
Abstract
Objective:
To investigate the triaging efficacy of the human papillomavirus (HPV) 16/18 E7 oncoprotein assay for high-grade cervical intraepithelial neoplasia (CIN2+) screening in HPV 16/18-positive patients in a tertiary hospital in China.
Methods:
We collected 476 cervical cell samples from women who tested positive for HPV 16/18 in the gynecological clinic of Peking Union Medical College Hospital between September 2018 and September 2022 and analyzed them by the HPV 16/18 E7 oncoprotein assay before colposcopy and biopsy. The study assessed the triaging efficacy of the HPV 16/18 E7 oncoprotein assay in HPV 16/18-positive patients by analyzing its performance against the gold standard of histologically confirmed CIN2+.
Results:
The positive rate of the HPV 16/18 E7 oncoprotein assay was 41.0% (114/278) in the negative for intraepithelial lesions and malignancy/CIN1 group and 80.3% (159/198) in the CIN2+ group. For triage of women with a positive HPV 16/18 test for CIN2+ detection, the HPV 16/18 E7 oncoprotein assay had a sensitivity, specificity, positive predictive value, and negative predictive value of 80.3%, 59.4%, 58.5%, and 80.9%, respectively. Furthermore, longitudinal follow-up of five patients showed a good correlation between the expression of the HPV 16/18 E7 oncoprotein and cervical lesion grades.
Conclusions:
As a triage method for HPV 16/18-positive patients, the HPV 16/18 E7 oncoprotein assay improves the specificity, reduces the colposcopy referral rate, and has the potential for long-term monitoring of high-grade CIN.
Introduction
Despite the availability of screening programs and preventive interventions, cervical cancer remains a serious public health problem worldwide and is the second most common gynecological cancer. 1 –3 Early screening plays an important role in the diagnosis and treatment of cervical intraepithelial neoplasia (CIN) and cervical cancer. Cervical cancer is a significant public health issue worldwide and is the second most common gynecological cancer, despite the availability of screening programs and preventive interventions. 1 –3 Screening for CIN is crucial for early detection and treatment of precancerous lesions before they develop into cervical cancer.
The recommended age range for cervical cancer screening varies by country but generally starts around age 25 years and continues until around age 65 years. Cervical cytology is one of the most commonly used screening techniques. The sensitivity and specificity of cytology are 53.0% and 96.5%, respectively. 4 In addition to the relatively low specificity, the drawbacks of cytology also include the inadequacy and uneven skill level of technical personnel. In addition to the low sensitivity, the drawbacks of cytology also include the inadequacy and uneven skill level of technical personnel. 5
To compensate for the drawbacks of cytology, in 2014, the World Health Organization (WHO) recommended the use of the high-risk human papillomavirus (Hr-HPV) test for cervical cancer screening in developing countries. 6 –8 However, ∼90% of human papillomavirus (HPV) infections are transient, which tends to result in low specificity. 9 Furthermore, HPV 16/18 has a higher risk than other HPV types, causing ∼70% of cervical cancer cases. 10 According to the American Society for Colposcopy and Cervical Pathology (ASCCP) guidelines, HPV 16/18-positive patients should be referred directly for colposcopy, whereas patients with other HPV types should undergo cytology triage before referral for colposcopy. 6
However, this tends to result in high rates of colposcopy referral for HPV 16/18-positive patients due to the characteristics of “transient” infection and low specificity of HPV testing. 11 Therefore, it is crucial to identify an accurate and efficient diagnostic method to triage patients who test positive for HPV 16/18.
According to a previous study, the integration of the HPV genome in the host cell results in overexpression of E6 and E7 oncoproteins, which are involved in the transformation and progression of cervical and other HPV-related cancers. 12 The persistent expression of viral protein E6 in conjunction with protein E7 is responsible for the oncogenic properties of Hr-HPV by promoting cell proliferation and malignant phenotypes. 13 Therefore, the E7 oncoprotein may be a potential marker for CIN. 14 In our previous study, 15 we set a positive cutoff value of 8.27 for the HPV 16/18 E7 oncoprotein, and the diagnostic effect of CIN2+ was pretested with a small sample size.
