
Abstract
Background:
Pain crises in sickle cell disease (SCD) lead to high rates of health care utilization. Historically, women have reported higher pain burdens than men, with recent studies showing a temporal association between pain crisis and menstruation. However, health care utilization patterns of SCD women with menstruation-associated pain crises have not been reported. We studied the frequency, severity, and health care utilization of menstruation-associated pain crises in SCD women.
Materials and Methods:
A multinational, cross-sectional cohort study of the SCD phenotype was executed using a validated questionnaire and medical chart review from the Consortium for the Advancement of Sickle Cell Research (CASiRe) cohort. Total number of pain crises, emergency room/day hospital visits, and hospitalizations were collected from a subcohort of 178 SCD women within the past 6 months and previous year.
Results:
Thirty-nine percent of women reported menstruation-associated pain crises in their lifetime. These women were significantly more likely to be hospitalized compared with those who did not (mean 1.70 vs. 0.67, p = 0.0005). Women reporting menstruation-associated pain crises in the past 6 months also experienced increased hospitalizations compared with those who did not (mean 1.71 vs. 0.75, p = 0.0016). Forty percent of women reported at least four menstruation-associated pain crises in the past 6 months.
Conclusions:
Nearly 40% of SCD women have menstruation-associated pain crises. Menstruation-associated pain crises are associated with high pain burden and increased rates of hospitalization. Strategies are needed to address health care disparities within gynecologic care in SCD.
Introduction
Sickle cell disease (SCD) is one of the most common genetic conditions worldwide with more than 300,000 births yearly. 1 It is characterized by vaso-occlusion, premature red cell destruction, vascular injury, and progressive organ damage. 1 Recurrent acute painful crises are a hallmark of SCD and are associated with disease severity, increased hospitalizations, and increased mortality. 2,3 Women with SCD have higher rates of acute vaso-occlusive pain than men, particularly within their reproductive years; 4,5 in addition, they are at increased risk for pain associated with their menstrual cycles. 6 –8 Reported data suggest that, around menstruation, 28%–36% of SCD women suffer from menstruation-associated pain crises, which are distinct from menstrual cramps. 6,8 In addition, 49% of adolescents with SCD report pain 1 week before their menstrual cycle and 54% report dysmenorrhea. 9
Despite several studies exploring the temporal relationship between vaso-occlusive pain and menstruation, little data exist on its frequency, severity, and health care utilization patterns associated with menstruation and sickle cell pain. In addition, studies have not included women from sub-Saharan Africa, which has the greatest SCD prevalence worldwide. Within the international Consortium for the Advancement of Sickle Cell Research (CASiRe) cohort, we aimed to determine the frequency, severity, and impact on health care utilization patterns of menstruation-associated pain crises. An improved understanding of the understudied SCD-related complications will provide needed guidance in the management of women with SCD.
Materials and Methods
The CASiRe group is an international multi-institutional collaboration with sites in the United States, Europe, and Africa, studying the clinical severity of SCD in 877 patients of all ages on a global scale using a validated questionnaire and medical chart review, standardized over three continents and four countries (the United States, Italy, Ghana, and the United Kingdom), as described previously. 10,11 This cross-sectional, multisite cohort substudy was institutional review board (IRB) approved at six CASiRe sites (four in the United States and two in Ghana). This substudy was added after CASiRe was established so we were unable to consent some patients from Europe (Napoli); other sites from Europe were not included in this study due to registry abstraction of data in the United Kingdom and Italy (Padova).
After receiving IRB approval at each institution, informed consent and assent were obtained from the study subjects, and the questionnaire was answered by the parent/legal guardian of the patient or by the patient herself. Females who had undergone menarche were asked if pain crises were associated with their menstrual cycle any time during their lifetime and within the past 6 months. Baseline and current laboratory data were collected. Medical chart review confirmed the total number of reported pain episodes during the previous year (whether or not these episodes were managed in a health care facility), the number of pain episodes requiring emergency room (ER)/day hospital (DH)/clinic visits in the past year, and the total number requiring hospital admission in the past year. We also recorded the subjective severity of pain during their menstruation-associated pain crises in a subset of patients. Information on other clinical complications associated with SCD was also extracted from the medical records. In Ghana, this involved a review of paper charts, while in the United States, review of electronic medical records was performed.
