
Abstract
Background:
Hemorrhoids, a gastrointestinal tract disorder, are common during pregnancy. However, large-scale epidemiological studies on hemorrhoids during pregnancy are limited. Therefore, this study used analyzed data from a nationwide population-based database to investigate the prevalence, characteristics, and treatment of hemorrhoids in Taiwan.
Materials and Methods:
This retrospective population-based study used data from the National Health Insurance Research Database and Taiwan Birth Certificate Application to collect the medical records of women who were pregnant at any time during 2009–2018. Hemorrhoids was defined by International Classification of Diseases, 9th Revision, Clinical Modification (ICD-9-CM) (455. X) and International Classification of Diseases, 10th Revision, Clinical Modification (ICD-10-CM) (K64.X, O22.4X) with related treatment.
Results:
We enrolled 1,608,804 deliveries in 1,070,708 women. The proportion of hemorrhoids increased with age in both primipara and multipara women. Of the pregnant women, 31% received oral medication, and 93.2% used the topical ointment to treat their hemorrhoids. Few patients (1.8%) required procedure or surgery during pregnancy, and 41.4% of those patients underwent procedure or surgery in their first trimester. The cumulative incidence of hemorrhoids during pregnancy was significantly higher in women with a history of hemorrhoids and those with multifetal pregnancies. No significant difference in the incidence of hemorrhoids was observed between multiparous and primiparous women.
Conclusion:
Women with a history of hemorrhoids or those carrying multiple fetuses had an increased risk of hemorrhoids during pregnancy. The most commonly used treatment for hemorrhoids during pregnancy was topical ointments, with only a small proportion (1.8%) of patients requiring procedure or surgery.
Introduction
Hemorrhoids, a common medical condition that affects the anorectal area, are often encountered in clinical practice. Although their exact causes remain unknown, hemorrhoids are a normal part of the anatomy of the anorectum because they serve as venous anal cushions that play a crucial role in maintaining continence. 1,2 The prevalence of hemorrhoids in Europe is estimated to be 9%–11%, 3 and a Korean population study reported an incidence of 14%. 4 In the United States, hemorrhoids affect 20%–50% of the population. 5
Hemorrhoids often develop during pregnancy. 6 They are associated with changes in hormones such as progesterone during pregnancy and an increase in circulating blood volume, leading to an increase in intra-abdominal pressure and venous congestion in the perianal area. 7 The main symptoms of hemorrhoids are pain, bleeding, prolapse, itching, and burning. Pregnant women may experience acute thrombosed hemorrhoids, which can cause severe pain. 8
Treatment options for hemorrhoids include dietary changes, such as increasing fiber intake, lifestyle changes, medications, and surgery. Conservative treatments are preferred for pregnant women to manage hemorrhoids, with the goal of controlling pain and relieving symptoms. 9 When conservative treatment is ineffective, minimally invasive procedures, such as rubber band ligation, sclerotherapy, and infrared photocoagulation, can be alternative treatment options. 8 Some studies have revealed that surgery can relieve discomfort during pregnancy, particularly in cases of severe pain caused by thrombosed hemorrhoids. 10 In addition, 19.6% of pregnant women with thrombosed hemorrhoids undergo office-based excisional treatment. 11
Few large-scale epidemiological studies have investigated hemorrhoids occurring during pregnancy. This study used data from a nationwide population-based database to investigate the prevalence and characteristics of hemorrhoids in pregnant women in Taiwan and proposed treatment options for this condition during pregnancy. We determined an optimal treatment plan for hemorrhoids by using insurance claims data. All patients in our study experienced symptoms and received treatment.
Materials and Methods
Sources of study data
Taiwan's single-payer National Health Insurance (NHI) program, which was established on March 1, 1995, provides comprehensive health insurance coverage to nearly 100% of Taiwan's citizens. 12 The NHI Research Database (NHIRD) is a valuable resource for evaluating the health status of patients in Taiwan and contains information on demographics, such as age and sex, surgical procedures, medical expenditures, and prescription details for inpatient and outpatient care. Disease diagnoses are coded in accordance with the International Classification of Diseases, 9th Revision, Clinical Modification (ICD-9-CM) and the International Classification of Diseases, 10th Revision, Clinical Modification (ICD-10-CM).