The results showed that the sensitivity and specificity were 70.6% and 67.9%, respectively. To further investigate the triaging efficacy of the HPV 16/18 E7 oncoprotein in HPV 16/18-positive patients for the diagnosis of CIN2+ in larger sample sizes, in this study, we analyzed the expression levels of the HPV 16/18 E7 oncoprotein in 476 HPV 16/18-positive samples, and the triaging effect of the HPV 16/18 E7 oncoprotein in HPV 16/18-positive samples was analyzed based on the gold standard of cervical pathology results (Fig. 1).
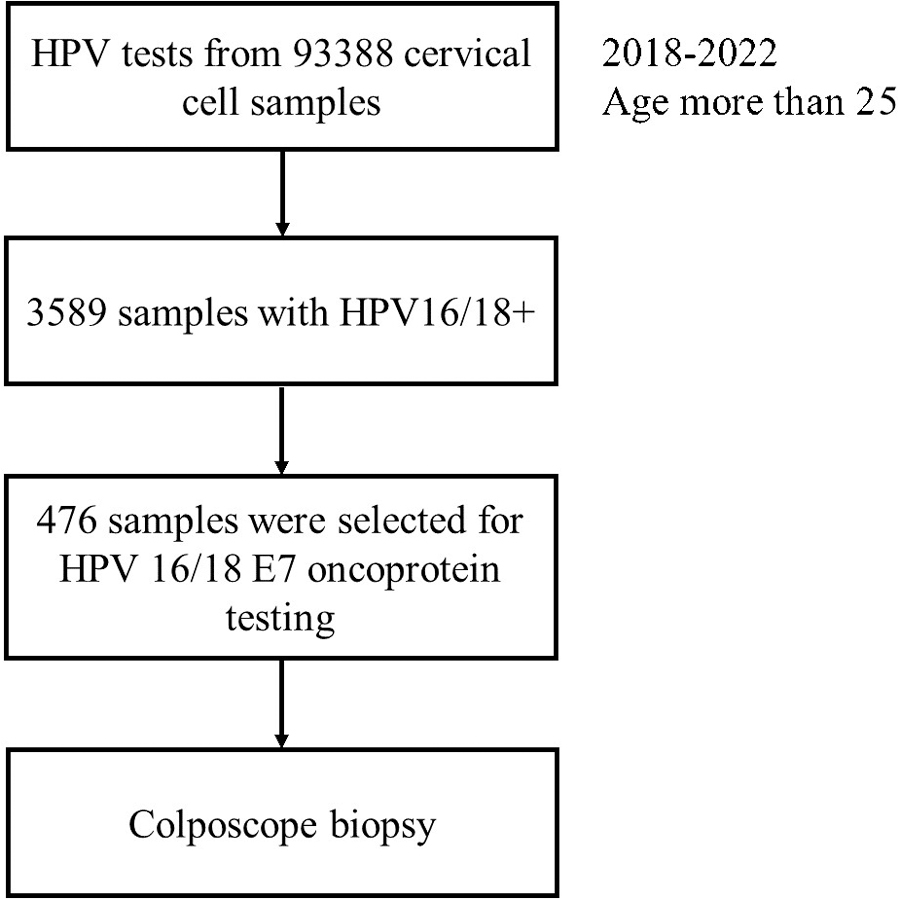
Flow chart of the study.
In this study, we aimed to further investigate the triaging efficacy of the HPV16/18 E7 oncoprotein in HPV 16/18-positive patients for the diagnosis of CIN2+. To achieve this, we analyzed the expression levels of the HPV 16/18 E7 oncoprotein in 476 HPV 16/18-positive samples and evaluated its effectiveness correlated with cervical histology.