Statistics
Categorical variables are summarized by counts and percentages, whereas continuous variables are presented as mean ± standard deviation (SD). Categorical data were compared by chi-square or Fisher's exact test, and continuous data were compared by independent t-test. p-Values <0.05 were considered significant. Two-sided p-values were used. All statistical analyses were performed in SAS 9.4 (SAS Institute, Cary, NC, USA).
Results
Demographics
A total of 178 female participants who had attained menarche were enrolled (Table 1), 154 (86.5%) from Ghana and 24 (13.5%) from the United States. The mean age was 30.16 ± 12.49 years and did not differ based on whether they reported menstruation-associated pain crises. Three quarters of the participants (135/178; 75.8%) had HbSS genotype, 22.5% had HbSC, and 1.7% had HbSβ+-thalassemia. Only 11 (6.2%) women were on hydroxyurea and 4 (2.2%) on chronic blood transfusions, all of whom were from the United States. Sixteen (8.9%) women reported using some form of contraception. Of these, 13 women answered the type of contraception: 6 oral contraceptives, 4 injectable hormones, 2 intrauterine devices, 1 implantable device. Annually, the mean number of total pain crises was 4.80 ± 11.23 SD, the mean number of pain crises requiring an ER visit was 2.07 ± 2.91 SD, and the mean number of pain crises resulting in hospitalization was 1.07 ± 1.93 SD. Forty percent of women with HbSS and 32.5% of women with HbSC experienced menstruation-associated pain crises sometime during their lifetime.
Demographics and Clinical History
DH, day hospital; ER, emergency room; Hosp, hospitalizations; PC, pain crisis; SBeta Plus Thal, sickle beta plus thalassemia; SD, standard deviation.
Pain crisis frequency and health care utilization in the past year: Comparison of SCD women with menstruation-associated pain crisis in their lifetime versus SCD women without menstruation-associated pain crisis in their lifetime