According to Taiwan's Child Welfare Law, medical facilities are obligated to maintain records of birth certificates and related information and to submit the records to the household registration and health authorities within 7 days of a child's birth. This law was established in 2004 and includes information on maternal background, pregnancy status, newborn data, and spouse information. This study used data from Birth Certificate Application (BCA) forms, which record live births and stillbirths with a gestational age of ≥20 weeks or a birth weight of ≥500 g, and data from the NHIRD to investigate the epidemiology and treatment of hemorrhoids in pregnant women in Taiwan. Because both databases are deidentified, the requirement for written informed consent was waived. The Institutional Review Board of Chang Gung Memorial Hospital approved this study (approval no. 202200735B0).
Study cohort
This study collected data from BCAs on women who experienced pregnancy and childbirth in Taiwan between January 1, 2009, and December 31, 2018. This study enrolled patients who were diagnosed as having hemorrhoids during pregnancy and received treatment such as oral medication, topical ointment, a procedure, or surgery on the basis of medical records. We excluded those with birth records from 2001 to 2008 to ensure that the first recorded birth in the study period was considered primiparous. Women with missing information were also excluded (Fig. 1). Hemorrhoids have the ICD-9-CM code 455.X 13 and ICD-10-CM codes K64.X and O22.4X.
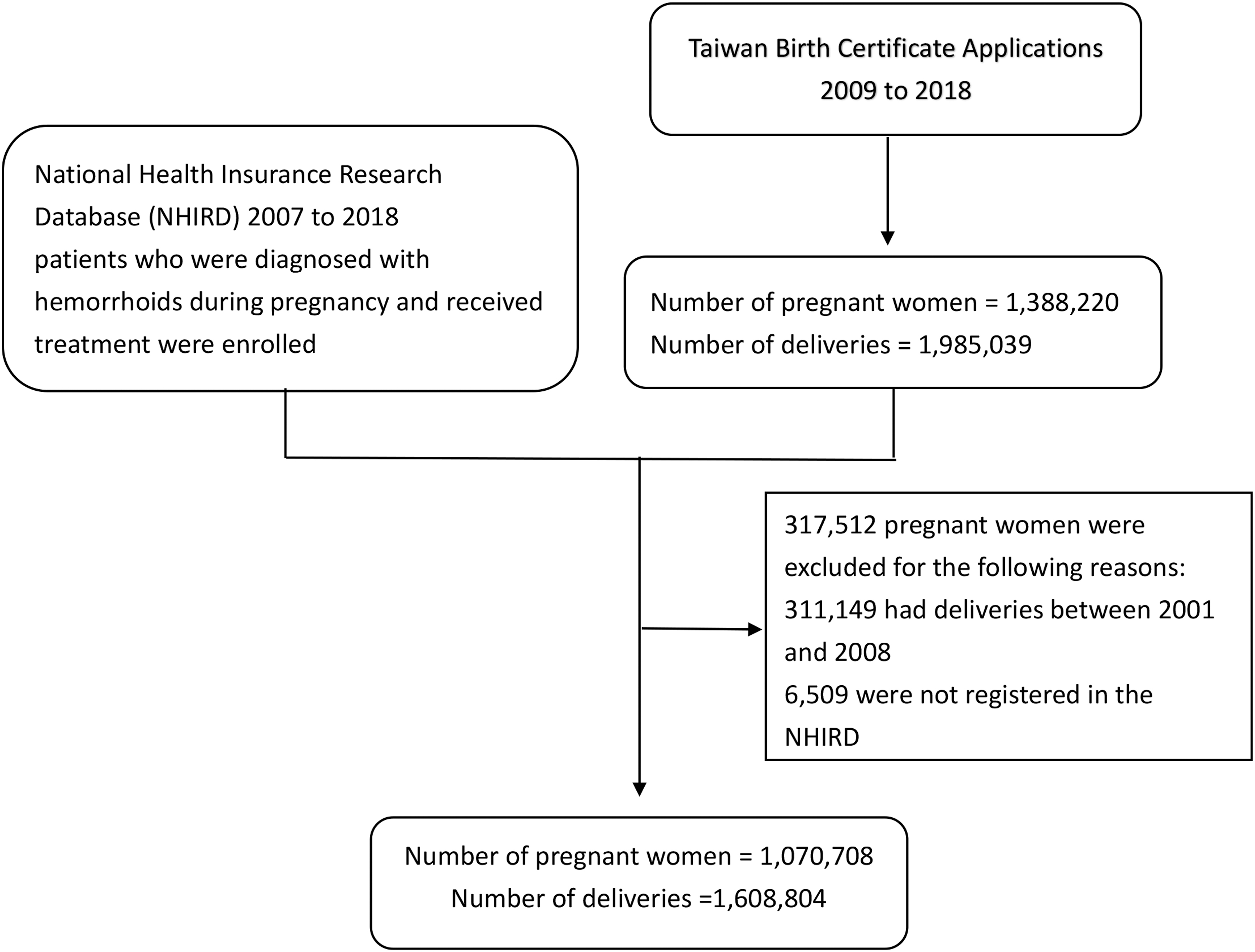
Flowchart of patient selection.
