
Abstract
Purpose:
The aim of this study was to utilize an intersectional framework to examine academic faculty's lived experiences during COVID-19. Specifically, we set out to: (1) describe the multiple intersectional identities (e.g., gender, race/ethnicity, rank, caregiver status, disability status) represented by the faculty, (2) examine potential disparities in well-being, workload, and productivity linked to these intersectional factors, and (3) identify qualitative themes endorsed by faculty as they relate to lived experiences during COVID-19.
Methods:
This was a cross-sectional mixed-methods research study. The Center for Women in Medicine and Science (CWIMS) at the University of Minnesota developed and implemented a survey between February–June of 2021 in response to national reports of disparities in the impacts of COVID-19 on faculty with lived experiences from multiple intersections.
Results:
There were 291 full-time faculty who participated in the study. Quantitative findings indicated that faculty with multiple intersectional identities (e.g., woman+assistant professor+caregiver+underrepresented in medicine) reported greater depression symptoms, work/family conflict, and stress in contrast to faculty with fewer intersectional identities. Furthermore, faculty with more intersectional identities reported higher clinical workloads and service responsibilities and lower productivity with regard to research article submissions, publications, and grant submissions in contrast to faculty with fewer intersectional identities. Qualitative findings supported quantitative findings and broadened understanding of potential underlying reasons.
Conclusions:
Findings confirm anecdotal evidence that faculty with lived experiences from multiple intersections may be disproportionately experiencing negative outcomes from the pandemic. These findings can inform decisions about how to address these disparities moving into the next several years with regard to promotion and tenure, burnout and well-being, and faculty retention in academic medical settings. Given these findings, it is also important to intentionally plan responses for future public health crises to prevent continued disparities for faculty with multiple intersectional identities.
Introduction
Recent research has shown that the COVID-19 pandemic has resulted in adverse impacts on well-being 1 –4 and productivity 5 –7 for many faculty in academic settings. Key outcomes assessed include burnout, anxiety, depression, 1 –4 and increased substance dependence. 8 –10 Research has further suggested that minoritized groups such as faculty who identify as Black, Indigenous, and People of Color, women, or early-career faculty, may be at greater disadvantage with regard to the impacts of COVID-19. 2,3,5,11 –23 However, little is known about the impact of COVID-19 on academic medicine faculty with regard to multiple overlapping identities such as gender, race/ethnicity, academic rank or track, disability, caregiver status, or underrepresentation in medicine. 24 The purpose of this article is to use an intersectional framework to identify and describe the diversity of faculty experiences during the COVID-19 pandemic and to examine potential disparities in emotional well-being, workload, and productivity as they relate to intersecting social identities.
Intersectionality is a theoretical framework, which posits that heterogeneity across different intersections of identity (e.g., race/ethnicity, gender, education status, career status) is integral to understanding health and social experiences. 25,26 Specifically, social positions that exist on a hierarchy of social power are not independent and ultimately shape human experience jointly. 27 As social positions intersect at the individual level (e.g., race and gender), experiences at those intersections are influenced by larger interpersonal and structural systems of oppression such as racism and sexism. 28,29 Thus, individuals with multiple oppressed identities have unique experiences from one another. When pursuing research that aims to examine disparities, we must consider everything that can marginalize people (gender, race, class, sexual orientation, physical ability, caregiver status, academic rank, etc.) as potentially overlapping.
The main research questions for this mixed-methods study include: (1) What are the multiple intersectional identities represented by academic medicine school faculty during COVID-19 at the University of Minnesota (UMN) Medical School? (2) How are the intersectional lived experiences of faculty linked to disparities in emotional well-being, workload, and productivity during the COVID-19 pandemic? and (3) What qualitative themes do faculty endorse with regard to multiple lived experiences and intersectional identities throughout the pandemic?
Methods
Study design and sample
After numerous reports and early evidence of disparities experienced by faculty with multiple intersectional identities (e.g., women, minority, assistant professors, caregivers, disability), 3,5,11 –23 the Center for Women in Medicine and Science (CWIMS) 30,31 at the UMN Medical School decided to explore this issue further. We conducted a cross-sectional mixed-methods study aimed at examining faculty workload, productivity, and well-being during the COVID-19 pandemic. An online Qualtrics 32 survey was developed and administered in February–June 2021 to study the influence of COVID-19 on the lived experiences of full-time faculty from the UMN Schools of Medicine (n = 3000 faculty), Public Health (n = 130 faculty), and Dentistry (n = 120 faculty) who were eligible to participate in the study. There were 291 faculty who completed the survey, with some faculty (n = 7) holding dual appointments in multiple schools (e.g., Medical School and the School of Public Health).
Survey development
A diverse group of women faculty (n = 15), including both PhDs and MDs, representing the majority of departments within the UMN Medical School, who were also members of CWIMS, met regularly in May 2020 to November 2020 to develop a cross-sectional survey according to survey research best practices. 33,34 Multiple stakeholder groups (e.g., Office of Faculty Affairs; Office of Diversity, Equity and Inclusion; Well-being Working Group) were also convened for feedback during survey development. Survey items were drawn from pre-existing and validated surveys unless they were new areas of research, such as COVID-19 questions, which were then created by the study team or adapted from other studies. 8,35 –37 The anonymous survey included 81 questions, using branching logic to reduce survey participant fatigue.
In addition to quantitative survey questions, seven qualitative write-in responses were solicited through questions such as: (1) “Please describe in what ways, if any, your productivity has been impacted as a result of the COVID-19 pandemic,” (2) “Please describe how changes to childcare/education for the 2020–2021 school year have impacted your family,” (3) “Please explain changes, if any, you have made to your personal priorities since the COVID-19 pandemic,” (4) “Please share how your academic work experience during the COVID-19 pandemic has been influenced by any of your identities (e.g., your gender or racial identity).” On average the survey took 15–20 minutes to complete. This study was determined not to be human subject research (STUDY00010358: COVID-19 Health Sciences Faculty Survey) by the UMN IRB. However, given survey research best practice was used in the development of the survey, 33,34 consenting language was included.