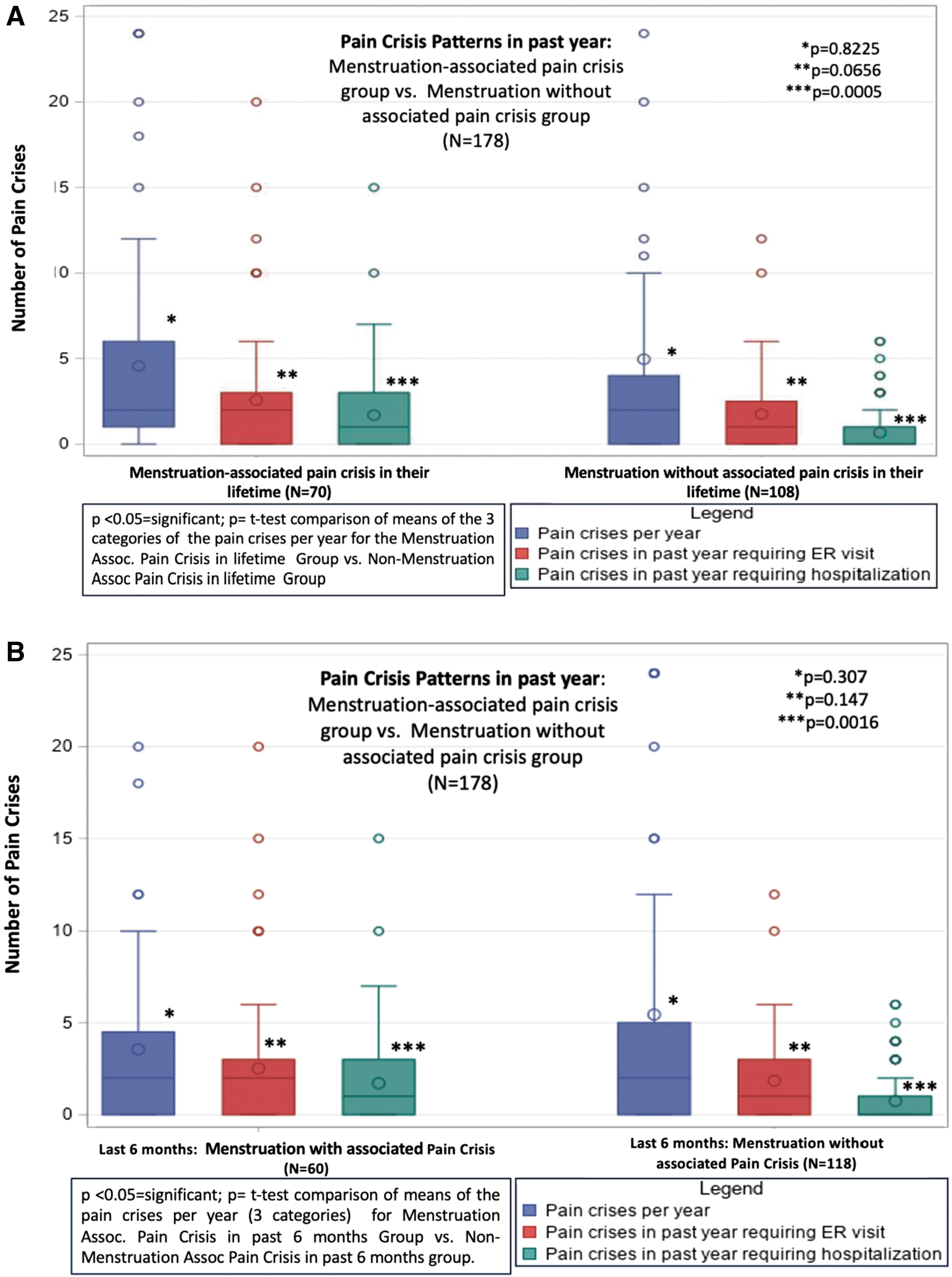
Seventy (39.3%) participants reported that their menstrual flow triggered pain crises in their lifetime (40% in Ghana and 37% in the United States) (Table 1). There was no significant difference in the mean number of pain crises per year in participants who experienced menstruation-associated pain crises in their lifetime compared with those who did not (Fig. 1). Over the previous year, there was an increased number of pain episodes requiring ER/DH/clinic visits in those with menstruation-associated pain episodes (mean ± SD: 2.57 ± 3.70 vs.1.75 ± 2.21), although this was not statistically significant (p = 0.0656) (Fig. 1A). However, women with a history of menstruation-associated pain were significantly more likely to be hospitalized (mean ± SD: 1.70 ± 2.53 vs. 0.67 ± 1.26, p = 0.0005) (Fig. 1A). Stratified analysis by country (the United States and Ghana) shows similar increases in hospitalization in women with menstruation-associated pain crises (Supplementary Table S1a, b).
Pain crisis frequency and health care utilization in the past year: Comparison of SCD women with menstruation-associated pain crisis in the past 6 months versus SCD women without menstruation-associated pain crisis in the past 6 months
Menstruation-associated pain crises within the past 6 months were recorded in 86% (n = 60) of participants who reported menstruation-associated pain crises in their lifetime (n = 70) (Fig. 1B). A history of menstruation-associated pain crises in the past 6 months was associated with increased hospitalization visits for pain (mean ± SD: 1.71 ± 2.66 vs. 0.75 ± 1.32, p = 0.0016) and a trend toward higher ER/DH/clinic utilization (mean ± SD: 2.52 ± 3.94 vs. 1.85 ± 2.19, p = 0.147) (Fig. 1B). The total number of pain crises per year was not significantly different between the two groups (mean ± SD: 3.55 ± 4.39 vs. 5.45 ± 13.49, p = 0.307) (Fig. 1B).