Study variables
We examined various background factors that may contribute to the development of hemorrhoids in pregnant women. These factors include the mother's age at delivery; whether the birth is single or multiple; and a history of constipation, hemorrhoids, or other disorders during pregnancy. Constipation (ICD-9-CM: 564.0; ICD-10-CM: K59.0X) was diagnosed on the basis of three outpatient visits or one hospitalization within 1 year. A history of hemorrhoids (ICD-9-CM: 455.X; ICD-10-CM: K64.X, O22.4, or O87) was determined on the basis of relevant treatment or hospitalization within 2 years before delivery.
This study classified the treatment of hemorrhoids into four categories: oral medication, topical therapy, clinical procedures (e.g., prolapsed hemorrhoid injection, cryotherapy, sclerotherapy, and ligation), and surgery (e.g., simple thrombectomy, total external hemorrhoidectomy, partial hemorrhoidectomy, combined internal and external hemorrhoidectomy, fistulectomy with partial hemorrhoidectomy, and external thrombectomy). 13 We also included comorbidities in the analysis, namely, gestational diabetes (ICD-9-CM: 648.0, 648.8; ICD-10-CM: O24, O99.81), pregnancy-induced hypertension (ICD-9-CM: 642.3–642.9; ICD-10-CM: O11.1–11.3, O13–16), chronic hypertension (ICD-9-CM: 401–405, 642.0–642.2; ICD-10-CM: O10, I10–13, I15, N26.2), pre-eclampsia (ICD-9-CM: 642.4–642.54; ICD-10-CM: O14–P14.13), and eclampsia (ICD-9-CM: 642.6–642.64; ICD-10-CM: O15–O15.9).
Statistical analysis
This study employed Pearson's chi-squared test for categorical variables and t-tests for continuous variables. We evaluated the cumulative incidences for women with and without a history of hemorrhoids, with singleton versus multifetal pregnancy, and with primipara versus multipara status by using the Kaplan–Meier method. Statistical significance was indicated by p < 0.05. All statistical analyses were performed using SAS version 9.4 (Cary, NC, USA).
Results
This study enrolled a total of 1,388,220 women with 1,985,039 deliveries between 2009 and 2018 from BCAs. We later excluded 659 women who were not enrolled in the NHI program and 311,149 women who gave birth between 2001 and 2008. The study evaluated a total of 1,070,708 women with 1,608,804 deliveries (Fig. 1).
Table 1 lists the demographic characteristics of the primiparous and multiparous groups with or without hemorrhoids in each pregnancy. In both groups, the incidence of hemorrhoids was <3% in women aged <20 years, and the incidence increased with age. The proportion of pregnant women with hemorrhoids did not differ substantially between those with single or multiple gestations (5.3% vs. 5.2%; 5.2% vs. 4.6%, respectively). However, women with a history of hemorrhoids or constipation had a significantly higher risk of hemorrhoids during pregnancy, with 10.3% and 25.7% developing hemorrhoids during pregnancy, respectively. In terms of comorbidities during pregnancy, women with gestational diabetes had a higher risk (16.1% vs. 15.0%) of hemorrhoids than did women without gestational diabetes. Hypertension, epilepsy, and pre-eclampsia during pregnancy were not associated with an increased risk of hemorrhoids.
