
Abstract
Objective:
Maximizing preconception health is an important strategy to prevent preeclampsia in pregnancy. Preeclampsia remains a significant cause of maternal and fetal morbidity and mortality. We examined the associations between preconception maternal body weight, body mass index (BMI), and blood pressure with preeclampsia and its related outcomes.
Materials and Methods:
We performed a retrospective review of 11,214 live births from 6 months preconception during 2009–2018 in the University of Washington medical system. Outcomes were analyzed using chi-square, analysis of variance, and t-tests. Binary logistic regression was performed to examine associations.
Results:
Of 11,214 births, 1,539 (13.7%) were complicated by preeclampsia. Individuals with preeclampsia weighed more and had higher blood pressure from 6 months preconception to at least 6 months of pregnancy compared with those without preeclampsia (p < 0.001). Persons with prepregnancy systolic blood pressure (SBP) ≥130 mmHg were 3.2 times more likely to develop preeclampsia than those with SBP <130 mmHg (adjusted odds ratio [aOR] = 3.24, 95% confidence interval [CI] = 2.37–4.43). Women with prepregnancy BMI ≥30 kg/m2 were 2.3 times more likely to develop preeclampsia (aOR = 2.31, 95% CI = 1.72–3.10) than those with BMI <30 kg/m2. Mothers with preeclampsia were more likely to deliver preterm (29% vs. 13.8%, p < 0.001) and have neonates with 5-minute Apgar scores <8 (22.1% vs. 12.1%, p = 0.02) and lower preterm birthweights (1,909 g, 95% CI = 1,813–2,004 g vs. 2,057 g, 95% CI = 1,989–2,123 g).
Conclusions:
Maternal obesity and elevated blood pressure from 6 months preconception to 6 months of pregnancy were associated with preeclampsia, resulting in maternal and fetal complications.
Introduction
Preeclampsia affects 5%–8% of pregnancies worldwide. 1 It is the leading cause of prematurity and fetal growth restriction, and the mortality of newborns born to mothers with preeclampsia is five times greater than those born to mothers without preeclampsia. 2 Approximately 50,000 pregnant persons worldwide die from preeclampsia and its complications annually, and preeclampsia is the second leading cause for peripartum intensive care unit admission after hemorrhage.1,2 Several maternal and pregnancy-related risk factors for preeclampsia have been identified, including chronic hypertension and obesity.3–5 Specifically, up to 20%–50% of individuals with chronic hypertension will develop preeclampsia, and the risk of preeclampsia is five to six times higher in individuals with chronic hypertension than in individuals without a diagnosis.3,4 Individuals with obesity (body mass index [BMI] ≥30 kg/m2) are up to three times more likely to develop preeclampsia than those with a normal weight and are at increased risk of cardiovascular events following pregnancy. 5
Several studies have described and quantified the interactions of maternal weight, BMI, and chronic hypertension with preeclampsia with varying risk calculations and certain limitations.6–22 Savitri et al. observed that higher prepregnancy BMI was associated with higher pregnancy systolic blood pressure (SBP = 0.25 mmHg/kg/m2, 95% confidence interval [CI] = 0.17–0.34 mmHg/kg/m2), and that every 1 kg/m2 increase in prepregnancy BMI was associated with a 9% higher odds of developing preeclampsia (adjusted odds ratio [aOR] = 1.09, 95% CI = 1.04–1.14). 10 Shao et al. found that individuals with a prepregnancy BMI ≥30 kg/m2 had a 81% higher odds of developing preeclampsia in pregnancy (OR = 1.81, 95% CI = 1.81–2.39), 22 whereas Bodnar et al. reported that a prepregnancy BMI ≥30 kg/m2 conferred a 2.9 times higher odds of preeclampsia (aOR = 2.9, 95% CI = 1.6–5.3). 15
Although the magnitude of preeclampsia risk varies by methodological design and patient population, it is clear there is an intimate link between obesity and preeclampsia, and some groups have even proposed incorporating BMI as a way to diagnose preeclampsia, in conjunction with blood pressure criteria. 12