Frequency of menstruation-associated pain crises in the past 6 months
The total number of menstruation-associated pain crises was recorded in the past 6 months within the cohort of women who reported these symptoms (Table 2). Eight women from the United States and 52 from Ghana reported increased pain frequency during menses within the past 6 months. Forty percent (n = 24) of women reported four or more and 55% (n = 33) reported three or more menstruation-associated pain crises (Table 2). The remaining 45% of women reported one to two episodes of pain crises in the past 6 months (n = 27).
Frequency of Menstruation-Associated Pain Crisis in the Past 6 Months (N = 60)
Severity of menstruation-associated pain crises
A self-report of severity of pain crises (mild, moderate, severe) was recorded from 80% (n = 56) of the participants with menstruation-associated pain crises (Supplementary Fig. S1). This study did not include a validated tool for pain severity. Four women responded from the United States and 52 from Ghana. Thirty-six percent (n = 20) of women reported moderate-to-severe levels of pain, whereas 64% reported a mild level of pain.
Contraception and menstruation-associated pain crises
A subanalysis of women on contraception was performed. Eight of the 16 women who were on contraception reported experiencing menstruation-associated pain crises in their lifetime. Severity of menstruation-associated pain crises was recorded in 7 of the 8 women on contraception: none reported severe, 28.6% (n = 2) reported moderate, and 71.4% (n = 5) reported mild levels of pain. Of those not on contraception (n = 49), 6.1% (n = 3) reported severe, 63.3% (n = 31) reported moderate, and 30.6% (n = 15) reported mild levels of pain. However, women taking contraception revealed no significant difference in menstruation-associated pain crises frequency and health care utilization patterns compared with those not on contraceptives (Supplementary Table S2).
Discussion
Using a unique international cohort of women with SCD from different geographic and cultural backgrounds, our study aimed to provide a better understanding of the frequency and severity of menstruation-associated pain crises and the resultant impact on health care utilization. Our findings showed that nearly 40% of women in the United States and Ghana who had undergone menarche have increased pain burden demonstrated by higher hospital utilization for pain crises management, with more than one third reporting moderate-to-severe levels of vaso-occlusive pain during menses. When stratified by country, Ghanaian and American women with SCD reported similar frequencies of menstruation-associated pain crises at 40% and 37%, respectively. This is consistent with Sharma and colleagues' report of roughly 30% of women with SCD (n = 221) temporally associating vaso-occlusive pain episodes with their menstrual cycle in the United States 5 and Yoong and Tuck's study reporting 37% (n = 42) of U.S. women with SCD experiencing painful crises with each menses. 7
Data on health care utilization practices in menstruating women with SCD are lacking. Previous studies did not include health care utilization among women with SCD experiencing pain during their menses. 5,12 Pain crises requiring hospitalization were two times higher in women who experienced pain crises with menses during their lifetime compared with those who did not within our CASiRe cohort. When stratified by country, the increased hospitalization rate among SCD women experiencing menstruation associated pain crisis remains. A similar study in SCD women found that 21% had at least three cyclical crises documented in a 6-month period. 7 Comparatively, 58% of our study population reported at least three cyclical pain crises within 6 months.