Background Characteristics of Primiparous and Multiparous Women With or Without Hemorrhoids During Pregnancy
Table 2 presents the distribution of treatments for pregnant women with hemorrhoids. As presented in Table 2, 31% of the patients received oral medication, 93.2% used topical ointment, and a minority received invasive interventions (procedures: 762 of 84,188 [0.9%]; surgery: 756 of 84,188 [0.9%]). Among the patients, 82% were first diagnosed and treated during pregnancy by obstetrician–gynecologists. Most patients did not visit a proctologist (90.7%).
Treatments for Pregnant Women with Hemorrhoids During Pregnancy
Hemorrhoid prolapse injection, cryotherapy, sclerosis, and internal hemorrhoidal ligation.
Thrombectomy, hemorrhoidectomy (external, internal), and hemorrhoidectomy (partial, internal, and external).
Department in which patient first received diagnosis and was treated during pregnancy.
CRS, colorectal surgery; GCS, general surgery; OBS, obstetrics and gynecology.
Table 3 presents the percentage of individuals who underwent procedures and surgery for hemorrhoids, which increased with age. A higher proportion (35.8%) of the women with a history of hemorrhoids before pregnancy underwent procedures or surgery for hemorrhoids during pregnancy. Of those who underwent surgery, 41.4% underwent surgery in the first trimester; however, most patients (52.7%) received oral medication or topical ointment in the third trimester. In the invasive intervention group, 37.5% of the patients received medical care only once; in the oral medication and topical ointment group, 80.4% received medical care only once.
Distribution of Women Who Received Medical Care or Invasive Intervention for Hemorrhoids During Pregnancy
May have received treatment before surgery during pregnancy.