However, few studies have stratified the associations of elevated blood pressure and weight at timepoints spanning the preconception period and throughout pregnancy. The previously cited studies were limited by cross-sectional reporting of data, use of data from initial prenatal visits as preconception proxies (most before 16 weeks gestational age), or patient self-reporting of prepregnancy weight, which is often underestimated. 23 Certain studies also report total weight gain in pregnancy as the primary exposure, which can introduce reverse causality bias, as edema resulting in weight gain is also a consequence of preeclampsia. 2 There is a need for more accurate extraction of prepregnancy obesity and blood pressure parameters. Changes in maternal blood pressure and weight over time beginning at 6 months preconception through early pregnancy are an underexplored area of research and offer opportunities for detection and prevention of hypertensive disorders of pregnancy. 7
In addition, The American College of Obstetricians and Gynecologists (ACOG), the national governing body that creates practice guidelines, acknowledges that its definitions of pregnancy-induced hypertension (≥140/90 mmHg) differ from stage 1 chronic hypertension as defined by The American Heart Association (AHA) and The American College of Cardiology (ACC) as blood pressures ranging from 130 to 139 mmHg (systolic) or 80 to 89 mmHg (diastolic). 24 This is an area of active investigation; for example, Li et al. demonstrated that individuals with stage 1 hypertension prepregnancy were 95% more likely to develop preeclampsia (aOR = 1.95, 95% CI = 1.45–2.60) compared with normotensive individuals. 6 Thus, there is a need to further study obstetric implications of stage 1 hypertension.
Given the maternal and fetal morbidity of preeclampsia, greater understanding of modifiable risk factors, such as maternal weight and blood pressure, in the preconception period is likely to improve risk assessment, better inform counseling, and prevent or mitigate development of preeclampsia. We therefore examined births between 2009 and 2018 in the University of Washington (UW) medical system to evaluate the associations between maternal weight, BMI, and blood pressures from 6 months preconception to at least 6 months of pregnancy in patients with and without preeclampsia. We predicted there would be a significant difference in these parameters as early as 6 months preconception and that prepregnancy obesity and stage 1 hypertension would be associated with increased risks of preeclampsia and its associated maternal and fetal complications in pregnancy.
Materials and Methods
This was a retrospective cohort study of 11,214 births in the UW system from 2009 to 2018. It included all live births with maternal blood pressure and obesity parameters documented at least 180 days (or 6 months) preconception. Our database did not report fetal demises or stillbirths. Unrealistic weights (<30 and >400 kg) and blood pressures (systolic <50 mmHg, diastolic <30 mmHg) were excluded owing to likelihood of data error. This study was approved by the UW Internal Review Board. Patient consent was waived.
Our primary outcome of interest was preeclampsia, and exposures were maternal weight, BMI, and blood pressure (including systolic and diastolic values). BMI categories were classified according to the Centers for Disease Control and Prevention. Secondary variables included maternal demographic variables (age, race, parity), preexisting maternal conditions (gestational diabetes, pregestational diabetes, gestational hypertension, chronic hypertension, depression), gestational weight gain category (recommended by the Institute of Medicine [IOM] based on prepregnancy BMI), gestational age at delivery, mode of delivery, infant birth weight, and 5-minute Apgar score. All data were extracted from the electronic medical records, and the following variables were extracted at prespecified timepoints preconception and in pregnancy: maternal weight 0–180 days before conception, 0–60 days before conception, 174–194 days of pregnancy, 8–14 days before birth, and 9–17 days before birth; and maternal blood pressure 0–180 days before conception, 0–30 days of pregnancy, 31–60 days of pregnancy, and 174–194 days of pregnancy.
Prepregnancy maternal height and weight were obtained and recorded by a medical assistant or nurse during a clinic visit. BMI was calculated as the ratio of weight (kg) divided by height (m2). If no prepregnancy weight or blood pressure was available, data from the first 60 days of gestation was used, and if multiple weights or blood pressures existed within the period, the mean of the values was used. Hypertensive disorders of pregnancy were coded by the International Classification of Diseases Tenth Revision (ICD-10) in accordance with the diagnostic criteria established by ACOG. Preeclampsia was not distinguished by presence or absence of severe features.
