
Abstract
Objective:
The presence of disparities in access to health care and insurance coverage can have a tremendous impact on health care outcomes. Programs like the Affordable Care Act were implemented to improve health care access and to address the existing inequities. The objective of this study was to identify any disparities that exist between males and females regarding health care coverage and out-of-pocket cost to health care.
Methods:
This analysis was a cross-sectional study using the Behavioral Risk Factor Surveillance System survey data collected between 2013 and 2018. The primary predictor was sex assigned at birth (with the binary option of male vs. female). The primary outcome was adequate health coverage. Survey participants who indicated that they had health insurance with no out-of-pocket cost barriers to receiving medical care were considered to have adequate health coverage, while participants who did not meet these criteria were considered to have inadequate health coverage. Covariates measured were age, race/ethnicity, educational level, employment status, and annual household income. SAS survey procedures and weighting methods were used to measure the association between the sex and adequate health coverage, after controlling for covariates.
Results:
The data spanning 6 years included 2,249,749 adults, of whom 1,898,097 (84.4%) had adequate health coverage. Females made up 55.8% (N = 1,256,243) of the total sample. About 32.6% (N = 733,216) survey participants were aged ≥65 years. Most respondents, 77.6%, were White (Non-Hispanic). Across the 6-year period, females were more likely to have health insurance but with out-of-pocket costs that served as a barrier to their medical care (adjusted odds ratios with 95% CI from 2013 to 2018 were 1.36 [1.29–1.43], 1.38 [1.32–1.46], 1.31 [1.24–1.38], 1.33 [1.26–1.40], and 1.32 [1.25–1.40], respectively).
Conclusions:
Females were more likely than males to indicate an out-of-pocket cost barrier to medical care despite having health insurance.
Introduction
Disparities in health care access and health coverage can greatly affect health care outcomes, quality of life, and medical costs. Before the Affordable Care Act (ACA) in 2010, many women were unable to find adequate insurance to cover essential preventative and reproductive health needs. 1,2 After the implementation of the ACA, the overall uninsured rate in 2015 dropped to 9.1% from 16% in 2010. 3 After the ACA expansion in 2014, the uninsured rate of females improved from 17% to 11% in 2016. 1 Women of reproductive age also had uninsured rates drop from 18.9% to 11.5% from 2012 to 2015, about a 40% reduction. 3,4 Moreover, a study by Chen et al. further showed a significant reduction in disparities among ethnic and racial minorities in access to care following the ACA from 2011 to 2014. 5
Despite overall reduction in uninsured individuals, some people with insurance still experienced out-of-pocket medical costs that were a barrier to care. Low-income individuals and families are particularly vulnerable to out-of-pocket costs. This may deter them from seeking certain kinds of health care depending on their specific insurance plan, which often vary by state. For example, some women have found challenges in coverage of maintenance therapies, for example chemotherapy for breast and lung cancer. 1,6
Even with improvements in uninsured rates, racial and ethnic disparities have persisted following the ACA. 3 An additional study that evaluated the effects of the ACA on women of reproductive age found that Latina women did not experience any improvement in insurance coverage following the ACA. 4 Another study analyzing secondary data from the National Health Interview Study from 2006 to 2014 showed that Black women had the most unmet health care needs compared with other groups, even after the ACA went into effect. 7 In addition to racial disparities, Jones and Sonfield found that in reproductive age women who were employed less than full time and obtained less education had higher rates of being uninsured as compared with non-White women. 4
Striving to understand health coverage and out-of-pocket cost barriers is necessary for guiding policy as it relates to individual and population health. The aim of this study is to identify any disparities from 2013 to 2018 that exist between females and males regarding health care coverage and out-of-pocket cost barriers to health care.
Methods
Study design
This is a cross-sectional study using data from the Behavioral Risk Factor Surveillance System (BRFSS) surveys collected between 2013 and 2018. The BRFSS data are collected annually from all 50 states of America as well as the District of Columbia and 3 U.S. territories. Each year, >400,000 adults are interviewed through telephone calls. 8 BRFSS obtains data with a computer-assisted telephone interview system using random-digit dialing. For landline telephone surveys, data are collected from an adult randomly selected in a household. For cell phone surveys, an adult answering the cell phone who lives in private residence or college housing is surveyed. Data collected are then sent to CDC for editing, processing, weighting, and analysis. Response rates from landline and cell phones are calculated and combined for each state. 9
Study population and outcome
A total of 2,752,686 adults were pooled across the years. Responses with missing values on medical cost, health insurance coverage, and demographic and socioeconomic covariates were excluded. The study had a final sample size of 2,249,749.