The results of the Kaplan–Meier analysis revealed a significantly higher cumulative incidence of hemorrhoids in women who had a history of hemorrhoids (p < 0.001; Fig. 2) and in those with a multifetal pregnancy (p < 0.001; Fig. 3) than in their counterparts. However, the results indicate no significant difference in the cumulative incidence of hemorrhoids between multiparous and primiparous women (p = 0.151; Fig. 4).

Cumulative incidence of hemorrhoids for women with and without a history of hemorrhoids during pregnancy.
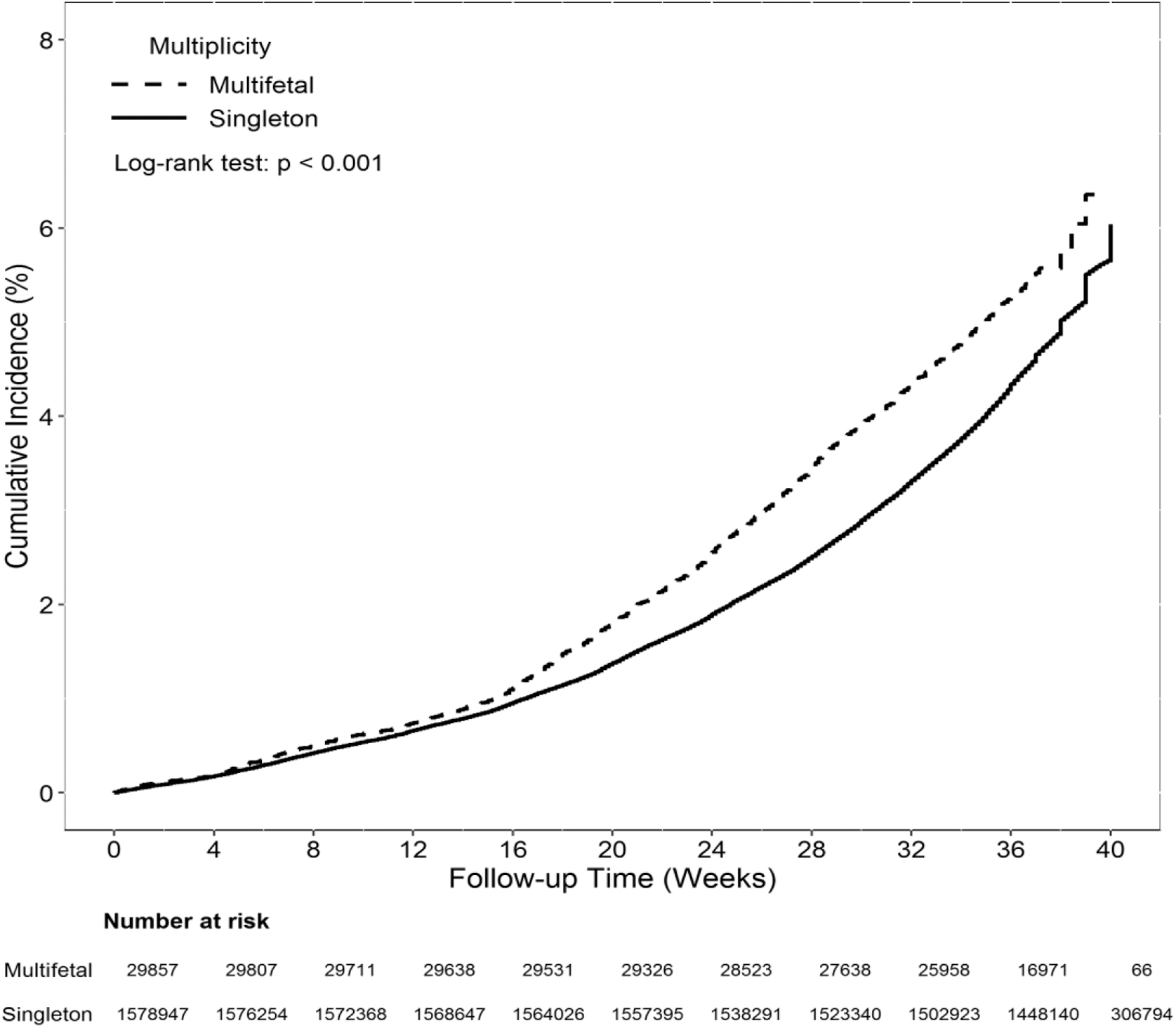
Cumulative incidence of hemorrhoids during pregnancy for women with multifetal and singleton pregnancies.
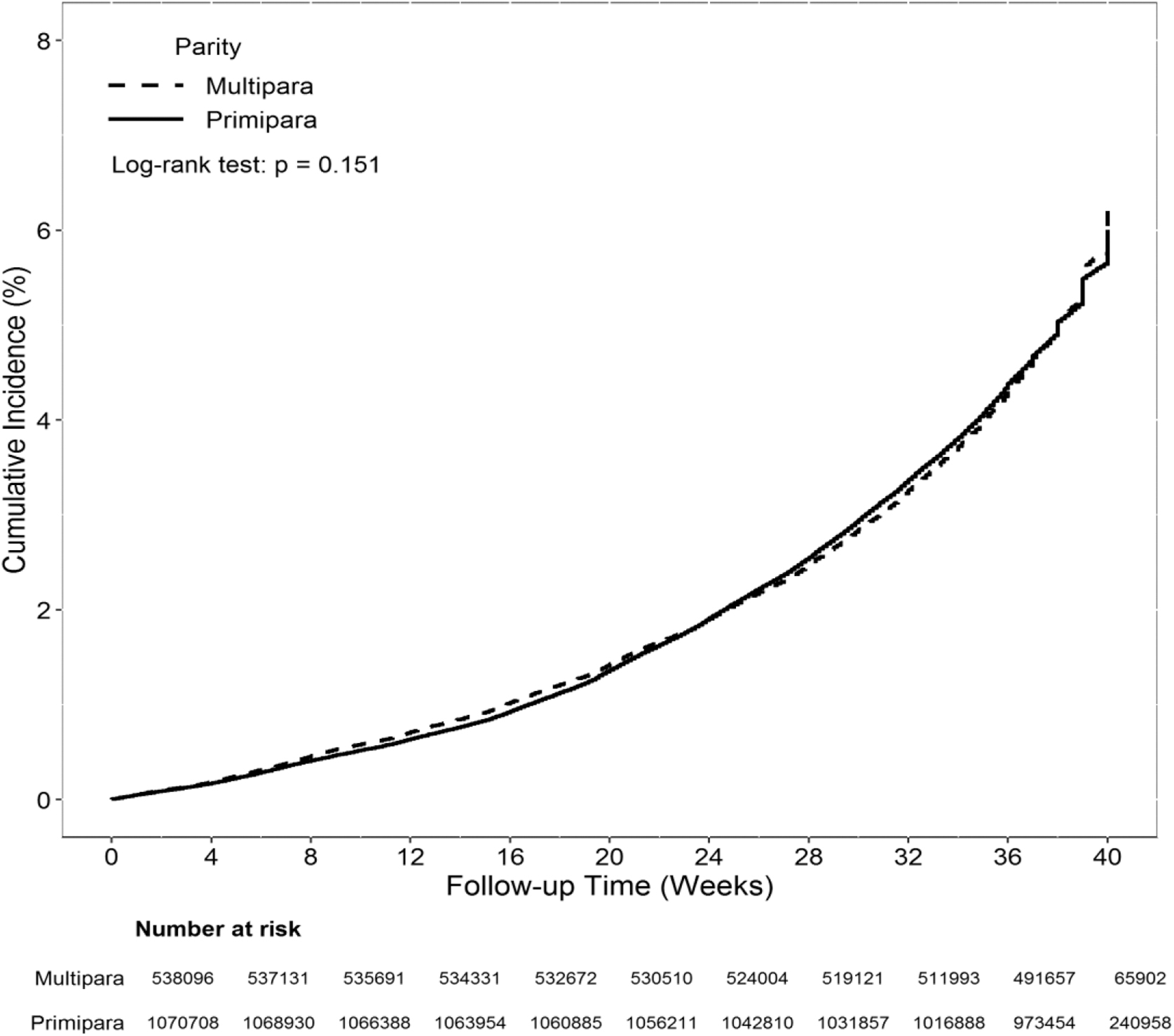
Cumulative incidence of hemorrhoids for primiparous and multiparous women during pregnancy.
Discussion
According to our review of the literature, this study is the first large-scale nationwide study of the management and treatment of symptomatic hemorrhoids during pregnancy in an Asian country. Our study divided pregnant women into primiparous and multiparous groups to compare the proportion of women who developed hemorrhoids. Although our findings indicate no significant difference between the groups, the incidence of hemorrhoids was associated with age, which is consistent with the findings of other studies. 3,14,15 However, a study by Gojnic et al. 16 suggested that multiparous women in Serbia and Montenegro have a higher incidence of hemorrhoids than primiparous women.
The multivariate analysis revealed that women with a history of hemorrhoids and those with multiple gestations were significantly more likely to develop hemorrhoids during pregnancy (both ps < 0.001). Studies have revealed that a history of anorectal disorders is a risk factor for hemorrhoids. 10,14 However, few studies have investigated the effect of fetal number on the incidence of hemorrhoids. The increase in the incidence of hemorrhoids in women carrying multiple fetuses can be explained by several factors, such as the steady growth of the fetus and the gradual increase in amniotic fluid in the second trimester, which lead to heavier intra-abdominal pressure, maternal weight, and total fetal weight. 17