For this study, several covariates of interest were extracted. Self-reported race was collected as Asian, Black, White, or other. Age was categorized as ≤20 years, between 20 and 35 years, or ≥35 years old. Parity was classified as nulliparous or multiparous. Maternal conditions were also extracted using ICD-10 codes and included preeclampsia, chronic hypertension, gestational hypertension, gestational diabetes, pregestational diabetes, and obesity (BMI ≥30 kg/m2). Presence of these comorbidities was recorded as “yes” if present and “no” if absent.
An assessment of the data was carried out at the time of exploratory data analysis, and the data were checked for missing variables, distributional assumptions, and outliers. Variables were incorporated for analysis if they had adequate sample sizes based on predetermined power calculations. Based on the prevalence of preeclampsia from the literature, a sample size of 1,015 participants was required for a logistic regression with a power of 80% and alpha of 0.05. 1 Descriptive statistics were used to describe our study population. Several sociodemographic and clinical characteristics were compared between the groups with and without preeclampsia, and their frequencies were determined. Differences between the two subgroups were then assessed using chi-square, analysis of variance, or t-tests as appropriate for the type of variable. Stratification analysis was completed at the prespecified timepoints before and in pregnancy.
Binary logistic regression was performed using the following potential predictors: maternal age, maternal race, parity, maternal BMI category, gestational weight gain category, and SBP to estimate the odds of preeclampsia with each exposure and account for potential confounders of preeclampsia. Statistical significance was set at p < 0.05, and ORs and aOR were calculated with 95% CIs. IBM SPSS software was utilized for all statistical tests.
Results
A total of 11,214 live births were recorded between 2009 and 2018 at UW. Many of these pregnancies had a diagnosis of either a pregestational or pregnancy-related complication (3,406, 30.4%), of which 1,539 (13.7%) had a diagnosis of preeclampsia. Very few pregnant persons diagnosed with preeclampsia had no other complication (4.1%) with most individuals having two or more additional complications (78.2%; Table 1). The demographic characteristics of the entire sample and subsamples are given in Table 2.
Risk of Preeclampsia by Preexisting Maternal Conditions

Demographic Characteristics of the Entire Sample and Subsets

BMI, body mass index; IOM, Institute of Medicine.
There were 1,796 persons with a diagnosis of chronic hypertension (16.0%) and 1,673 persons with a diagnosis of gestational hypertension (14.9%). Most people with preeclampsia also had superimposed chronic hypertension compared with those without preeclampsia (90.3% vs. 4.2%, p < 0.001). Individuals with chronic hypertension were more likely to develop preeclampsia than those without a diagnosis (77.4% vs. 1.6%, p < 0.001). Similarly, majority of those who had a diagnosis of gestational hypertension developed preeclampsia compared with those without a diagnosis (72.0% vs. 3.5%, p < 0.001). Women with preeclampsia had elevated mean systolic and diastolic blood pressures at all timepoints spanning 6 months preconception into the first and second trimester of pregnancy (Table 3). However, the mean blood pressures for women with preeclampsia were still within the normal pregnancy range during this time, defined as blood pressures ≤140/90 mmHg.