The outcome of interest in our study was adequate health coverage. This was defined as the presence of health insurance coverage with no medical cost barriers to accessing health care. This variable was derived from the following questions: “Do you have any kind of health care coverage, including health insurance, prepaid plans such as HMOs, or government plans such as Medicare, or Indian Health Service?” and “Was there a time in the past 12 months when you needed to see a doctor but could not because of cost?” Both had binary responses: “Yes” or “No.” The outcome had 4 groups: persons with health care coverage WITHOUT medical cost barriers; persons with health care coverage WITH medical cost barriers; persons with NO health care coverage WITH medical cost barriers; and finally, persons WITH NEITHER health care coverage NOR medical cost barrier.
Main predictor and covariates
Sex assigned at birth (with the binary option of male vs. female) was the main predictor variable. Demographic and socioeconomic covariates included in the analysis were age, race/ethnicity, educational level, employment status, and annual household income.
Race/ethnicity was grouped into White (non-Hispanic), Black (non-Hispanic), Asian (non-Hispanic), American Indian/Alaskan Native/Native Hawaiian or other Pacific Islander (non-Hispanic), Multiracial/Other race (non-Hispanic) and Hispanics. Education level was indicated by “did not graduate high school,” “high school graduate,” “attended college or tech school,” and “graduated college or tech school.” Employment status had the following categories: “employed for wages,” “self-employed,” “out of work for less than one year,” “out of work for one year or more,” “homemaker,” “student,” “retired,” and “unable to work.” Age (in years) was categorized as 18–24, 25–34, 35–44, 45–54, 55–64, and ≥65. Annual household income was indicated by the following tiers: “under $10,000,” “$10,000 to under $15,000,” “$15,000 to under $20,000,” “$20,000 to under $25,000,” “$25,000 to under $35,000,” “$35,000 to under $50,000,” “$50,000 to under $75,000,” and “$75,000 and over.”
Statistical methods
All data were analyzed using SAS version 9.4 (SAS Institute, Cary, NC).
Descriptive statistics
Differences in unweighted frequencies and proportions of the sex assigned at birth variable, demographic and socioeconomic covariates by the outcome variable were estimated using the chi-square test.
Regression analysis
The BRFSS complex sampling design was adjusted for using the SAS SURVEY procedure and weighting methodology. Domain statement was used to exclude missing values from the analysis. Unadjusted and adjusted (age, household income, race/ethnicity, and employment status) logistic regression models were used to assess the odds for adequate health coverage among females when compared with males over the 6-year study period. Using the unadjusted and adjusted odds ratio (OR) (age, household income, and employment status), we also evaluated the likelihood of adequate coverage between females and males of the same racial/ethnic groups. We also checked for interaction between sex and race/ethnicity as well as for collinearity. This analysis was determined to not be human subjects research by the local Institutional Review Board (IRB).
Results
Descriptive statistics
The analysis of the 6-year data showed that the study sample (N = 2,249,749) was made up of 55.8% females (N = 1,256,243), with 32.6% (N = 733,216) aged ≥65 years, and 77.6% identifying as White non-Hispanics (N = 1,745,209). The study revealed that 38% (N = 856,994) had graduated college or tech school, 43.7% (N = 983,034) were employed for wages, 8.9% (N = 199,022) were self-employed, and 28.3% (N = 636,739) were retired. Over half (52.9%, n = 1,186,114) indicated having an annual household income of <$50,000.
Among those included in the sample (N = 2,249,749), results showed that 84.4% (N = 1,898,097) had adequate health coverage (health insurance with no out-of-pocket cost barrier to health care) (Table 1). Of those with inadequate coverage, 7.4% (167,321) had out-of-pocket medical costs that served as a barrier to care despite having health insurance; 4.8% (N = 108,371) had neither health insurance nor out-of-pocket medical costs; and 3.4% (N = 75,960) were without health insurance and did have out-of-pocket medical costs that served as a barrier to care. Of the 1,898,097 persons with adequate health coverage, 55.8% (N = 1,059,325) were females, 80.2% (1,523,121) were White, non-Hispanics, 41% (N = 780,404) were college graduates or graduates of a tech school, 43.7% (N = 829,905) were employed for wages, 8.2% (N = 155,272) were self-employed, and 31.6% (N = 599,621) were retired, while 52% (N = 978,597) earned a household income of ≥$50,000.
Unweighted Demographics and Year of Survey by Health Care Coverage and Out-of-Pocket Cost Barrier, Behavioral Risk Factor Surveillance System, 2013–2018
This is a complete case analysis. We excluded all missing observations from this table.