According to a study conducted in the United States, the rate of premature delivery before 34 weeks is higher in triplet pregnancies, with two-thirds of deliveries reported to be premature, compared with one-fifth of twin pregnancies and 2% of singleton pregnancies. 18 Thus, women with multiple gestations may benefit from controlling their body weight and discussing the possibility of early delivery; this approach has been reported to have similar cumulative incidence rates to full-term pregnancy after 36 weeks.
The results of our study indicate that physicians generally prefer to administer conservative treatments to pregnant women with hemorrhoids, such as topical ointment, rather than oral medication. Conservative treatment is a common approach for pregnant women with hemorrhoids, unless their conditions are severe. However, some experts have suggested that surgery may be necessary to alleviate severe discomfort during pregnancy. 10 Conservative treatments are most commonly prescribed for pregnant women with hemorrhoids and typically involve increasing fluid and fiber intake and taking sitz baths.
Effective conservative treatments include flavonoid supplements, topical preparations, anti-inflammatory agents, and local steroids. However, oral medications are more commonly prescribed for the general population than topical treatments (100% vs. 83.5%). 19 According to Vazquez, 20 supplementation with rutoside, a common treatment for hemorrhoids, is not recommended during the first trimester of pregnancy. Pregnant women and their physicians are generally cautious about oral medications because of concerns for the health of the fetus. For this reason, physicians generally prefer to prescribe topical ointment for hemorrhoids during pregnancy.
