
Abstract
Background:
Cardiovascular disease is the leading cause of mortality for women and men. Prior studies have demonstrated the underrepresentation of women in published clinical trials, but no study to date has assessed inclusion of women in late-breaking clinical trials (LBCTs) presented at national meetings. The objective is to characterize the inclusion of women participants in LBCT presented at the 2021 American College of Cardiology (ACC), American Heart Association (AHA), and European Society of Cardiology (ESC) annual meetings and identify trial characteristics associated with improved inclusion.
Methods:
LBCT presented at the 2021 ACC, AHA, and ESC meetings were identified and the inclusion of women as participants was assessed. The inclusion to prevalence ratio (IPR) was calculated by dividing the percentage of women participants by the percentage of women in the disease population. IPRs <1 indicate underenrollment of women. Of the 68 LBCT, 3 trials were excluded due to lack of subject matter relevance.
Results:
Inclusion of women ranged from 0% to 71%. Only 47.1% of trials reported sex-specific analyses. The average IPR was 0.76 for all trials and did not vary based on conference, trial center, geographic region, or funding source. The average IPR varied based on subspecialty, with a statistical difference between interventional cardiology and heart failure (0.65 vs. 0.88, p = 0.02). The average IPR was significantly lower for procedural studies compared with medication trials (0.61 vs. 0.78, p = 0.008), as well as for studies with mean age <65 and trial size <1500 participants. There was no difference in IPR based on female authorship.
Conclusions:
LBCT can impact novel drug and device approval, intervention indications, and patient management. Nonetheless, most LBCT underenroll women, particularly, procedural LBCT. In 2021, sex-based enrollment disparities persist, highlighting the need to engage key stakeholders, including funding organizations, national governing bodies, editorial board members, and medical societies, in the creation of a coordinated strategic initiative to advance gender parity. These findings warrant further investigation to increase inclusion of women in trials, including potential enrollment requirements for consideration as LBCT by meeting organizers.
Introduction
Cardiovascular disease (CVD) is the leading cause of death among both women and men, yet the inclusion of women in clinical trials remains suboptimal. 1,2 Meaningful sex-based differences in symptomatology, pathophysiology, and clinical outcomes of CVD have been demonstrated. 3 A dearth of sex-specific data as it pertains to women and CVD persists, making risk–benefit decisions with regard to drug, device, and behavioral interventional therapies uncertain and limit the application of novel therapies. 4,5 As such, the federal organizations, including the National Institutes of Health and the U.S. Food and Drug Administration, have mandated demographic analyses and proposed a coordinated approach to the inclusion of women via the Health of Women Program Strategic Plan, resulting in an increase in the inclusion of women and minority populations in clinical trials, as well as more sex-specific analyses of results. 6
However, prior research has suggested that women remain underrepresented in clinical trials, particularly in trials that address device-based therapies, coronary artery disease, and heart failure. 7 –9 A recent analysis suggested that on average, individuals who identify as women make up about 25% of major clinical trials evaluating drug-eluting stents, ventricular assist devices, implantable cardioverter defibrillators, and cardiac resynchronization defibrillators. 10 Other studies have found that relative to the prevalence in the disease population, women have been more adequately enrolled in trials of hypertension and pulmonary artery hypertension, as compared with arrhythmia and heart failure trials. 1 Similar trends have been identified in other medical subspecialties, including neurology, as well as in gastroenterology. 11 –13
Among clinical trials, inadequate enrollment, trial retention, and sex-specific reporting are particularly prominent in interventional and device-based trials. 14,15 Late-Breaking Clinical Trials (LBCTs) at national conferences garner wide publicity and dissemination, often being advertised prominently to attendees as the most cutting-edge, highly-anticipated science of the year and being presented on the main stage at flagship conferences. LBCT are frequently highlighted in subsequent publications, including review articles summarizing high-impact trials from major conferences, reaping additional notice. 16,17 However, the representation of women in high-impact trials presented at major cardiovascular conferences remains unknown. This analysis seeks to characterize the inclusion of women in the LBCT at three major cardiovascular meetings to better understand current barriers to enrollment, reporting, and retention.