Among persons with both health coverage and out-of-pocket costs that served as a barrier to accessing medical care (N = 167,321), women made up 63.4% (N = 106,085) of this sample. They also made up 57.1% (N = 43,388) of the number of persons with out-of-pocket cost barrier and no health coverage, and 43.8% (47,445) of persons with neither health coverage nor medical cost barrier to health care access.
Logistic regression
After adjusting for age, income, race/ethnicity, employment, and education, females were more likely to have out-of-pocket costs that served as a barrier to care despite having health insurance than their male counterparts across the 6-year period (adjusted ORs with 95% Cl from 2013 to 2018 were 1.36 [1.29–1.43], 1.38 [1.32–1.46], 1.31 [1.24–1.38], 1.33 [1.26–1.40], and 1.32 [1.25–1.40], respectively; see Table 2 and Fig. 1). Females were less likely to have inadequate coverage with neither health coverage nor medical cost barrier to health care (adjusted ORs with 95% Cl from 2013 to 2018 were 0.56 [0.52–0.59], 0.60 [0.56–0.64], 0.58 [0.54–0.62], 0.58 [0.54–0.63], 0.58 [0.54–0.63], and 0.63 [0.58–0.68], respectively) [Table 2].
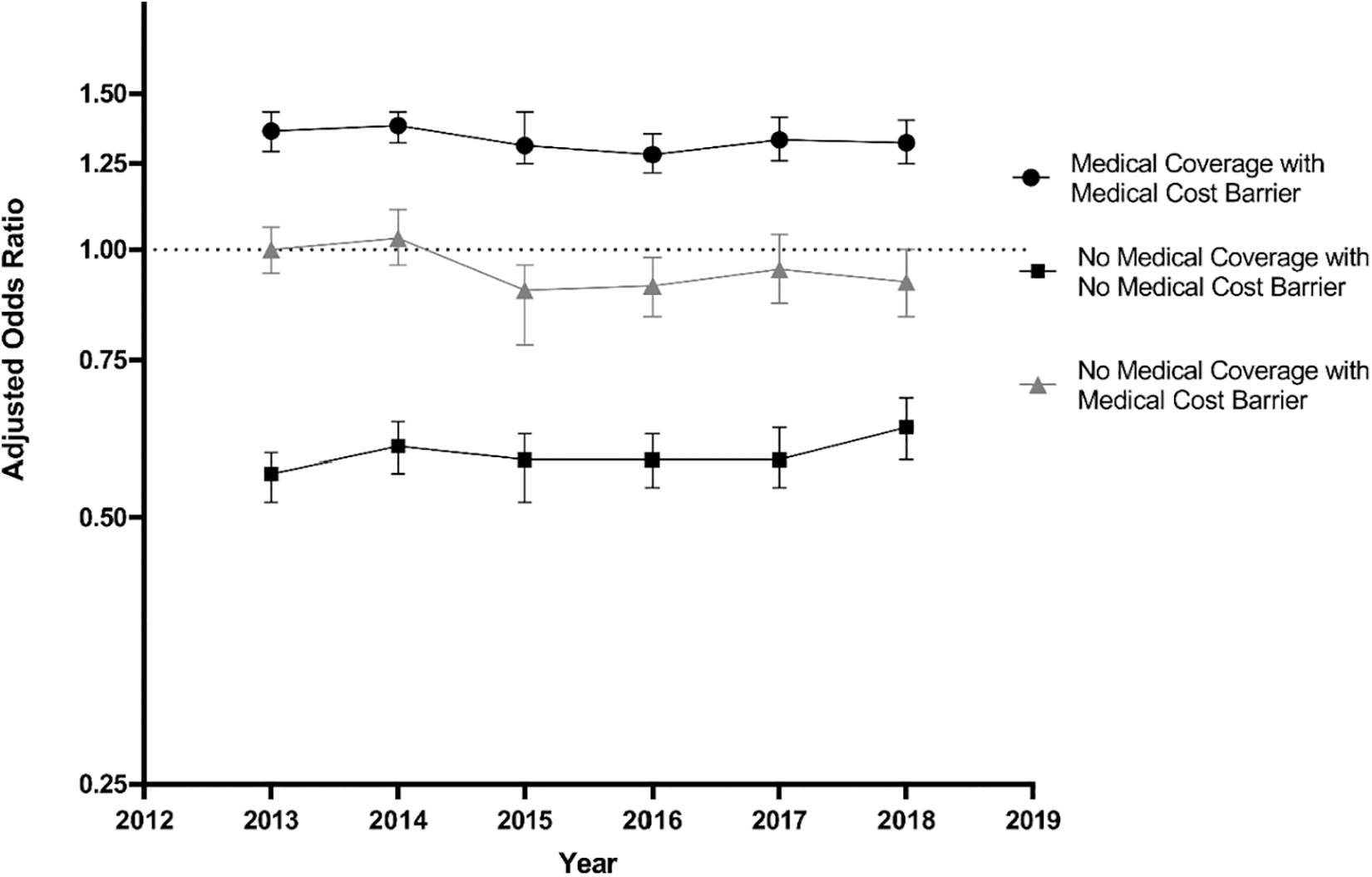
Trends in health coverage and cost that served as barriers to health care in females versus males. Odds ratios were adjusted for age, income, education, and employment status. Reference is Medical Coverage with No Medical Cost Barrier.