Procedures
Study participants were recruited by email through their university email account over the months of February to June 2021. Emails were sent twice from two different centers/offices 4 weeks apart, in addition to personal contacts from faculty's own departments to increase potential uptake for our survey response rate. Data were collected through the Qualtrics 32 survey administered through the CWIMs' account. Upon completing the survey, individuals received an email with consent information and were automatically placed into a random drawing for 50 prepaid $25 gift cards.
Measures
The survey collected information regarding participants' intersectional identities and examined their perceptions and experiences relating to well-being, workload, and productivity. All measures are listed in Supplementary Digital Appendix SA1. Qualitative data from questions utilizing free text write-in responses were used in qualitative analyses. All participants provided a free text response to at least one open-ended question.
Statistical analysis
Quantitative analysis
Overall participant demographic characteristics were summarized using counts (%) and displayed in both traditional format (Table 1) as well as visualized using sunburst plots, which reinforce emerging best practice 38 for applying an intersectional theoretical lens to data through data visualization. This intersectional approach embraces pluralism and demonstrates the mosaic of faculty within our data across multiple identities while protecting individual demographic information. Sunburst plots (Fig. 1) contain a series of concentric rings, with each layer of the concentric rings providing visual insight into faculty's multiple intersecting identities and lived experiences. The layers represent: gender (i.e., man, woman, self-identified), underrepresented in medicine (URM) 24 (i.e., yes/no), rank (i.e., assistant, associate, full professor), mission focus (i.e., clinic, education, research), caregiver status (i.e., yes/no) and disability status (i.e., yes/no). New variables were created to group participants into three intersections between identity and lived experience, including gender by URM, gender by caregiver status, and gender by rank.
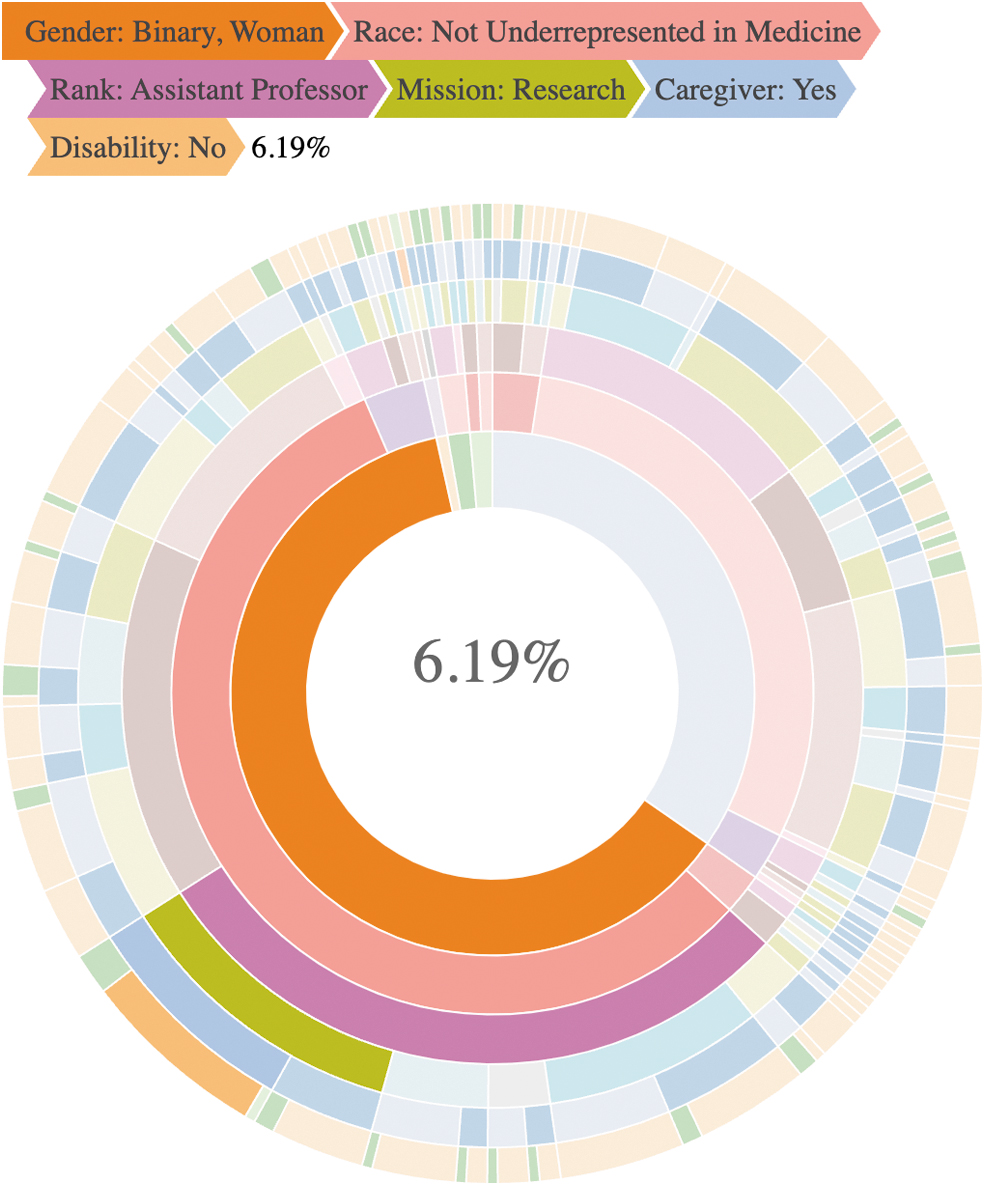
Sunburst plot of intersections of faculty lived experiences. Each layer of the concentric rings provides visual insight into faculty's multiple intersecting identities and lived experiences, representing: gender (i.e., man, woman, self-identified), URM (i.e., yes/no), rank (i.e., assistant, associate, full professor), mission focus (i.e., clinic, education, research), caregiver status (i.e., yes/no), and disability status (i.e., yes/no). The dark color pathway shows that about 6% of our sample identified as having the following multiple identities simultaneously: woman, not URM, assistant professor, primarily a researcher, caregiver, and has no disability. URM, underrepresented in medicine.