Methods
Data source
We identified 68 LBCT presented at the 2021 American College of Cardiology (ACC), European Society of Cardiology (ESC), and American Heart Association (AHA) annual meetings. Accompanying published articles were additionally reviewed if the date of publication occurred before December 1, 2021 (n = 39/68). Data were extracted from the abstract only if the full article was not published before this deadline. Studies were identified via the electronic conference portal and presentations were downloaded from the online portal. Accompanying published articles available at the time of analysis were identified through individual journal web portals. Three studies were excluded from the analysis (one meta-analysis; one prostate cancer trial; one breast cancer trial).
Variables
Characteristics of trials collected included subspeciality, type of intervention, geographic region of study, funding source, and authorship data. Participant characteristics, including total participants, median age, gender, and racial/ethnic distribution, were collected. Authorship data were collected, including total number of authors; number of female-identifying authors in the author block; and gender of first, last, and presenting authors. The gender of first, last, and presenting authors were characterized on the basis of publicly available biographic data.
An inclusion to prevalence ratio (IPR) was calculated: (percentage of women participants in each trial)/(percentage of women within disease population), based upon recent combined U.S. and global statistics (Table 1). 18,19 Denominators for each disease state were collected from large, population-based data. 2,19 –22 IPRs <1.0 indicate underenrollment of women as defined by previous studies. 4
Calculation of Disease Prevalence by Sex
LDL, low-density lipoprotein cholesterol; MI, myocardial infarction; TC, total cholesterol; TR, tricuspid regurgitation.
Statistical analyses
Statistical analyses were performed using an R software Version 1.4.1717 (R Foundation, Vienna, Austria) on an Apple MacBook Air computer (Apple Corporation, Cupertino, CA) and included unpaired t-test and analysis of variance (ANOVA) comparisons of continuous variables and Chi-Square/Fisher's Exact test comparisons as indicated for categorical variables. Primary analyses—including association of authorship, clinical trial, and participant characteristics with IPR—were performed, including unpaired t-test and ANOVA comparisons of continuous variables, with a two-tailed significance level of p < 0.05, not adjusted for multiple comparisons.
Results
Of 68 trials, inclusion of women ranged from 0% to 71%, with a mean of 35.2% ± 13.6%. In total, 29.4% of trials had <25% female enrollment and 85.3% of trials had <50% female enrollment. Only 47.1% of trials reported sex-specific analyses. Of trials reporting racial demographics, on average 72.9% of participants were white and mean age of participation 65.1 years (Table 2). Of trials included, 32.4% addressed general or preventative interventions, 22.1% heart failure, 14.7% interventional, 19.1% electrophysiology, and 11.8% other interventions. Medication-based therapies were assessed in 53.0% of trials, while interventional procedures were assessed in 27.9% of trials. The remaining 19.1% of trials addressed a variety of interventions, including cardiac rehabilitation, nutritional interventions (e.g., alcohol use, coffee consumption), educational curricula (e.g., clinician counseling as a quality improvement initiative), telemedicine programs (e.g., home blood pressure monitoring, remote access to lipid counseling), and electronic medical record based interventions (e.g., calculation of 1 year mortality).
Inclusion to Participation Ratio by Trial Characteristics
Statistical significance demonstrated between bolded criteria at the following thresholds: a p < 0.05, b p < 0.01.
Missing data 4.5%.
SD, standard deviation.
The average IPR was 0.76 ± 0.27 for all trials and did not vary significantly based on conference, trial center, geographic region, or funding source (data not shown), with only 15 trials exceeding an IPR of 1.0 (Fig. 1). The average IPR varied by subspecialty, with a statistical difference noted between interventional cardiology and heart failure (0.65 vs. 0.88, p = 0.02). In addition, the average IPR was significantly lower for procedure-based trials compared with medication trials (0.61 vs. 0.78, p = 0.008), mean age <65 years of age versus ≥65 years (0.67 vs. 0.81, p = 0.03), and those with <1500 participants versus ≥1500 participants (0.69 vs. 0.84, p = 0.03). Only 21.2% of the authorship block was women, with 4/68 women presenting authors and 8/55 women senior authors, although without statistical difference in IPR by presenting or senior author gender.