Unadjusted and Adjusted Odds of Health Coverage and Health Cost Barrier in Females Compared with Males, Behavioral Risk Factor Surveillance System, 2013–2018
Odds ratios were adjusted for age, income, race, employment status, and education.
aOR, adjusted odds ratio; CI, confidence interval; uOR, unadjusted odds ratio.
When compared with males of the same race/ethnicity, females were more likely to have health coverage but with the out-of-pocket cost barriers across the 6-year period. On adjustment, the relationship persisted for White (non-Hispanic) females across the 6 years. The relationship varied for other races, from females being more likely than males, to no difference between the sexes (Fig. 2). White non-Hispanic, Black non-Hispanic and Hispanic females, when compared with their respective male counterparts, were less likely to have out-of-pocket cost barriers with no health coverage, and this relationship persisted on adjustment (adjusted for age, income, race, employment status, and education).
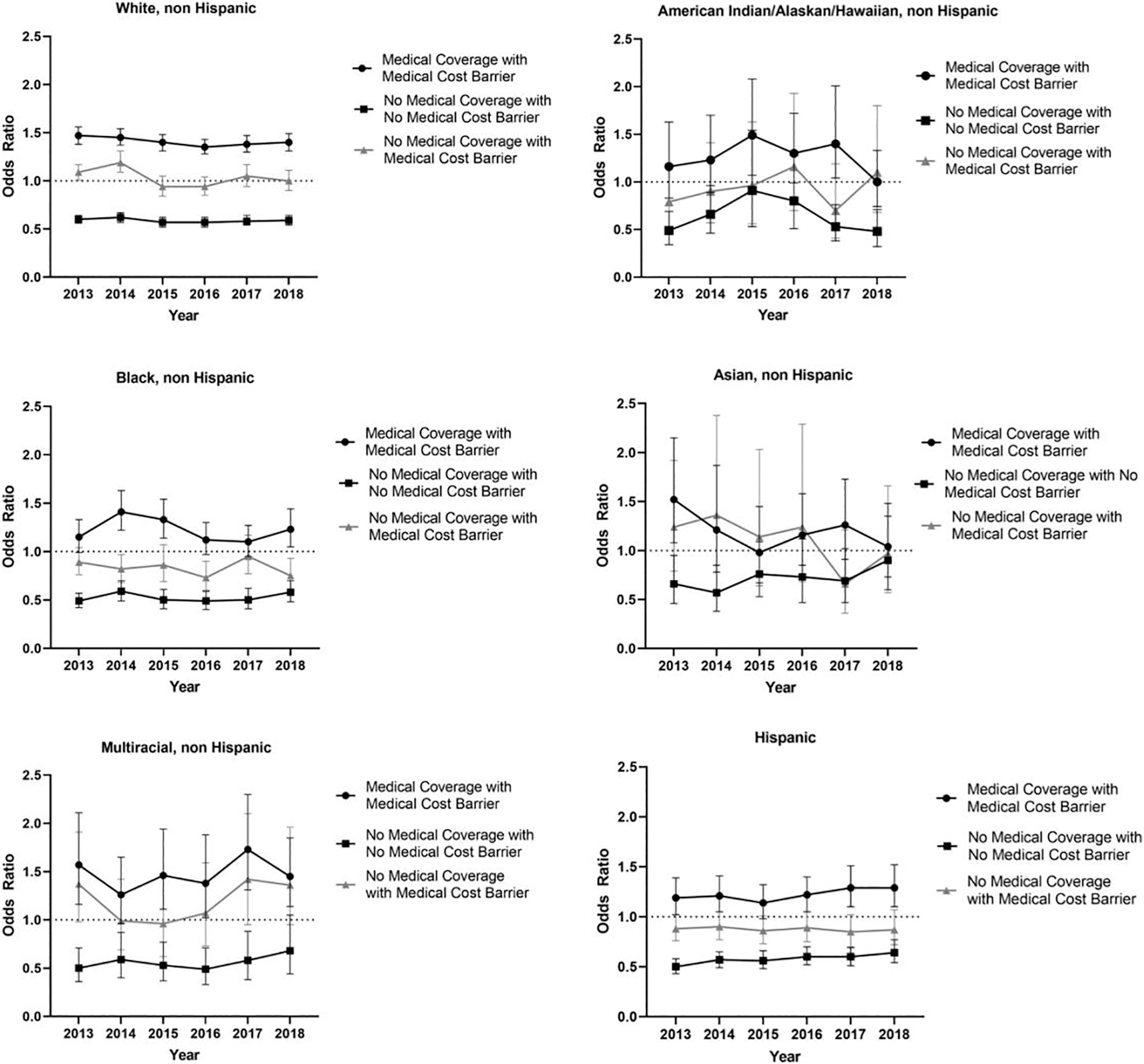
Trends in health coverage and cost barriers in females versus males of the same race. Odds ratios represent females versus males, and were adjusted for age, income, education, and employment status.