Methods
Clinical data
We collected 476 cervical cell samples from women who tested positive for HPV 16/18 in the gynecological clinic of Peking Union Medical College Hospital between September 2018 and September 2022 and analyzed them with the HPV 16/18 E7 oncoprotein test before performing colposcopy and biopsy. The triaging effect of the HPV 16/18 E7 oncoprotein in HPV 16/18-positive samples was analyzed based on cervical pathology results. The triaging effect of the HPV 16/18 E7 oncoprotein in HPV 16/18-positive samples was assessed using histologically confirmed high-grade lesions (CIN2+) as the gold standard. The patients ranged in age from 25 to 80 (41.7 ± 10.9) years.
Hr-HPV DNA test
The Cobas 4800 HPV test (Roche Diagnostics, GmbH, Mannheim, Germany) is a qualitative test for the detection of HPV DNA, which was used to analyze the samples. This test amplifies target DNA in cervical epithelial cells by PCR and nucleic acid hybridization (Cobas PCR collection media, Roche Molecular Systems, Inc.) to detect 14 Hr-HPV types, of which HPV 16 and HPV 18 are of the greatest importance. The samples were analyzed using the Cobas 4800 HPV test (Roche Diagnostics, GmbH), a qualitative test for HPV DNA detection.
This test amplifies target DNA in cervical epithelial cells through PCR and nucleic acid hybridization (Cobas PCR collection media, Roche Molecular Systems, Inc.) to detect 14 high-risk HPV types, with separate genotyping of HPV 16 and HPV 18, which are considered to be of utmost importance. This analysis also enables the detection of Hr-HPV types 31, 33, 35, 39, 45, 51, 52, 56, 58, 59, 66, and 68 at clinically significant levels of infectivity.
HPV 16/18 E7 oncoprotein assay
The HPV 16/18 E7 magnetic particle-based chemiluminescence enzyme immunoassay kit from FAMID Biomedical Technology (Tianjin) Co., Ltd. was used to analyze the E7 oncoprotein level according to the instructions. The patients were instructed to refrain from intercourse and vaginal medication. The supernatant was collected for analysis within 2 hours. The assay used the double-antibody sandwich method, wherein magnetic particles were used as the solid phase of the immune response, and highly specific antibodies were used to detect high-risk E7 oncoprotein in cervical cell samples. An E7 oncoprotein test value >8.27 was considered a positive result, whereas a test value <8.27 was considered negative.
Pathological examination
All study participants underwent colposcopy-guided biopsy collection, and the obtained biopsies were histologically classified by two pathologists as negative for intraepithelial lesions or malignancy (NILM), CIN1, CIN2, or CIN3. For the purpose of estimating the sensitivity and specificity of the HPV 16/18 E7 oncoprotein test, CIN2 and CIN3 were classified as positive cases, whereas NILM and CIN1 were considered as negative cases.
Statistical analysis
Statistical analysis was performed using SPSS v25.0. The count data are presented as frequencies (n) and percentages (%). Sensitivity, specificity, positive predictive value (PPV), and negative predictive value (NPV) were calculated. Statistical significance was set at p < 0.05.
Ethics approval statement
The study was approved by the ethics committee of Peking Union Medical College Hospital (approval no. KS2022335), which was in compliance with the institutional and national policies for research approvals. All participants provided informed consent before enrolling in the study.
Results
In this study, pathologically, 172 samples were classified as NILM, 106 samples were classified as CIN1, 95 samples were classified as CIN2, and 103 samples were classified as CIN3 based on histology. HPV 16/18 E7 oncoprotein levels were analyzed in 476 cervical cytology samples.
Distribution of the positive rate of HPV 16/18 E7 oncoprotein expression in all samples
The HPV 16/18 E7 oncoprotein test showed a positivity rate of 24.4% (42/172) in the NILM group, 67.9% (72/106) in CIN1 cases, 84.2% (80/95) in CIN2 cases, and 76.7% (79/103) in CIN3 cases (Fig. 2). The positivity rate of HPV 16/18 E7 oncoprotein in the histological positive group (CIN2+ cases) was significantly higher than that of the negative group (NILM and CIN1) (41.0% [114/278] vs. 80.3% [159/198], p < 0.001).