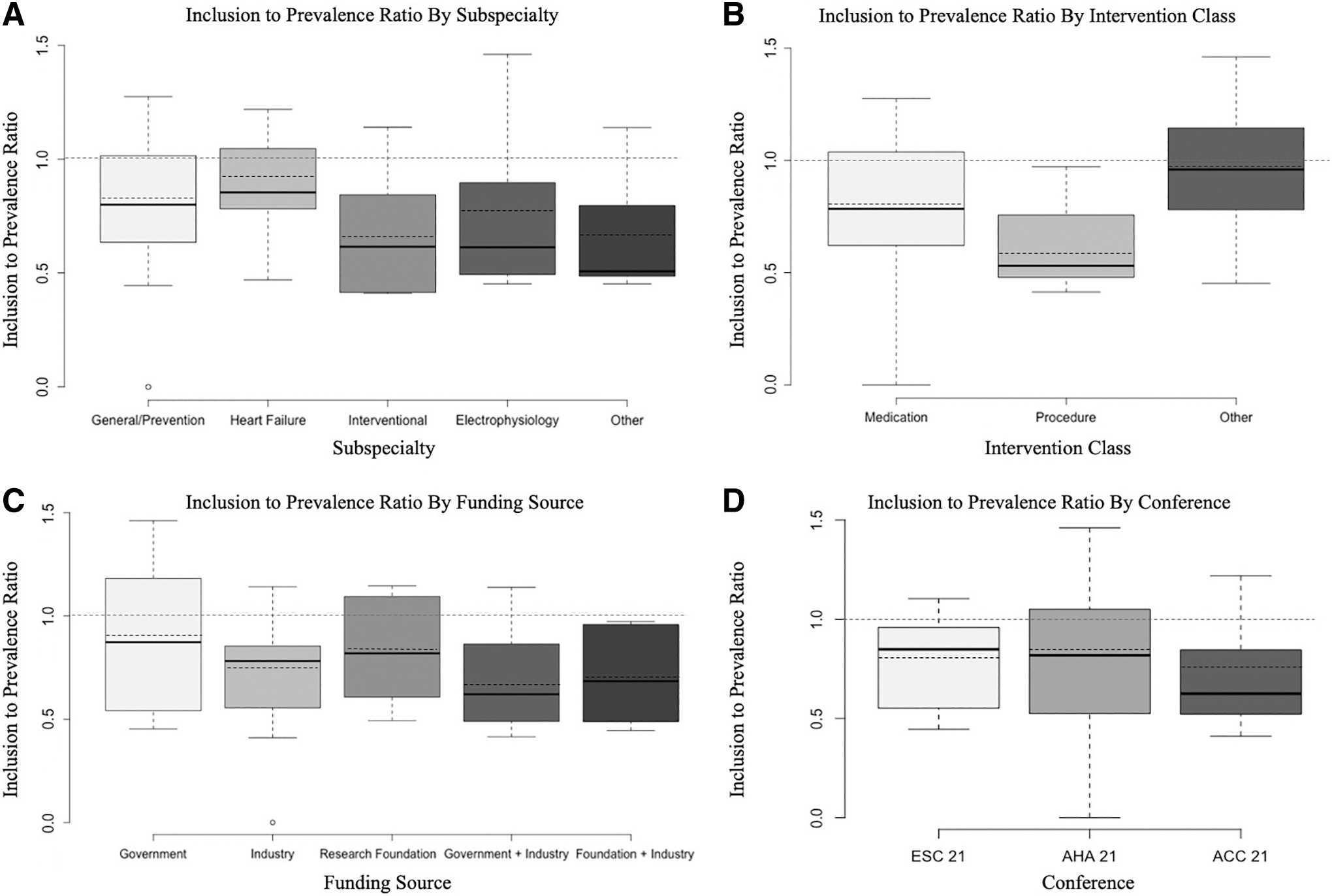
Inclusion of women in late-breaking clinical trials by prevalence of disease.