Participant Demographic Characteristics a
Percentages are calculated out of nonmissing values.
Gender: Self-described gender included “trans masculine/2nbinary,” “Fluid,” and “Genderfluid.”
URM: Black, Hispanic, American Indian/Alaska Native, Middle Eastern, North African, and multiple. 24
URM, underrepresented in medicine.
Well-being outcomes (i.e., PHQ4, family-work conflict, work-family conflict, stress, and Brief Resilience Coping Scale) were averaged within these intersections and scaled such that each outcome ranged from 0% to 100%, where the identity with the lowest score was assigned 0% and the highest assigned 100% allowing us to visually summarize the data across intersections. Radar figures (Fig. 2) were used to display outcomes for each of the intersectional identities (e.g., women, URM) in relation to their reported well-being outcomes. Lastly, bar plots (Figs. 3 –5) were used to show the relationship between intersectional identities and a variety of workload and productivity measures within each faculty mission area. Perceptions of workload in each mission area are presented as percentages of respondents answering less, same, or more to how their workload changed since the COVID-19 pandemic. Analysis was completed in R, version 4.1.1 (R Foundation for Statistical Computing, Vienna, Austria).
Qualitative analysis
A hybrid deductive and inductive qualitative analysis approach was used in coding the qualitative write-in response options in the survey. Specifically, the write-in response questions guided the formation of the deductive coding tree nodes, then additional inductive themes emerged within each deductive coding node during the coding process. 39,40 After all responses (n = 208) were initially coded into the deductive nodes, two additional rounds of coding were completed by two authors (J.M.B. and S.M.) to: (1) identify inductive themes and (2) identify inductive subthemes regarding faculty's lived experiences during COVID-19. Qualitative coding was conducted using Microsoft Excel 2016 (Microsoft Corporation, Redmond, WA). Quotes chosen for inclusion in the article exemplified the qualitative theme, with additional quotes being included in the Supplementary Digital Appendix SA2.
Results
Findings are organized by our research questions and presented with quantitative results first and qualitative findings second. Additional quotes by theme are presented in Supplementary Digital Appendix SA2.
Research question 1: what are the multiple intersectional identities represented by academic medicine school faculty during COVID-19 at the UMN Medical School?
Quantitative findings
Table 1 shows a traditional quantitative demographics table. Approximately 60% (n = 180) of faculty identified as women, about half (n = 133, 46%) of our sample reported being caregivers (child, adult, or caregiver for both), and almost half (n = 135, 47%) were assistant professors. In addition, about 14% (n = 40) of faculty reported having a disability, and close to 10% (n = 16) of faculty reported being from an URM group. 24 Faculty were almost equally split across focus areas of clinic, research, or education, with about 15% (n = 43) reporting a mixed appointment (e.g., clinic and research) and 5% (n = 14) reporting a primary focus on educational efforts.
When the sample demographics are viewed through the sunburst plot (Fig. 1) a more complex pattern emerges, identifying multiple intersections representing our faculty's lived experiences. For example, the dark color pathway in Figure 1 shows that about 6% of our sample identified as having the following multiple identities simultaneously: woman, not URM, assistant professor, primarily a researcher, caregiver, and has no disability. Other paths on this sunburst show other combinations of these identities and lived experiences, giving a more complete picture of the complexity of our faculty.
Qualitative findings
Two main qualitative themes emerged when faculty were asked about how their multiple identities may have impacted their lived experiences during COVID-19, including (1) multiple identities and lived experiences and (2) fewer leadership opportunities.
Multiple identities and lived experiences
Women faculty consistently reported that being a woman during COVID-19 adversely affected them due to their intersecting identities and multiple lived experiences. One faculty who identified as a woman and a caregiver stated: I feel that women have been more adversely affected during the pandemic due to increased caregiving and service demands. I also feel that I have probably been more adversely affected than male colleagues.
Another faculty who identified as a woman and URM expressed: My experience during COVID has been influenced by my racial identity because the pandemic has overlapped with another significant event in society- the most recent wave of recognition of systemic racial disparities permeating our society. During the immediate weeks after the George Floyd incident, I found it very hard to concentrate on work or focus on productivity. The immediate stress has dissipated, but it reminded me of the persistent underlying anxiety related to race that permeates my personal and professional life.
Men faculty also recognized that their lived experiences and identities affected them during COVID-19. One faculty who identified as a man said, “Being a white male has likely made my work easier than my non-white or my female colleagues.”
Fewer leadership opportunities
Women faculty reported fewer leadership opportunities being available during the pandemic as a result of their multiple lived experiences. One faculty who identified as a woman and caregiver said: Prior to and during the pandemic, as a woman, I feel I am often underestimated and overlooked for leadership positions. I have hunkered down and cranked out the work, more than my male colleagues, and I am viewed as “likable” and reliable and someone people want to work with, yet I do not have any real leadership role or ability to make decisions, develop programs, advocate for hiring, etc. I am expected to do increased work during the pandemic without recognition, promotion, or salary increases, and if I try to set boundaries or limits to have better work-life balance, it means someone else gets that opportunity who has fewer home demands.