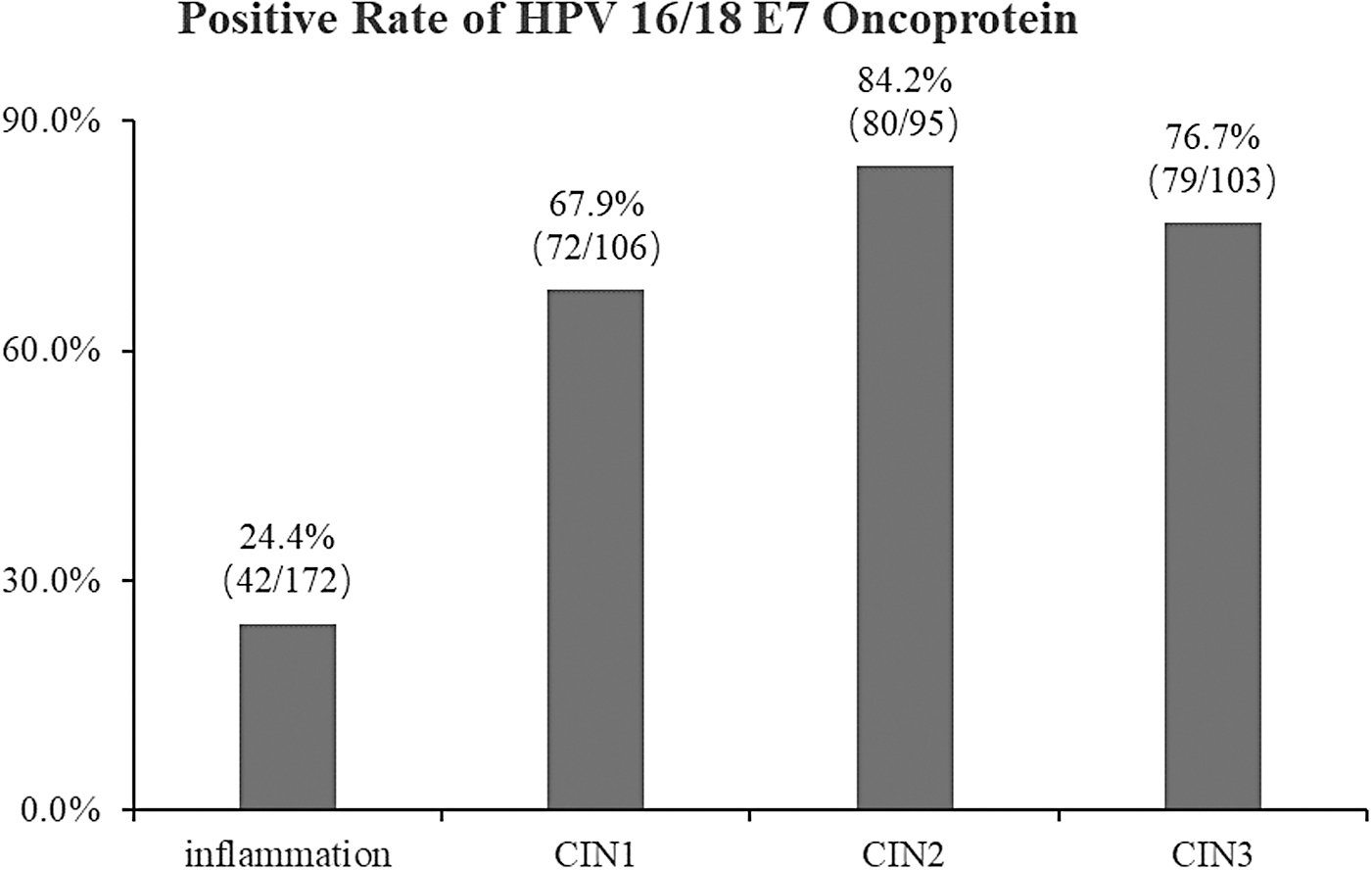
Positive rate of HPV 16/18 E7 oncoprotein in all samples. HPV, human papillomavirus.