Discussion
LBCTs present novel, practice-changing evidence to the medical community on a prominent stage and as such, should represent the gold standard for diversity, equity, and inclusion in clinical trial enrollment. This analysis of three major cardiovascular conferences in 2021 suggests that previously documented low inclusion of women in clinical trials, particularly in interventional and procedural spheres, persists for LBCTs despite ongoing efforts to achieve gender parity. 4
Equitable trial enrollment has been a growing focus for both academic and professional organizations over the past decade. Despite well-documented disparities, coordinated strategic initiatives to incentivize the inclusion of female participants are lacking. Investigators have postulated that contributors to limited trial enrollment of women may fall into several spheres of influence, including the patient, clinical care team, local research team, clinical trial infrastructure, and broader societal expectations. 15 Strategies to augment the enrollment of women and underrepresented minorities in clinical trials may include reducing barriers to access interventional care and referral to subspeciality care, as well as extending age-based inclusion criteria. The COVID-19 pandemic has shed light upon the utility of pragmatic trial design in the acute care setting, allowing for expanded outreach capabilities and exploration of virtual interventions and follow-up. 23,24
Outside of drug- and device-based clinical trials, the remaining trials of nutritional- and cardiac rehabilitation-based interventions demonstrate a signal toward improved enrollment of women (IPR 0.94), although a specific subgroup analysis was not performed due to small subgroup size. Similarly, trials of telemedicine- and electronic medical record-based therapies demonstrate a signal toward improved enrollment of women, highlighting an opportunity to further explore the role for virtual, telemedicine-based clinical trial platforms to augment the enrollment of women. Telemedicine may reduce barriers to trial participation by decreasing physical, logistical, and transportation barriers for participants.
CVD presents often at a later age in women as compared with men; as such, previous studies have demonstrated that greater female enrollment in trials may be achieved through the recruitment of older population. 25 This finding was reflected in the LBCTs assessed, with trials that had a mean age <65 years, including fewer women, while trials that had a mean age >65 enrolling a higher proportion of women. Future analyses may consider calculating age-stratified IPRs by disease state to identify whether and the extent to which liberalizing the upper age limit for inclusion might improve equitable gender enrollment. Special attention should also be paid to diversification of clinical trial leadership, as a diverse team may be more likely to enroll a more diverse population. In fact, a recent study found that cardiovascular trials led by women enrolled more female participants than trials enrolled by men (44.9% vs. 37.9%, p < 0.001). 26
In this sample, only 4/68 reported first authors were female, 8/55 reported last authors were female, and 21% of the total authorship block were female, demonstrating significant room for growth. Specific benchmarks for diversity of gender should be set a priori in trial design with predetermined checkpoints and benchmarks to assess for goal attainment.
It should be noted that this analysis has several limitations. Although LBCTs garner additional attention on a prominent stage at national flagship conferences, presentation under the designation of “late-breaking” may also reflect the timing of data collection and analysis; future studies may consider assessment of trials designated as “Key Sessions” or those presented on the main stage at large conferences. Previous analyses of Altimetric scores to denote overall trial impact have noted a discrepancy between media attention and number of citations, suggesting that digital attention may stand in contrast to academic importance, limiting the use of such metrics. 27 Second, a single year of LBCT data from three major conferences may not be generalizable across years. In particular, the COVID-19 pandemic may influence both trial enrollment and study publication, given that women were disproportionately affected by the pandemic in terms of care-taking burden, employment, grant funding, and publication. 28 Third, the sample size of 68 studies may preclude detection of statistically significant differences in many study characteristics, given limited statistical power.
Despite gradual improvement in the inclusion of women in clinical trials, we find that enrollment of women continues to lag in LBCT at the three largest cardiology conferences. We encourage cardiology societies to select—and stakeholders to design—high-impact trials that enroll patients that are representative of the population.
Footnotes
Acknowledgments
The authors thank the CardioNerds for their unconditional support of their academic and professional development, and Daniel I. Ambinder, MD for involvement in the conceptualization of this study.
Author Disclosure Statement
The authors have no relevant disclosures.
Funding Information
No funding was received in support of this project.