Research question 2: how are the intersectional lived experiences of faculty linked to disparities in emotional well-being, workload, and productivity during the COVID-19 pandemic?
Lived experiences of faculty emotional well-being during COVID-19
Quantitative findings
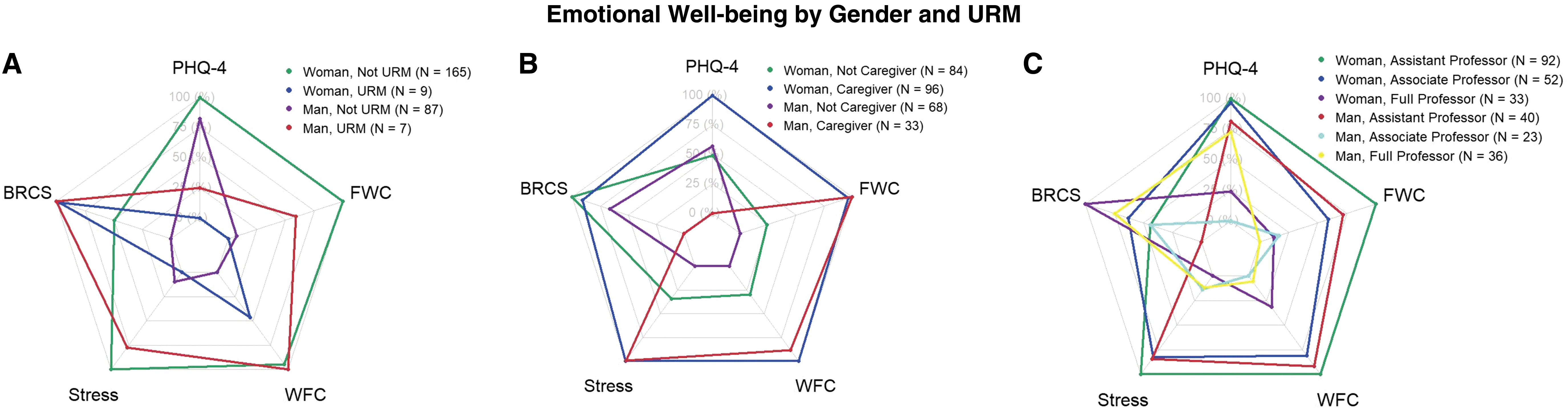
Figure 2A shows the dynamics between experiences of gender and URM across multiple domains of emotional well-being. Women who did not identify as URM reported the highest depressive symptoms (e.g., PHQ4), family-work conflict/work-family conflict, and stress scores, but reported scores in the mid range for coping skills. Men who did not identify as URM had the lowest or next to lowest family-work conflict/work-family conflict, stress scores, and coping scores.
In Figure 2B, the intersections between gender and caregiver roles with regard to emotional well-being are described. Women who identified as caregivers reported the highest scores on depressive symptoms, family-work conflict/work-family conflict, and stress. Men who did not identify as caregivers had the lowest family-work conflict/work-family conflict, stress, and mid-range scores on depressive symptoms and coping skills.
In Figure 2C, the intersections between gender and rank with regard to emotional well-being are described. Women who identified as assistant professors reported the highest levels of depressive symptoms, family-work conflict/work-family conflict, and stress but reported scores in the mid-range for coping skills. Men who identified as associate professors had the lowest or next to lowest levels of depressive symptoms, family-work conflict/work-family conflict, and stress, as well as coping skills.
Qualitative findings
There were two qualitative themes found under emotional well-being, including (1) general overall stress and (2) caregiving and stress.
General overall stress
Women faculty reported a higher overall sense of stress due to the ambiguity and uncertainty of COVID-19 and social unrest related to racism. One faculty identifying as a woman described: …more distractions in my environment, fewer boundaries between home and work, less motivation to complete tasks, general malaise about the state of the world, frequent checking of news related to COVID-, racial justice- and political issues.
Caregiving and stress
Women faculty also expressed that the stress they were experiencing during COVID-19 was related to being a caregiver. One faculty who identified as a woman, caregiver, and assistant professor said: I am constantly stressed by the balance of motherhood and work. There doesn't seem to be space for lightness and fun in the midst of community and national discord as well as the pandemic…I feel that few useful things are being done to support faculty. I'm not really interested in a tenure clock extension as it's already an incredibly long road to become an associate professor. I'm also struggling to see the end of the road with being able to provide my children with safe and fun activities and connect socially in more satisfying ways.