The quality and characteristics of SCD pain associated with menses are well described in a qualitative study by Day et al. as well as in a descriptive study by Sharma et al. 6,8 Women with SCD were able to distinguish their acute vaso-occlusive (VOC) pain from menstrual pain, describing VOC as sharp pain in their bones compared with a muscular, throbbing, tingly pain experienced during menstruation. 6,8 The study by Sharma et al. also revealed that pain crises may present up to 7 days before the onset of menses. 8 Furthermore, only 40% of the 43 women reporting cyclical pain crises met the clinical criteria for dysmenorrhea in Sharma et al.'s report. 8
This is supported by Khachikyan et al.'s study showing that nearly 50% of SCD adolescent females reported pain 1 week before their menses. 9 More than one third of our SCD women experiencing menstruation-associated pain crises reported moderate-to-severe levels of pain. This group of patients may represent a subphenotype of pain severity given the increased hospitalizations and pain frequency reported in our cohort and supported by the aforementioned studies. 6,8 Unfortunately, despite the distinguishing characteristics of menstruation-associated pain crises described by women with SCD, many caregivers and clinicians have not modified their treatment protocols accordingly or in an individualized manner. 6
Health care providers' poor understanding and lack of knowledge of the different types of pain that can occur in women with SCD lead to a further widening of the health care disparities that already exist within SCD reproductive and gynecologic health. 6 Previous studies report women being underappreciated when discussing menstruation-associated pain, compounding the pre-existing lack of compassionate care and poor access to appropriate pain management for non-menstruation VOC pain episodes in the ER or other acute care settings. 6,13 Despite initiatives to address the global inequities in the management and treatment of SCD, efforts to prioritize women's health issues in this setting are lacking. 8,13 In a review by Smith-Whitley, the paucity of large well-designed clinical trials and reliance on relatively old studies in an era of medical advancement for SCD have contributed to this disparity. 13
Effective treatment options remain a challenge globally for SCD women with gynecologic issues, including menstruation-associated pain, especially in sub-Saharan Africa. Across the world, significant gaps in care exist relating to reproductive health for women with SCD. 14 No evidence-based guidelines exist to guide the management of menstruation-associated pain in SCD. There is a lack of data available on the risks and benefits of various contraceptive methods, factors that influence contraceptive choice, and short- and long-term impact on health and quality of life. Schichor initially reported that hormonal contraception may be effective in decreasing pain crises in women with SCD. Treatment with medroxyprogesterone acetate led to significantly less pain crises compared with placebo in 23 SCD women during a 2-year controlled crossover trial. 12
Another study of 43 women reporting at least one pain crises per month who were placed on 1 year of contraception with either trimonthly depot-medroxyprogesterone acetate (DMPA) or once monthly microgynon found that 70% of patients were pain free on the DMPA treatment arm, while patients on microgynon reported fewer pain crises at a lower rate. 15 Our study reported that just 16 of the 70 women with a history of menstruation-associated pain crises were on some form of contraception, all of them from the United States, highlighting the challenges with overall access to mitigating strategies for women experiencing cyclical pain as well as disparities between high-income and low/middle-income countries. Similarly, one study found that 18.8% of women with SCD reported using oral contraceptives. 16 Women with SCD also report a low use of long-acting reversible contraception (22%) and demonstrate low knowledge of the efficacy of hormonal contraceptive options; 17 in addition, 73% report that SCD did not inform their choice of birth control. 17
Furthermore, women with SCD have twice the odds of venous thromboembolism compared with men with SCD; 18 this risk must be weighed when considering hormonal contraception choices. Lack of needed public health attention in women with SCD has led to a paucity of reproductive health services globally including oral contraceptives as an option, especially in women living in Ghana. 19,20 In addition, socioeconomic factors, education status, religious, and cultural beliefs may impact availability and acceptance of reproductive options and treatments for women in Ghana living with SCD. 20 The high percentage (40%) of Ghanaian SCD women reporting cyclical pain crises in our study underlies the additional burden of pain they experience in our cohort. Ghanaian women with menstruation-associated pain crises were hospitalized significantly more times than their case–controls of similar age.
Access to disease-modifying therapies remains a challenge for SCD patients in Ghana including available blood transfusions and hydroxyurea likely leading to the higher combined ER visits and hospitalizations than their case–control cohort from the United States (Supplementary Table S1a, b). Intervening earlier with disease-modifying therapies such as hydroxyurea is a strategy for prevention in SCD patients in high-income countries. Hydroxyurea was given earlier to U.S. children who experienced earlier pain crises in a previously published study by our CASiRe cohort. 11 Recent studies in some sub-Saharan African countries and other lower-middle income countries have shown efficacy in reducing sickle cell complications with hydroxyurea. 21 –23
Unfortunately, these treatment options remain inaccessible for many SCD patients living in Ghana and many other African countries where the disease burden remains the highest. Strunk et al. revealed that the main contributor to disparities in health care utilization was the lack of financial resources, lack of local health care providers, and poor access to appropriate pain medication including opioids leading to a higher rate of DH/ER visits compared with the United States within the CASiRe cohort study. 24 Thus, Ghanaian SCD women experiencing menstruation-associated pain crises experience additional health care barriers including access to these disease-modifying treatments. Development of SCD-specific therapies as well as treatment specific to managing menstruation are needed desperately to control the pain crisis before the onset or during menstruation.