Mean Maternal Systolic and Diastolic Blood Pressures (±Standard Deviation) for Women Prepregnancy and During Pregnancy with and Without a Diagnosis of Preeclampsia
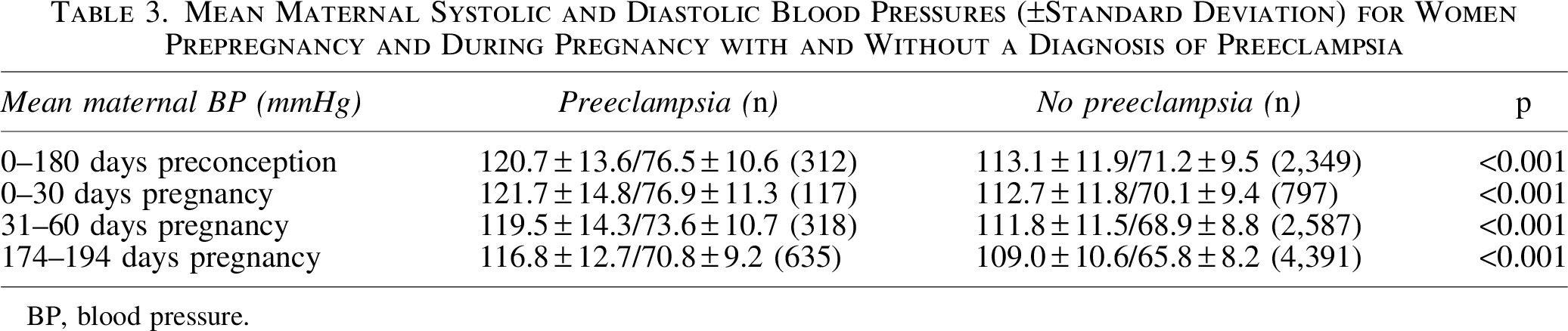
BP, blood pressure.
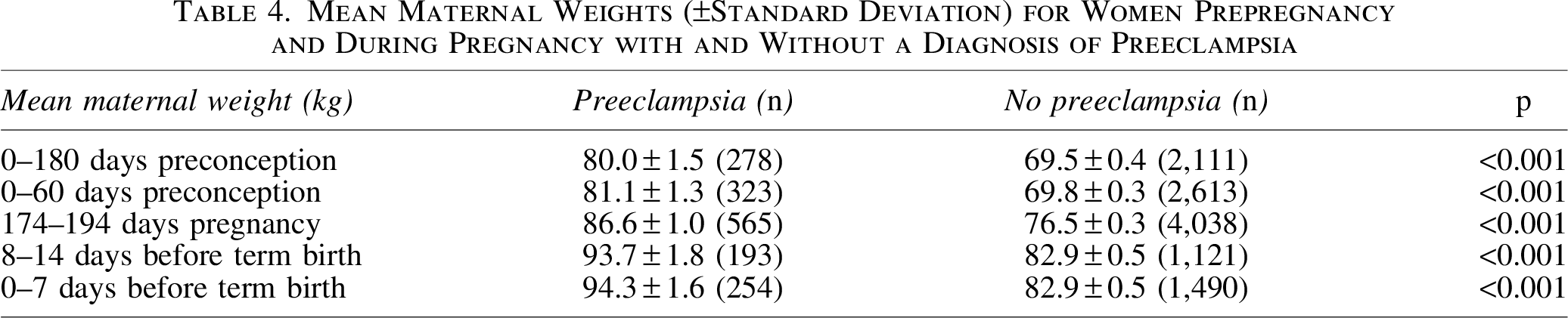
On average, the preeclampsia group was heavier (81.6 ± 1.5 kg vs. 70.5 ± 0.5 kg, p < 0.001) and had a higher BMI (30.3 ± 0.5 kg/m2 vs. 26.2 ± 0.2 kg/m2, p < 0.001) than the group without preeclampsia. Persons who developed preeclampsia weighed significantly more than those without a diagnosis at timepoints spanning 6 months preconception to within 1 week of birth (Table 4). Individuals with a prepregnancy BMI ≥30 kg/m2 were more than twice as likely to develop preeclampsia as those with a normal weight (27.1% vs. 11.5%, p < 0.001). The proportion of women who developed preeclampsia also increased consistently with increasing BMI category (p < 0.001; Fig. 1). People who gained weight above the IOM's gestational weight gain (GWG) recommendations were more likely to develop preeclampsia as compared with those within the GWG goal (17.7% vs. 10.9%, p < 0.001).

Proportion of women who developed preeclampsia by BMI category. BMI, body mass index.