Lived experiences of faculty's workload during COVID-19
Quantitative findings
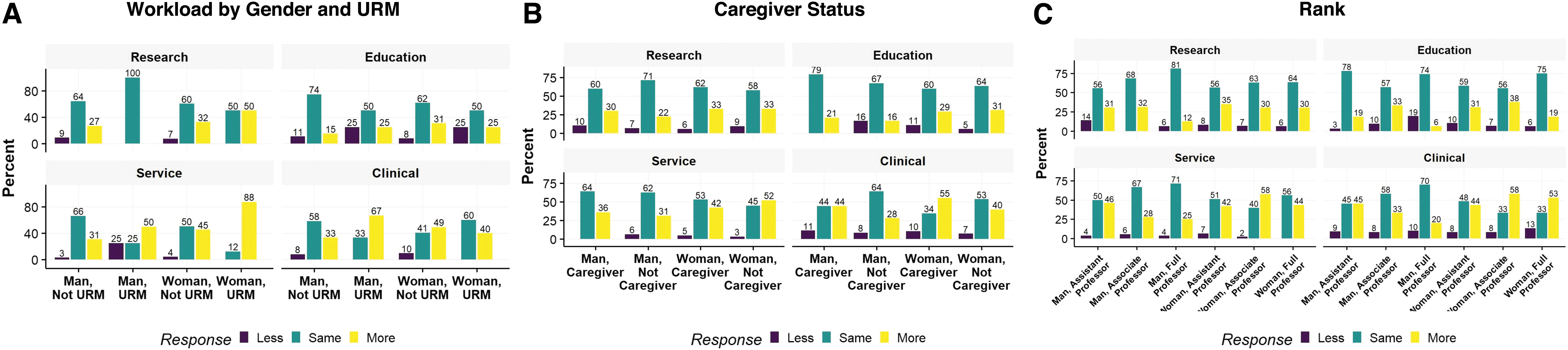
Figure 3A focuses on the intersection between gender and URM with workload. Results showed that 88% of women and 50% of men who identified as URM reported that their service workload was currently more than before COVID-19, compared with 45% and 31% of women and men who did not identify as URM, respectively. In addition, 67% of men who identified as URM reported doing more clinical work than before COVID-19. Only 33% of men who did not identify as URM reported that their workload had increased.
In Figure 3B, the intersections between gender and caregiver role with workload are described. Results showed that both women who were caregivers (42%) and women who were not caregivers (52%) reported their service workload was currently more than before COVID-19. Only 36% of men who were caregivers and 31% who were not, reported that their service workload increased from before COVID-19. In addition, 55% of women caregivers reported their current clinical workload had increased compared with before COVID-19. In contrast, 64% of men noncaregivers reported that their clinical workload stayed the same.
Figure 3C depicts the intersection between gender and rank with regard to workload. Results showed that 42%–58% of women at any rank and ∼50% of men who identified as assistant professors reported more service and clinical workload currently than before COVID-19. More men at associate or full professor rank reported that their service and clinical responsibilities were unchanged during COVID-19.
Qualitative findings
The main qualitative theme found was that workload greatly increased during COVID-19 for women faculty.
Workload increased
Women faculty reported that their workload dramatically increased across all missions (i.e., clinical, education, research, administration) during COVID-19. One faculty identifying as a woman and an assistant professor stated: Every area for me increased and new work demands, starting immediately in March 2020. Much of my previous work was put on hold to address the new demands and now all that gets done is what needs to get done. The “old” work is still on hold. The new work has taken over and is the priority.
Other women faculty reported that workload increased because they were doing the work of others that were not replaced because of a COVID-19 hiring freeze. One example included: I am doing the onsite work for 5 other employees who have been working from home or who have left their positions and the University has not permitted replacement hires.
Men faculty commonly pointed to logistical challenges with COVID-19. One faculty identifying as a man stated, “working remotely is less efficient.” Another said, “Teaching in the era of remote learning has required redesigning curriculum and delivering it differently.”
Lived experiences of faculty's productivity during COVID-19
Quantitative findings
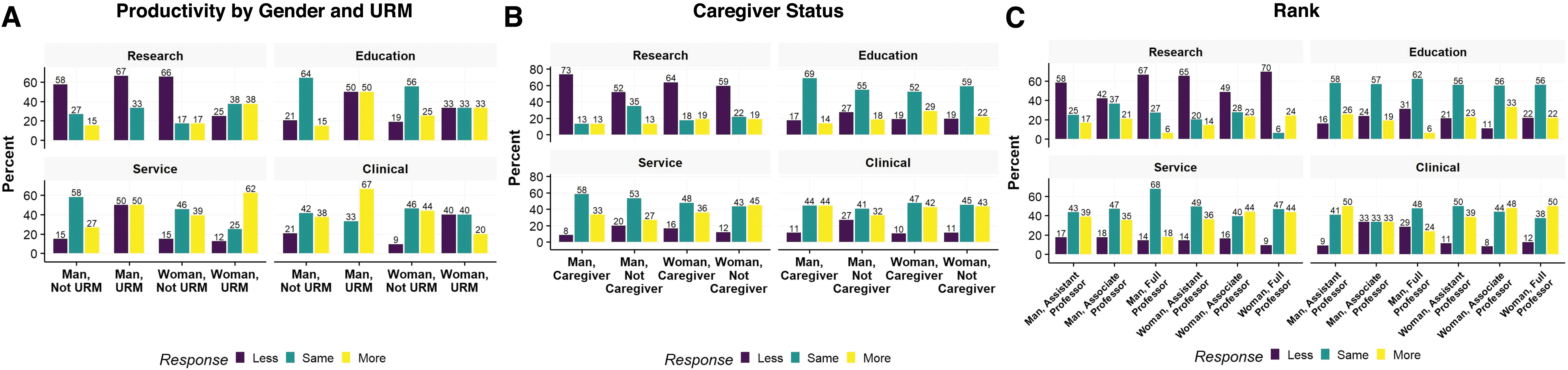
Figure 4A focuses on the intersection between gender and URM with productivity. More women not identifying as URM (i.e., 66%, 44%) and men who identified as URM (i.e., 67%, 67%) reported less research productivity and more clinic productivity compared with before COVID-19. Men who did not identify as URM reported their clinic productivity stayed the same. In addition, 62% of women who identified as URM and 50% of men who identified as URM reported more service productivity as compared with before COVID-19 in line with the reported increased service workload.
In Figure 4B, the intersections between gender and caregiver role with regard to productivity are described. Results show that 73% of men caregivers and 64% of women caregivers who did not identify as URM reported less research productivity than before COVID-19. Only 52% of men noncaregivers reported less research productivity compared with before COVID-19.
