affirmative were then asked whether they were currently breastfeeding or pumping breast milk to feed their infant. For those currently breastfeeding, we estimated the duration of breastfeeding to be the difference between the date of their discharge for childbirth to the date of survey completion. Among those who had discontinued breastfeeding by the time of the survey, we further asked how many months or weeks they had breastfed. All responses were converted to months before analysis.
For purposes of describing our sample, we included variables on demographics, pregnancy history, and survey timing. Veteran's age at the time of birth was categorized as 20–24 years old, 25–34 years old, and 35+ years old. Participants were asked separately about Hispanic or Latina or Spanish ethnicity, which was dichotomized (yes/no). Rural residence was defined based on matching individual Federal Information Processing System codes for county of residence with rural/urban continuum codes. 46 Participants were also asked about their employment status (employed/self-employed, unemployed, homemaker, student, retired, unable to work), highest level of education (high school, college 1–3 years, associates/trade school, college 4 years, graduate school), and self-reported parity (primiparous, 2–3, 4+). Finally, we estimated time from birth to survey completion (weeks).
Statistical analyses
We used VA records from the original study sample of 4,000 Veterans who used VA pregnancy benefits to construct nonresponse weights using inverse probability weighting with sociodemographic, clinical, and administrative variables accessible in CDW. 47 One-hundred twenty data elements were used to create the nonresponse weights. All analyses used the resulting weights to account for nonresponse and all descriptive results report weighted percentages.
We first compared outcomes descriptively between Black and white Veterans. Weighted Ns and percentages are reported for categorical outcomes and weighted median and interquartile range is reported for breastfeeding duration (weeks). General linear models with a log-link and Poisson error distribution were then applied separately to examine associations of race with categorical outcomes. Cox regression was used to examine the association of race with duration of breastfeeding. Models adjusted for age (years), urban versus rural residence, and parity, as these were a priori expected to be associated with race and predictors of the evaluated outcomes. We present relative risks (RR) and hazard ratios (HR) with 95% confidence intervals (95% CI) from unadjusted models and adjusted models. All statistical tests used an alpha level of 0.05. All analyses were completed using Stata 16.1.
Results
Overall, 60% of Veterans in our cohort were 25–34 years old, 12.9% identified as Hispanic/Latina/Spanish ethnicity, the majority were urban dwelling, and nearly half were employed either for wages or self-employed (Table 1). A little over one third of Veterans using VA pregnancy benefits were nulliparous. The median time between giving birth and completing the survey was just over a year (58.4 weeks). Age distribution, education, and time between birth and survey completion did not vary between racial groups. White Veterans tended to be more likely than Black Veterans to live in a rural area (18.3% vs. 6.7%). Notably, a higher percentage of Black Veterans than white Veterans reported being unemployed (14.2% vs. 6.5%). Finally, Black Veterans were less likely than white Veterans to be nulliparous (28.5% vs. 38.8%).
Characteristics of Black and White Veterans with Births Paid for by VA, June 2018 Through December 2019
With respect to access and use of pregnancy-related health care, unadjusted percentages indicated slightly lower access and use among Black versus white Veterans, however, none of these differences was statistically significant after adjusting for age, rurality, and parity (Table 2). Approximately a third of Black and white Veterans reported needing mental health care during pregnancy. Regardless of race, of those who reported needing mental health care during pregnancy, ∼20% indicated they did not receive such care.
Access and Utilization of Health Care During Pregnancy and Postpartum Among Black and White Veterans with Births Paid for by VA, June 2018 Through December 2019
Relative risk (RR) adjusted for parity, urban versus rural residence, and age (years) with Black race as the referent category.
Among those with a self-reported need for mental health care during pregnancy.
In terms of birth outcomes, unadjusted percentages indicated that Black Veterans and their infants had slightly worse outcomes relative to white Veterans and their infants (Table 3). After adjustment for age, rurality, and parity, Black Veterans were 67% more likely than white Veterans to have a postpartum rehospitalization (RR 1.67, 95% CI: 1.04–2.68) and 67% more likely to have a low-birthweight infant (RR 1.67, 95% CI: 1.20–2.33). No other racial disparities in outcomes for birthing Veterans or their infants were detected in our adjusted models.
Birthing Veteran and Infant Outcomes Among Black and White Veterans with Births Paid for by VA, June 2018 Through December 2019
Relative risk (RR) or hazard ratio (HR) adjusted for parity, urban versus rural residence, and age (years) with Black race as the referent category.
p < 0.05.
p < 0.001.