Interaction between sex and race/ethnicity
An interaction was found between race and sex. White males were less likely than males and females of other races/ethnicity to have inadequate health coverage of any kind. White females were more likely than White males to have health coverage with medical cost barrier but less likely to have no health coverage with no medical cost barrier to health care (Fig. 2).
Discussion
Despite overall increased health care coverage and a decrease in out-of-pocket costs, The Commonwealth Fund reported in 2016 that ∼11% of individuals incurred health care expenses exceeding 10% of their income. 10 In this analysis, we provide an overview of self-reported health care coverage and cost barriers in the United States for female versus men. Our results suggest that females more than males continue to have increased odds of out-of-pocket costs that served as a barrier to care despite having medical coverage. This relationship appears to be largely unchanged from 2013 through 2018. When examining if these relationships differ by race/ethnicity, the same relationship does not persist for Asians across sex. This suggests that health coverage and cost barriers are similar among Asian males and females.
Our results suggest that although more women are insured, the coverage may be inadequate compared with their male counterparts. Women often have greater preventive and health care needs, such as contraceptive services, early cancer screenings, and maternity care. Although many of these preventive health visits are fully covered under the ACA, the prescriptions and testing generated from these appointments often involve a patient copay resulting in a greater financial burden on women. A study by Hoagland and Shafer evaluated out-of-pocket costs from individuals with employment-sponsored insurance in 2018. They found that women's services were one of the leading causes of out-of-pocket cost. 11 Moreover, they found that there was one of four chances that a patient would receive a bill for a preventative care service that should have been fully covered. 11
Daher et al. also utilized the BRFSS to evaluate gender disparities in accessing health care and nonmedication adherence due to cost barriers. Similar to our findings, women were more likely to report delays in accessing health care and report cost barriers to seeing a provider and adhering to medication use.
12
Several studies have found that high out-of-pocket prescription costs have been shown to lead to nonmedication adherence and worse clinical outcomes.13
Policies that include greater coverage of preventative services and reduce cost shares may assist with reducing out-of-pocket cost barriers for females. 1 Evaluation of health care policies for women is critical as a recent analysis has found a trend in worsening life expectancy and material mortality. 2 Other considerations for future research include a more in-depth evaluation of societal factors influencing cost barriers.
As with any analysis of the BRFSS, this analysis has limitations including noncoverage bias, since adults residing in households without a telephone are excluded, and these tend to be people of lower socioeconomic status. Moreover, the binary definition of “out-of-pocket costs that served as a barrier to care” may overestimate the difference in the underinsured as some respondents may have very real but small out-of-pocket costs. Other analyses have used a percentage of income spent on health care, which standardizes cost differences more effectively.
We were only able to determine if there was a cost that served as a barrier to care. Another limitation is self-report bias could occur as people tend to report a healthier lifestyle. In addition, we are unable to examine the types of health care women may be receiving with additional costs compared with their male counterparts, and therefore cannot make recommendations on where improvements in health care coverage should take place.
Conclusion
Although there has been a decline in the number of uninsured females since 2010, females are unfortunately more likely to have inadequate coverage with out-of-pocket costs that serve as a barrier to them accessing care. Further research on policies as it relates to cost sharing and out-of-pocket costs may help guide improvements in health insurance coverage.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This research received no funding.