Figure 4C depicts the intersection between gender and rank with productivity. Results showed that women and men assistant professors (i.e., 65%, 58%) and women and men full professors (i.e., 70%, 67%) reported less research productivity as compared with before COVID-19. Women associate professors (44%, 48%), women full professors (44%, 50%), and men full professors (18%, 24%) reported more service and clinical productivity since before COVID-19.
Qualitative findings
Two main themes were identified under productivity: (1) decreased research productivity, and (2) caregiving role impacts on productivity.
Decreased productivity
Women faculty said there were many reasons for their decrease in productivity during COVID-19, with one main reason being their multiple lived experiences. One faculty who identified as a women and caregiver stated: …I think the overall quality of the work produced decreased due to burn out, home responsibilities, and barriers that women faculty face. There have been benefits to working from home, but I am definitely burned out in a different way as a result of so much social isolation.
Men faculty also indicated a decrease in productivity during the COVID-19 pandemic. However, their main reason was challenges related to working virtually rather than their multiple lived experiences. One faculty identifying as a man said: I have more clinical responsibilities, specifically more time clinically that was taken away from academic time. The academic needs actually increased due to changing to virtual…
Caregiver roles
Women faculty said that their caregiving role greatly impacted their productivity. A faculty who identified as a woman, caregiver, and assistant professor expressed: Lack of additional child care options (i.e., evening/weekend help from family/friends) has resulted in decreased productivity since I need to perform tasks around my house (e.g., cooking, cleaning, etc.) during normal work hours instead of during times when I would usually have help here and there.
Lived experiences of faculty's article and grant submission during COVID-19
Quantitative findings
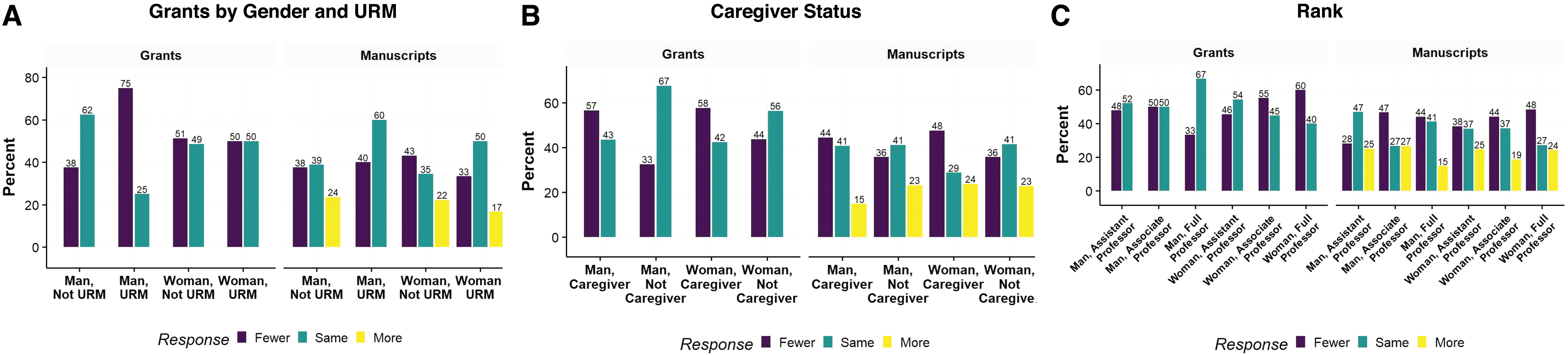
Figure 5A focuses on the intersection between gender and URM with regard to articles and grants. Results showed 75% of men who identify as URM, 50% of women who identify as URM, and 51% of women who do not identify as URM reported submitting fewer grants than before COVID-19. Both men (60%) and women (50%) who identify as URM reported submitting the same amount of articles as before COVID-19.
Figure 5B depicts the intersection between gender and caregiver role with regard to articles and grants. Results show that 58% of women caregivers and 57% of men caregivers reported submitting fewer grants than before COVID-19 and 48% of women caregivers and 44% of men caregivers reported submitting fewer articles. By contrast, 67% of men noncaregivers and 56% of women noncaregivers submitted the same amount of grants as compared with before COVID-19.
Figure 5C shows the intersection between gender and rank with regard to articles and grants. Results indicated that 67% of men full professors submitted the same amount of grants compared with before COVID-19. By contrast, 60% of women full professors submitted fewer grants compared with before COVID-19. Women across all ranks reported submitting fewer articles compared with before COVID-19.
Qualitative findings
Four themes emerged when faculty were asked about articles and grant productivity during COVID-19, including: (1) productivity decreased, (2) gender disparities in funding, (3) collaboration/communication decreased, and (4) productivity increased.
Productivity decreased
Women faculty said that their research/scholarship, both articles and grants, took a major hit due to COVID-19 and a main contributor was their multiple lived experiences, including being a caregiver. One faculty who identified as a woman, and caregiver, expressed: My research productivity, which my tenure depends on, has suffered significantly. I have three school age children at home who have been doing distance learning since March 2020 and I am the primary caregiver. The time available to read, think, complete research and data analysis, and write has been squeezed out dramatically due to the demands of caregiving, teaching (students are needing so much more), service, and increased clinical demands (keeping up with COVID changes). The time demands for teaching and service have increased due to changes in courses, student needs, and increased need for people to complete service work (and increased demands due to COVID, uprising/anti-racism work).
While some men faculty also reported that their article and grant productivity decreased, they focused more on logistical issues rather than multiple identities leading to disadvantages. For example, one faculty identifying as a man stated, “my lab runs way less effectively since I'm not there and the staff/trainees have limited and proscribed times to be at the bench.”