Diagnostic efficacy of the HPV 16/18 E7 oncoprotein assay
For CIN2+ detection in HPV 16/18-positive patients, the HPV 16/18 E7 oncoprotein assay had a sensitivity, specificity, PPV, and NPV of 80.3%, 59.4%, 58.5%, and 80.9%, respectively. The number of colposcopies for the HPV 16/18 E7 oncoprotein positive for detecting one case of CIN2+ was 1.71 (Table 1).
Diagnostic Efficacy of Cervical Intraepithelial Neoplasia 2+ by Human Papillomavirus (HPV) 16/18 E7 Oncoprotein and HPV 16/18 Testing
CIN, cervical intraepithelial neoplasia; HPV, human papillomavirus; NPV, negative predictive value; PPV, positive predictive value.
Longitudinal follow-up of five patients with persistent HPV 16 infection
To further investigate the potential of HPV 16/18 E7 oncoprotein testing as a predictor of cervical disease development and prognosis, we performed longitudinal follow-up testing on five patients with persistent HPV 16 infection, 1 year after the initial test.
Of these patients, three showed negative HPV 16/18 E7 oncoprotein results on two successive tests (1 year apart), and were classified as NILM based on histological findings. One patient had a positive HPV 16/18 E7 oncoprotein result at the first visit (with a test value of 11) and histological findings of CIN1, but tested negative at the second visit (14 months later) with histological findings of NILM.
One patient had consecutive positive HPV 16/18 E7 oncoprotein results, with a first test value of 10 and histological findings of CIN1, and a second test value of 47 (1 year later) corresponding to histological findings of CIN2 (Table 2). These results suggest that HPV 16/18 E7 oncoprotein testing may have potential as a predictor of cervical disease development and progression.
Longitudinal Follow-Up of Five Patients with Persistent Human Papillomavirus 16 Infection
HPV 16/18 E7 oncoprotein test value >8.27 was considered positive.
Discussion
The referral of women who test positive for HPV 16 and 18 for colposcopy without the use of cytology in triage is recommended in many countries 6 ; however, this approach often leads to a high rate of unnecessary colposcopy referrals due to the relatively low specificity of the test. 11 Consequently, the development of objective and accurate triage options is a major focus in cervical cancer screening. The HPV-encoded E7 oncoprotein is a major driver of HPV oncogenic activity, and elevated expression of the E7 oncoprotein can lead to oncogenic transformation. 16
In this study, the HPV 16/18 E7 oncoprotein assay was utilized as a triage test for women who tested positive for HPV 16 or 18 DNA. The sensitivity and specificity of the assay for detecting CIN2+ cases were 80.3% and 59.4%, respectively. Both the sensitivity and specificity were much higher than those of the HPV 16/18 test alone in the ATHENA (Addressing THE Need for Advanced HPV diagnostics) study (51.8% and 20.4%). 17 Besides, a similar study by Sørbye et al. 18 reported that when triaging HPV DNA-positive patients, the sensitivity and specificity (CIN2+) of a 7-type HPV-mRNA test were 76.1% and 71.0%, respectively.
In addition, when combined with the HPV 16/18 E7 oncoprotein, the PPV and NPV were 58.5% and 80.9%, respectively, and the referral number for detecting one CIN2+ was as low as 1.71. However, the referral number for detecting one CIN2+ was 2.38 for HPV 16/18 testing only. These results suggested that the HPV 16/18 E7 oncoprotein assay could be a good triage method for HPV 16/18-positive patients, which could greatly increase the sensitivity and specificity and reduce the colposcopy referral rate.