Discussion
Our study provides the first population-based estimates examining Black/white racial disparities in care access, use, and outcomes among Veterans and their infants using VA care. No statistically significant racial disparities in access or use of care during the perinatal period were detectable; nevertheless, Black Veterans were more likely than white Veterans to experience postpartum rehospitalization and to have a low-birthweight infant. These two disparities persisted even after adjustment for age, parity, and rurality.
The failure to detect a statistically significant difference by race in access to and use of health care during the perinatal period is consistent with prior literature indicating that for many process measures, racial disparities observed outside VA are reduced or eliminated within VA. 32 In fact, our estimates indicate that timely prenatal care was more frequent among Veterans using VA pregnancy benefits than among the general population both overall and by race (Total: ∼85% vs. nonveterans 78%; Black: Veterans 84.1% vs. nonveterans 67.6%; white: Veterans 86.6% vs. nonveterans 82.8%). 48
Notably, nearly half of all births in the U.S. are paid for by Medicaid and those with Medicaid-paid births are less likely to receive timely prenatal care than those with private insurance or Veterans with VA-paid births. 49 Veterans with VA-paid births benefit from continuous health care coverage before, during, and after pregnancy, as well as programs VA has developed to address social and care coordination needs. These may reduce barriers to access and use of prenatal care and increase equity. Our findings regarding perceived timely access to prenatal care are in contrast to those of Mattocks, et al., who detected Black/white disparities in perceived timeliness of prenatal care in a convenience sample. 50
Overall, approximately three quarters of participants in both studies reported perceived timely access to prenatal care; however, in the present study the percentage of Black Veterans reporting perceived timely access to prenatal care was slightly higher than that reported by Mattocks, et al. Differences in our findings may be due to variations between studies in sampling (convenience vs. population based), study recruitment period, and statistical methods.
Given the high burden of mental health conditions experienced by women Veterans and particularly those using VA pregnancy benefits, we examined perceived need for mental health care and receipt of needed care. 41 No racial differences in perceived need or receipt of mental health care were detected. The percentage of Veterans who reported receiving needed mental health care during pregnancy was higher than that reported in the general population (∼50%), and suggests the success of VA's continued investment in mental health care for all Veterans and specialized programs such as the VA Maternity Care Coordination Program. 51,52 Nevertheless, one in five Veterans in our study were unable to access needed mental health care indicating there may be a persistent unmet need for perinatal mental health care. Prior research suggests that Veterans with no mental health diagnosis or treatment before pregnancy who experience new onset of symptoms may be at high risk of not receiving needed care. 19,53
Untreated depression, anxiety, or posttraumatic stress disorder in pregnancy is associated with a range of negative consequences for the pregnant person and their infant, and continued efforts are needed to ensure all Veterans in VA have access to perinatal mental health care. 38,54 –56 Continued refinement of screening tools, timing, and referral processes in addition to the recent introduction of the Reproductive Mental Health Consultation telephone program will hopefully help to ensure that pregnant Veterans get the mental health care they need. 42,57
Although our unadjusted findings suggested small-to-moderate racial disparities across some measured birth outcomes, adjusted models only detected racial disparities in postpartum rehospitalization and low birthweight. Racial disparities in postpartum rehospitalization and low birthweight have previously been described in the general U.S. population. 58,59 Our postpartum rehospitalization findings are particularly concerning due to the racial disparity, and as the percentage of Veterans in our study reporting a postpartum rehospitalization (6.5%–10%) is much higher than that reported in the U.S. population, which ranges from 1% to 2.15%. 58,60 This may reflect the higher comorbidity of pregnant VA users compared with pregnant people in the community and our use of a longer time period (12 months vs. 30 days). 58 Findings also raise concerns about risk for pregnancy-related morbidity and mortality among Veterans using VA pregnancy benefits, as among nonveterans nearly half of all deaths among pregnant and birthing people in the U.S. occur between 43 days and 1 year postpartum with the leading causes of death being heart and mental health conditions. 61,62
To date, no data on maternal mortality among Veterans have been published. Given these concerns, continued efforts to ensure care coordination during pregnancy and reintegration into VA health care postpartum are needed. The VA Maternity Care Coordination program is currently expanding to include a full year postpartum. The racial disparity in low birthweight that we detected among Veterans using VA pregnancy benefits is consistent with prior findings among Veterans and nonveterans: among Veterans both racial groups in our study had slightly higher prevalence of low birthweight than the nonveteran population (Veterans: 16.2% Black vs. 10.5% white; U.S. population: 14.2% Black vs. 6.8% white). 63,64 Interestingly the Black/white disparity in prevalence of low birthweight was smaller among Veterans. 39,64
Strengths of this VETPRAMS analysis include use of population-based sample, comprehensive adjustment for nonresponse, and incorporation of some previously validated survey questions and relatively large sample size. Nevertheless, our findings must be considered in the context of several limitations, including self-reported outcomes with the potential for reporting bias. Importantly, self-report has demonstrated good validity for the majority of the clinical outcomes we included in our study such as cesarean section, birthweight, gestational age at birth, and NICU admission, and the overall frequency of these outcomes is consistent with prior research that used hospital discharge data. 65 –68 Also, while accuracy of self-report might vary over time, weeks between giving birth and completion of the survey did not vary by race, and therefore, we would not expect this form of recall bias to impact estimates of racial disparities. Additionally, by adjusting for nonresponse, we may have reduced potential selection bias in which factors, such as mental health diagnoses that increase risk of adverse pregnancy outcomes, might also influence likelihood of participation.