Gender disparities with funding
Women faculty said longstanding gender disparities contributed greatly to their reduced research productivity during COVID-19. One faculty identifying as a woman, and assistant professor: I feel that as a woman I frequently have less access to research opportunities because of my gender. During the pandemic, I have seen colleagues who are male being given opportunities to research projects related to COVID-19 and I send email inquiries and never hear back. As a woman, I have found it very hard to find mentorship and sponsorship in basic science research and become included in communities like graduate programs.
Collaboration/communication decreased
Faculty also identified that opportunities for collaboration and communication decreased during COVID-19, which affected their ability to do research. A faculty identifying as a woman and assistant professor shared: Communication is more difficult because you can't just go talk to someone. It all requires an appointment. Without communication, not as much gets done. In the research lab, hiring students has been difficult, and the shutdown/slowdown reduced experiments that could be done—less papers.
Men faculty also endorsed collaboration and communication as problems, but focused more on the ways other people were negatively interacting with them. One faculty identifying as a man stated: Interactions with faculty and collaborators have changed substantially in their tone. Everyone seems to be on edge and sometimes it feels like they don't have enough to do and are just irritable.
Productivity increased
Men faculty expressed that COVID-19 brought about opportunities to increase their research productivity. One faculty identifying as a man shared: I would say that my productivity has not been affected very much at all. Since there is not much else to do outside of work, and I don't spend time going to and from campus, I think I have been working more efficiently.
Some women faculty also stated that their productivity had increased, however this was mostly related to being allowed to have more flexibility in their multiple identities. One faculty identifying as a woman stated: My own productivity has increased while working from home. I work probably more hours during the week, but have more flexibility with family roles and can take more effective breaks.
Discussion
Overall, findings showed several patterns that reinforce existing gender disparities as well as intersectional disparities that have carried forward during COVID-19. 3,5,11 –23 Specifically, women faculty reported less emotional well-being, carried more service and clinical workload, and had lower levels of article and grant productivity, whereas men faculty generally reported higher emotional well-being, less service workload, and had higher levels of article and grant productivity. These results both reinforce and extend other recent findings on women faculty who are caregivers during COVID-19. Specifically, our findings support prior studies that have shown that women faculty with caregiving responsibilities report higher levels of depressive symptoms and lower levels of productivity. 20,41,42 Findings from the current study also extend prior results by showing that women faculty also report increased service and clinical responsibilities.
In addition, this study extends prior COVID-19 research by highlighting intersectional results. Specifically, results showed that women who identified as URM, caregivers, and assistant professors also reported less emotional well-being, carried more service and clinical workload, and had lower levels of article and grant productivity, whereas faculty without these multiple identities generally reported higher emotional well-being, less service workload, and had higher levels of article and grant productivity. Women at full professor level also reported an increase in service and clinical workload and a decrease in research productivity, including article and grants submission, whereas men faculty reported maintaining the same level of service, clinical workload, and grant submission. Women also reported fewer opportunities for research collaboration and leadership during COVID-19. The increased service workload among all women faculty is of concern as it can contribute to existing inequities in service work distribution among faculty and does not tend to be recognized in promotion and tenure requirements. 23
Qualitative findings support and provide a richer context for understanding the quantitative findings. These findings showed patterns such as all faculty experiencing increased workloads and less productivity, but the reasons for this were endorsed differently by gender. For example, reduced productivity identified by men was more focused on lower productivity of their staff and others, which then led to their own lower productivity. Whereas, women faculty identified their productivity was decreased due to the multiple intersections of their lived experiences (e.g., caregiver, woman, assistant professor). Although all workload is deemed important to the academic mission, workload more aligned with academic productivity, such as grants and articles, was more protected for men (senior faculty and noncaregiver) while service responsibilities were disproportionately distributed to junior faculty and women faculty. Ongoing evaluation and more equitable adjustment of service workload among faculty should be considered as we move beyond the early COVID-19 timeline.
Findings from this mixed-methods study may be useful for informing next steps for addressing gender disparities heightened by the pandemic. For example, creating more funding opportunities for women, URM, and assistant professor faculty would be essential to support these faculty in recovering from the disadvantages they experienced during the pandemic. In addition, providing more leadership opportunities for faculty with multiple lived experiences is important to stop the perpetuation of already existing gender and racial/ethnic disparities prepandemic, 11 –13,16 –19,42 as well as having an increased potential to reach transformative leadership that is often associated with women leaders. 43,44 Specifically, it will be important for faculty with multiple lived experiences whose perspectives are valued in this way to be offered leadership roles rather than simply “asked for feedback”; the latter perpetuates the idea of the “minority tax,” 45 which adds burden to those most affected to advocate for themselves or issues pertaining to their minoritized identity or DEI broadly.
Additionally, creating intentional rapid response plans for future public health crises such as ensuring more diverse faculty are involved in leadership positions that are responsible for decision making during crises and plans to support faculty well-being (with a focus on childcare issues), workload, and productivity during future public health crises would be essential.
Study findings also need to be interpreted in light of limitations of the study design. First, the survey response rate and overall sample size was small, collecting only 9% of the eligible population, thus generalizability to all UMN faculty is limited, as well as to faculty at other institutions. The UMN Medical School Office of Faculty Affairs 2020–2021 Academic Year Report 46 indicated our entire medical school population is 74% White, and 13.5% Asian (e.g., 87.5% Not URM; 12.5% URM). Although our sample size is closely proportional to our institution's population distribution, the sample was also limited by having small numbers of racially/ethnically diverse faculty. This may have limited our ability to capture robust intersectional results. Future research is needed with more racially/ethnically diverse faculty to confirm our findings. In addition, this survey was conducted mid-COVID, when in-person school attendance and daycare options were still limited and staffing shortages were common, and faculty responses may have differed if asked earlier or later during the pandemic.