This study had several limitations. First, most of our study population was from Ghana, with only a handful of women with SCD in the United States represented due to the fact that this was a secondary analysis of the larger CASiRe study. This limits the generalizability of our findings; however, when data were stratified by country, similarities in pain frequency and increased health care utilization were seen. Second, the indications for contraceptive use were not assessed, and we cannot ascertain whether patients were placed on contraception for pregnancy prevention or for managing menstruation-associated pain. We also did not use a validated tool for the recorded severity of menstruation-associated pain crisis from each subject. Finally, we did not further explore the impact of menstruation-associated pain crises on daily functioning and health-related quality of life, which will be the focus of a future prospective study.
In conclusion, we found that menstruation-associated pain crises occurred in more than one third of U.S. and Ghanaian women with SCD with a significant increase in hospitalizations in those who experienced menstruation-associated pain. This has major implications for provision of appropriate gynecologic care for women with SCD and underscores the extreme importance of improving access to effective treatment options including contraceptives and disease-modifying therapies.
Footnotes
Acknowledgments
Thanks to Adetola Kassim and Vishwas Sakhalkar for their help in developing the questionnaire and protocol. Thanks to the students at the University of Michigan Minority Health and Health Disparities International Research Training (MHIRT) program: Ahmed Owda, Duna Buttner, Sophia Akatue, Ashya Smith, Austin Novarra, Clementine Fu, Lewis Graham, Esther Kim, Haikel Halle, Sheri Van Omen, Marianna Yamamoto. Thanks to our patients and their families who enthusiastically participated in the study.
Authors' Contributions
C.Se., J.C., and A.C. wrote the article and analyzed the data. C.St., I.T., and C.M.P. critically edited the article and analyzed the data. J.C., C.Se., A.C., J.G., S.W., I.T., C.St., A.R., B.I., D.M., E.V.A., B.A., C.A.-B., R.C., R.U., F.F., W.Z. contributed to the interpretation of the results. All authors (excluding J.C., J.G., and A.R.) contributed to the collection of the data. All authors reviewed and approved the final article.
Author Disclosure Statement
There are no competing conflicts of interest as it relates to this article. However, below are the listed financial disclosures of the authors: A.C.: Research funding and consultancy from Global Blood Therapeutics, Novartis, Agios, Bluebird Bio; consultancy from Cheisi. D.M.: Research funding from Grifols; consultancy for Novartis, Pfizer, Global Blood Therapeutics. B.A.: Consultancy for Aruvant, Agios, Bluebird Bio, CRISPR, Forma, Global Blood Therapeutics, Hemanext, Novartis, NovoNordisk, Emmaus, Cyclerion, Terumo, Sanofi, Vertex; research funding: Imara. B.I.: Education funding: Novartis AstraZeneca, Global Blood Therapeutics, Celgene, Vertex. C.St.: Consultancy Global Blood Therapeutics and Novartis. R.C.: Research funding: Global Blood Therapeutics, Novartis. W.Z: Consultancy: GlycoMimetics, GlaxoSmithKline, Lundbeck. C.M.P.: Consultancy for Novartis and Global Blood Therapeutics, DSMB: Global Blood Therapeutics. No disclosures to declare from the other co-authors.
Funding Information
This study was supported in part by research funding from Grant No. National Institute on Minority Health and Health Disparities T37MD001425 to A.C.
Supplementary Material
Supplementary Figure S1
Supplementary Table S1
Supplementary Table S2
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.