In addition, in this study, the positive rates of the HPV 16/18 E7 oncoprotein in patients with NILM and CIN1 were 24.4% and 67.9%, respectively. Although the expression of the HPV 16/18 E7 oncoprotein was lower than that in CIN2 and CIN3, it was still quite high. The possible reason may be that ∼1.6%–11.7% of NILM and 10%–30% of CIN1 lesions progress to CIN2–CIN3, 9,19 –22 and the positive HPV 16/18 E7 oncoprotein in NILM and CIN1 may indicate the possibility of developing into CIN2+.
Therefore, the HPV 16/18 E7 oncoprotein may be used as a potential monitoring indicator to predict the development of CIN2, and its follow-up monitoring value may be more important than its diagnostic value. To explore the significance of the HPV 16/18 E7 oncoprotein for longitudinal continuous detection and whether it can be used to predict the future development of NILM and CIN1, it is necessary to further detect the expression of the HPV 16/18 E7 oncoprotein in large-scale NILM and CIN1 samples.
In addition, the five patients underwent follow-up testing of the HPV 16/18 E7 oncoprotein 1 year after the first test in this study, and the results showed that the expression of the HPV 16/18 E7 oncoprotein correlated well with cervical lesion grades. Although there were only a few cases, it could be inferred that the HPV 16/18 E7 oncoprotein has potential predictive value as an indicator for long-term monitoring, and a larger sample size is needed in the future for longitudinal experiments.
The positive rate of the HPV 16/18 E7 oncoprotein in CIN2 was 84.2%, which was higher than that in CIN3 (76.7%), mainly because the HPV 16/18 E7 oncoprotein is more active at the beginning of tumor progression, which mainly promotes the formation of benign tumors and plays a relatively weak role in the progression of malignant transformation. 23 Therefore, the HPV 16/18 E7 oncoprotein is more sensitive in screening for CIN2, which is the focus of clinical screening for cervical precancerous lesions.
Moreover, HPV 16/18 E7 oncoprotein expression was negative in 39 CIN2/CIN3 cases (39/198, 19.7%). In our preliminary experiment, 15 we analyzed the false-negative results of the HPV 16/18 E7 oncoprotein in seven CIN2+ samples. One of the seven samples (CIN3) showed substantially intact cells, with low HPV 16/18 E7 oncoprotein expression in a few cells, as well as some cell fragmentation and protein release. These data indicated that sampling has a significant impact on the E7 protein assay, suggesting that it is important to standardize the sampling procedures to ensure optimal number of cells and integrity for the HPV 16/18 E7 oncoprotein assay.
In addition, the real purpose of our study was to screen for CIN2 and CIN3, not to screen for visible tumors and invasive cancer samples, which need biopsy rather than protein detection. In our preliminary experiment, the detection results of cancer and microinvasion were not good, which showed significant cell fragmentation with few normal cells and very low HPV 16/18 E7 oncoprotein expression due to cell fragmentation. Furthermore, to better and more comprehensively assess the triaging effect of HPV 16/18 E7 oncoprotein, we will develop our protocols and conduct follow-up studies on patients who test positive HPV 16/18 but have lower titers of the HPV 16/18 E7 oncoprotein.
There are also some limitations in this study. First of all, the sample size of this study is relatively small and it is a single-center study, making the data less convincing. Therefore, in our further analysis, a multicenter study with a significantly larger experiments will be carried out in the near future to verify the findings of this study. Second, the sensitivity and specificity obtained in this study were not very ideal, with a sensitivity and specificity for diagnosing CIN2+ cases of 80.3% and 59.4%, respectively. Last but not least, due to the limitations of time and conditions, this study is a cross-sectional study on the whole, longitudinal experiments with a larger sample size could better demonstrate the predictive value of HPV 16/18 E7 oncoprotein for long-term monitoring
Conclusion
In conclusion, utilizing the HPV 16/18 E7 oncoprotein assay as a triage test for women with positive HPV DNA 16/18 test results enhances specificity and reduces the rate of unwarranted colposcopy referrals for high-grade CIN detection. In addition, it shows promise for long-term monitoring of high-grade CIN, but additional research is required to explore this possibility further.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.