However, only the birthing Veterans' data were available to us as linkage with infant medical record data were not possible. Furthermore, the survey asked specifically about racial identity from the perspective of the respondent, did not include an option to check more than one race, and did not include questions regarding how their racial identity was perceived by others, including clinicians. 69 Thus, while this study provides important basic descriptive data, our conceptualization of race is a limitation that precludes detailed examination of how the complexities of racism shapes access, experiences, and outcomes of health care for pregnant Veterans. 69 While our sample size was relatively large compared with other studies of pregnant Veterans, which relied on survey data, we still may have been underpowered to detect racial disparities in some outcomes. For example, the observed nonsignificant adjusted relative risk (aRR) for preterm birth of 1.34 (0.9–2.0) is comparable with prior findings from a larger VA birth cohort analysis in which this disparity was statistically significant for Black versus white Veterans (adjusted odds ratio 1.49, 1.29–1.71). 38
Finally, our data were collected before the COVID-19 pandemic, which engendered rapid changes in health care, and the passage of the Protecting Moms Who Served Act, which provides additional support for VA care for pregnant Veterans. Therefore, we cannot examine these impacts with our data. Thus, our findings provide important baseline data for any future efforts to evaluate the impact of the pandemic and the Protecting Moms Who Served Act on access to care and outcomes among pregnant Veterans in VA.
Conclusions
Overall, our analysis of the VETPRAMS survey found that pregnant VA users have high rates of prenatal access, consistent with an older claims-based analysis. 49 Racial disparities in U.S. pregnancy care access and use were minimal in the Veterans surveyed, suggesting that some of the structures in VA are effective at reducing racial disparities in health care access. Nonetheless, we identified Black/white disparities in postpartum rehospitalization and low birthweight. Cumulatively, our findings underscore the idea that access is necessary but not sufficient for ensuring health equity. Future policies and programs should continue to strengthen perinatal mental health care access and services for all pregnant and postpartum Veterans, and future research should consider a life-course perspective, partnering with community-based organizations to ensure Black Veterans have access to culturally competent continual support throughout all stages of pregnancy. 70 –72
Footnotes
Acknowledgments
The authors would like to thank all the Veterans who contributed to this study through participation in our survey. The views expressed herein are those of the authors and do not necessarily reflect the position or policy of the Department of Veterans Affairs or the U.S. government.
Authors' Contributions
J.G.K.: conceptualization (lead), funding acquisition (lead), methodology (lead), and writing—original draft (lead); A.S.B.: conceptualization (equal), data curation (co-lead), formal analysis (lead), and writing—reviewing and editing (equal); E.V.T.: project administration (lead), and writing—reviewing and editing (equal); D.A.E.: writing—reviewing and editing (equal); K.O.H.: visualization (lead), and writing—reviewing and editing (equal); A.M.J.: writing—reviewing and editing (equal); E.W.M.: conceptualization (equal), project administration (equal), and writing–reviewing and editing (equal); D.S.: writing—reviewing and editing (equal); J.G.S.: writing—reviewing and editing (equal); J.T.-S.: writing—reviewing and editing (equal), data curation (co-lead), and software (lead); E.M.Y.: funding acquisition (equal), and writing—reviewing and editing (equal); D.L.W.: conceptualization (equal), methodology (equal), and writing—reviewing and editing (equal); and A.Y.C.: writing—reviewing and editing (equal).
Author Disclosure Statement
The authors have no conflicts of interest to disclose.
Funding Information
Dr. Katon was supported by a VA Health Services Research & Development (HSR&D) Career Development Award [grant number 13-266], a VA HSR&D Services Directed Research Award [SDR 19-325], the VA Office of Women's Health, and the VA HSR&D Center of Innovation for Veteran-Centered and Value-Driven Care. Dr. Bossick was supported by grant number T32HS013853 from the Agency for Healthcare Research and Quality. Dr. Yano was supported by a VA HSR&D Senior Research Career Scientist Award (grant number RCS 05-195).
Supplementary Material
Supplementary Table S1
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.