Mean Maternal Weights (±Standard Deviation) for Women Prepregnancy and During Pregnancy with and Without a Diagnosis of Preeclampsia
Of the 2,788 individuals with all available parameters (age, parity, race, gestational weight gain category, BMI, and SBP) for our binary logistic multivariate regression model, we found that only BMI category and SBP were significant. Every increase in initial SBP by 1 mmHg increased the odds of developing preeclampsia in pregnancy by 4.8% (aOR = 1.048, 95% CI = 1.04–1.06). Individuals with a prepregnancy SBP ≥130 mmHg were 3.2 times more likely to develop preeclampsia in pregnancy compared with those with SBP <130 mmHg (aOR = 3.24, 95% CI = 2.37–4.43). Persons classified as overweight prepregnancy were 45% more likely to develop preeclampsia (aOR = 1.45, 95% CI = 1.07–1.96), and those classified as obese prepregnancy were 2.3 times more likely to develop preeclampsia (aOR = 2.31, 95% CI = 1.72–3.10) compared with those with normal weight before pregnancy.
Mothers with preeclampsia were more likely to deliver preterm (29% vs. 13.8%, p < 0.001) than those without the disease. Neonates of mothers with preeclampsia also had a higher proportion of 5-minute Apgar scores <8 (22.1% vs. 12.1%, p = 0.02, n = 728). When comparing birthweights in pregnancies with and without preeclampsia, there was a significant difference between birthweight among preterm neonates (p = 0.02), but no difference between term neonates (p = 0.20). The mean birthweight for preterm babies without preeclampsia was 2,057 g (95% CI = 1,989–2,123 g, n = 626) and 1,909 g for those with preeclampsia (95% CI = 1,813–2,004 g, n = 269). The mean birthweight for term deliveries without preeclampsia was 3,403 g (95% CI = 3,388–3,418 g, n = 4,135) and 3,376 g (95% CI = 3,334–3,419, n = 717) for those with preeclampsia.
Discussion
Our study found that individuals who developed preeclampsia in pregnancy had significantly higher BMI, weight, and blood pressures as early as 6 months preconception compared with normotensive women. These trends persisted through the first and second trimester of pregnancy. Although these variables have been identified as risk factors for preeclampsia in previous research, our study quantified these associations at multiple timepoints before and during early pregnancy. Our finding supports the theory of pregnancy as a metabolic stress test that can unmask preexisting subclinical disease and that more comprehensive preconception care is necessary to maximize maternal, fetal, and neonatal health in pregnancy. 25 The findings of our study are significant because they describe the interplay of maternal weight and blood pressure parameters with preeclampsia during a preconception window that has not been previously studied, offering a more accurate representation of prepregnancy health and risk for subsequent pregnancy complications.
We found that women who developed preeclampsia weighed more with higher BMI beginning at 6 months preconception and that a prepregnancy BMI ≥30 kg/m2 was associated with preeclampsia. The OR we observed was in the similar range as previous works that incorporated prepregnancy values from patients' first antenatal visit.5,9–11,13,15,19,21,22 Our study demonstrates that prepregnancy obesity metrics of maternal BMI, weight, and recommended gestational weight gain are all significant when comparing pregnancies with and without preeclampsia and therefore offer clinical utility for informing patient counseling. It also supports emerging work that obesity may be used as diagnostic aide for preeclampsia along with blood pressure criteria. 12
In addition, the preeclampsia group had elevated systolic and diastolic blood pressures at all timepoints spanning 6 months preconception into ∼6 months of pregnancy. We explored the subgroup of individuals with stage 1 hypertension and determined that having a prepregnancy SBP ≥130 mmHg contributed to greater preeclampsia risk than a SBP <130 mmHg. This finding directly supports work by Li et al. that suggested an increased risk of preeclampsia with stage 1 hypertension in a similar large, high-risk cohort. 6 Emerging clinical trials demonstrate that treating chronic hypertension with a blood pressure target of <140/90 mmHg results in decreased adverse pregnancy outcomes, including preeclampsia. 26 As a result, current diagnostic and treatment guidelines for pregnancy-induced hypertension are being challenged.