Furthermore, the study is cross-sectional and it is unknown if these findings would be maintained longitudinally. Finally, although this study utilized emerging formats in data visualization that are best practice in prioritizing intersectionality in the summarization of data, there are mixed opinions on some of the data visualization techniques (e.g., radar charts). 47
In conclusion, study findings indicated that COVID-19's influence on faculty's well-being, workload, and productivity could not be fully understood without using an intersectional framework that allows for consideration of faculty's multiple lived experiences. These multiple lived experiences for women faculty in particular (e.g., caregiver, URM, assistant professor) were a key contributor to their experiences of lower well-being, increased workload, and decreased productivity during COVID-19. Interventions that include institutional policy change to course correct the disadvantages to faculty with multiple lived experiences during COVID-19 are important to allow for faculty well-being to be improved, workload to level out, and productivity to return to prepandemic levels.
Ethics Approval
This study was determined not to be human subject research (STUDY00010358: COVID-19 Health Sciences Faculty Survey) by the University of Minnesota IRB, 7/23/2020.
Footnotes
Authors' Contributions
All authors confirm they fit the ICMJE criteria for authorship. All authors made “substantial contributions to the conception or design of the work; or the acquisition, analysis, or interpretation of data for the work; AND Drafting the work or revising it critically for important intellectual content; AND Final approval of the version to be published; AND Agreement to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.”
J.M.B.: is the co-principal investigator of the study, conceptualized the article, assisted with data interpretation, wrote all drafts of the article, gave final approval of this version to be published, and agrees to be accountable for all aspects of the work regarding the accuracy or integrity of any part of the work.
R.L.F.: conducted the data analysis. She also critically reviewed the article, gave final approval of this version to be published, and agrees to be accountable for all aspects of the work regarding the accuracy or integrity of any part of the work.
K.M.: contributed to the design of the study and assisted with conceptualizing the survey, with data acquisition, analysis, and interpretation, and with writing and critically reviewing the article. She gave final approval of this version to be published and agree to be accountable for all aspects of the work regarding the accuracy or integrity of any part of the work.
S.W.: contributed to the design of the study and assisted with conceptualizing the survey, with data acquisition, analysis, and interpretation, and with writing and critically reviewing the article. They gave final approval of this version to be published and agree to be accountable for all aspects of the work regarding the accuracy or integrity of any part of the work.
S.P.: assisted with conceptualizing the survey and article, with data interpretation, and with writing and critically reviewing the article. She gave final approval of this version to be published and agrees to be accountable for all aspects of the work regarding the accuracy or integrity of any part of the work.
A.K.-B.: assisted with conceptualizing the survey and article, with data interpretation, and with writing and critically reviewing the article. She gave final approval of this version to be published and agrees to be accountable for all aspects of the work regarding the accuracy or integrity of any part of the work.
R.G.G.: assisted with conceptualizing the survey and article, with data interpretation, and with writing and critically reviewing the article. She gave final approval of this version to be published and agrees to be accountable for all aspects of the work regarding the accuracy or integrity of any part of the work.
K.L.: assisted with conceptualizing the survey and article and with writing and critically reviewing the article. She gave final approval of this version to be published and agrees to be accountable for all aspects of the work regarding the accuracy or integrity of any part of the work.
A.L.C.: assisted with conceptualizing the survey and article and with writing and critically reviewing the article. She gave final approval of this version to be published and agrees to be accountable for all aspects of the work regarding the accuracy or integrity of any part of the work.
R.D.: assisted with conceptualizing the survey and article, with data interpretation, and with writing and critically reviewing the article. She gave final approval of this version to be published and agrees to be accountable for all aspects of the work regarding the accuracy or integrity of any part of the work.
N.N.: assisted with conceptualizing the survey and article and with writing and critically reviewing the article. She gave final approval of this version to be published and agrees to be accountable for all aspects of the work regarding the accuracy or integrity of any part of the work.
C.M.: assisted with conceptualizing the survey and article, with qualitative data interpretation, and with writing and critically reviewing the article. She gave final approval of this version to be published and agrees to be accountable for all aspects of the work regarding the accuracy or integrity of any part of the work.
S.M.: assisted with conceptualizing the survey and article, with qualitative data interpretation, and with writing and critically reviewing the article. She gave final approval of this version to be published and agrees to be accountable for all aspects of the work regarding the accuracy or integrity of any part of the work.
E.A.R.: assisted with conceptualizing the survey and article and with writing and critically reviewing the article. She gave final approval of this version to be published and agrees to be accountable for all aspects of the work regarding the accuracy or integrity of any part of the work.
S.P.: assisted with conceptualizing the survey and article, with data interpretation, and with writing and critically reviewing the article. She gave final approval of this version to be published and agrees to be accountable for all aspects of the work regarding the accuracy or integrity of any part of the work.
S.S.: is the co-principal investigator of the study, contributed to the design of the study, assisted with conceptualizing the survey and article, with data interpretation, and with writing and critically reviewing the article. She gave final approval of this version to be published and agrees to be accountable for all aspects of the work regarding the accuracy or integrity of any part of the work.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This study was supported by the Medical School Office for Diversity, Equity, and Inclusion through the Center for Women in Medicine and Science (CWIMS), a Women's Center Gender Equity Grant (PI: Berge, Spencer) from the Women's Center at the University of Minnesota, a NIH Prize for Enhancing Faculty Gender Diversity in Biomedical and Behavioral Science (Berge, recipient), and a National Institutes of Health's National Center for Advancing Translational Sciences grant UL1TR002494. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health's National Center for Advancing Translational Sciences.
Supplementary Material
Supplementary Digital Appendix SA1
Supplementary Digital Appendix SA2
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.