Our results reveal that a small percentage of the women underwent surgery during pregnancy to treat hemorrhoids. Conditions that necessitated surgery include ineffective conservative treatments for grade III or IV hemorrhoids with severe symptoms, the presence of other anal diseases, and thrombosed hemorrhoids. 21,22 Only 0.9% (n = 756) of the women in this study underwent surgery, whereas Saleeby et al. observed that only 0.2% (n = 25) of patients underwent surgery. 10 Most of these patients required medical assistance in their first trimester and may have required additional medical care throughout their pregnancy.
The treatment of hemorrhoids is generally based on the degree and the severity of hemorrhoids. 2 Acute crises, such as perianal thrombosis and thrombosed hemorrhoids, are common and may occur in pregnant women with pre-existing hemorrhoids. 9 These conditions are characterized by sudden and severe pain and require immediate medical attention. 8 Therefore, pregnant women with hemorrhoids may require invasive intervention if their symptoms cannot be effectively managed with oral or topical medications.
In this study, 5.3% of primiparous women and 5.2% of multiparous women developed hemorrhoids during pregnancy. Although hemorrhoids are common, the exact incidence of this condition in pregnant women remains unclear. 20 According to Hong et al., 17% of pregnant women in Korea develop hemorrhoids. 15 A study conducted in Italy revealed that 25%–35% of pregnant women have symptomatic hemorrhoids during the third trimester and the first month after delivery. 23 The prevalence of hemorrhoids during pregnancy has varied considerably between studies. Gojnic et al. observed an 85% prevalence of hemorrhoids during second and third pregnancies. 16
The causes of this inconsistency in the results are unclear; however, it may be explained by the small sample sizes in some studies that used questionnaires or phone interviews. 15,24,25 The self-diagnosis of perianal diseases is highly inaccurate. 26 In addition, some patients may provide socially acceptable answers to private questions, such as those related to the digital evacuation of stool or fecal incontinence, which could result in potential under-reporting of symptoms. 25 This study overcame this limitation because we employed a broad national sample of pregnant women whose diagnoses and treatments were provided by physicians, ensuring a high degree of accuracy.
Limitation
This study has several limitations. First, hemorrhoids are a self-limiting disease, and some women may not seek medical attention for mild symptoms and instead rely on self-treatment or over-the-counter medications, which are not covered by the NHI plan. Patients with hemorrhoids may not discuss the condition with their health care provider because of embarrassment or out of a desire for privacy. In addition, our study only enrolled patients with information regarding the treatment type received in their medical records. These factors all contribute to the low incidence in our study.
Second, some treatments for hemorrhoids are not covered by insurance in Taiwan and must be purchased out of pocket, such as diosmin, Doppler-guided hemorrhoidal artery ligation, transanal hemorrhoidal dearterialization, and stapler hemorrhoidopexy. Pregnant women may opt for these treatments because of their perceived benefits, such as lower levels of pain and shorter recovery times. However, information on out-of-pocket treatments was unavailable because the data were obtained from the NHIRD.
Third, certain risk factors for hemorrhoids may increase the risk of developing hemorrhoids, such as low-fiber diets, frequent straining, prolonged standing or squatting, and high body mass index. 1,27 However, the NHIRD does not provide information on these risk factors.
Conclusion
This study revealed that the incidence of hemorrhoids during pregnancy was higher in women with multifetal pregnancies and in those with a history of hemorrhoids. The effect of parity on the incidence of hemorrhoids during pregnancy was nonsignificant. Topical ointment was the most common conservative treatment to manage hemorrhoids during pregnancy, with invasive interventions required for a minority of patients.
Footnotes
Acknowledgment
We thank Health Information and Epidemiology Laboratory of Chang Gung Memorial Hospital, Chiayi Branch, for the comments and assistance in data analysis.
Authors' Contributions
Y.-Y.C. conceived the study idea. C.-Y.C., C.-H.L., L.-Y.C., W.-T.S., and Y.-Y.C. developed the analysis plan and coding framework. K.-J.C., W.-T.S., and Y.-H.Y. conducted data extraction and analysis on the eligible articles, and K.-J.C. and Y.-H.Y. validated the framework. Y.-Y.C. wrote the initial draft. C.-H.L., W.-T.S., L.-Y.C., and Y.-H.Y. reviewed and edited the article. All authors contributed to article revisions, read, and approved the final version. All authors have read and agreed to the published version of the article.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This study was supported by a grant from Chang Gung Memorial Hospital (approval no. 202209276306).