Of note, the mean systolic and diastolic blood pressures for individuals who developed preeclampsia in our study were in the normal range although still significantly higher than those without preeclampsia. We hypothesize that elevated but normal blood pressure ranges may underestimate preeclampsia risk and warrant maternal and fetal surveillance with interpretation of patients' overall risk for preeclampsia, maternal weight parameters, blood pressure trend, gestational age, and fetal status.
Preeclampsia coexisted with multiple other complications in our pregnant population, including chronic hypertension, gestational hypertension, pregestational diabetes, gestational diabetes, and depression. Regarding fetal risks, we found that individuals with preeclampsia were more likely to experience premature delivery, give birth to neonates with lower 5-minute Apgar scores (<8), and have lower mean birthweights for preterm deliveries as compared with those without preeclampsia. These findings corroborate past work and emphasize the maternal and fetal morbidity associated with preeclampsia.1,2,5,27–29
Strengths of our study include its large, diverse sample size and a high-risk obstetrics setting. The database included 11,000 pregnant persons with sociodemographic representation mirroring that of the reproductive-aged U.S. population.30,31 The percentage of pregnancies impacted by preeclampsia in our study was higher than the national and global rates (13.7% vs. 5%–8%). 1 Our study population is applicable to most academic and referral centers in the United States, and we argue that there is a greater need to study and prevent consequences of preeclampsia in these settings. We also had access to comprehensive and longitudinal reporting of variables of interest and confounding variables for rigorous analyses. Of importance, prepregnancy maternal weight, BMI, and blood pressure were extracted from the electronic health records, a limitation of past studies owing to patient self-reporting and reliance on prepregnancy proxy variables (e.g., antenatal visit data in the first or second trimester of pregnancy).
Our study was limited by its retrospective nature and incomplete data in the electronic health records. We therefore excluded variables that were insufficiently reported. To reduce the effects of confounding variables and capture temporal exposures, we performed binary logistic regression and stratification analysis, although residual confounders likely exist owing to the study's observational design. These associations will require further prospective validation but raise the potential for improving risk assessment, prevention, diagnosis, and treatment of preeclampsia. Other limitations of our database include lack of reporting of certain variables, such as fetal demises and stillbirths. We anticipate that the number of fetal demises and stillbirths was very small relative to the number of live births based on available literature.32,33
A next step for our study is to further subclassify our observed associations with preeclampsia by obesity class (i.e., class I, II, and III) and type of preeclampsia (i.e., with and without severe features, early or late onset). Additional research questions are to determine how early lifestyle and medical interventions affect preeclampsia risk, and whether there is an association with other clinical outcomes, such as gestational age at delivery, mode of delivery, birthweight, and neonatal intensive care unit admission. Extended long-term follow-up of mothers in the 12 weeks postpartum (i.e., fourth trimester) is also an understudied and critical period with potential to impact maternal cardiovascular health. Finally, further identification of modifiable and nonmodifiable factors influencing preeclampsia risk may promote effective public health interventions, such as ambulatory blood pressure monitoring and nutritional counseling. Future efforts can determine the efficacy of these preventative measures.
Our study findings suggest that patients with a prepregnancy BMI ≥30 kg/m2 should be counseled to reduce their weight before conception to decrease their risk for preeclampsia, and obese patients who are beginning pregnancy should be monitored closely for the development of preeclampsia. Patients with a diagnosis of chronic hypertension should be strongly counseled and supported to optimize blood pressure control in the preconception period. Moreover, patients with borderline elevated blood pressures, or stage 1 hypertension, may benefit from more frequent and earlier supervision by their obstetricians and primary care providers with stricter blood pressure control in the 6 months before conception.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This project is supported by the Health Resources and Services Administration (HRSA) of the U.S. Department of Health and Human Services (HHS) under cooperative agreement U4DMC39438: Pregnancy-Related Care Research Network. Dr. Jelin is supported by K23DK119949 from the NIH/NIDDK.
Disclaimer
The contents of the publication are solely the responsibility of the authors and do not necessarily represent the official views of the NIH, HRSA, HHS, or the U.S. Government.