
Abstract
Objective:
Primary high risk human papilloma virus (hrHPV) testing is recommended as first-line screening for cervical cancer. Testing involves either a clinician-collected or a self-collected cervicovaginal swab. This study examines concordance between methods of collection of primary HPV testing.
Methods:
Ovid MEDLINE, Ovid Embase, and Cochrane were searched for relevant studies on self-collected and clinician-collected primary HPV testing published before December 31, 2022. English-language studies for primary HPV testing of average-risk patients were included. Studies conducted in screening settings rather than colposcopy clinics, that used standard devices for HPV collection, and that directly compared methods of collection were included. Outcomes were concordance and kappa between paired samples, and rate of HPV detection in self-collected and clinician-collected samples.
Results:
A total of 2381 studies were screened, of which 228 were included for full-text evaluation. Thirty-six studies, including 23,328 individuals screened, met the inclusion criteria. The rate of HPV detection ranged from 4.7% to 63% for self-collection and from 3.7% to 62% for clinician-collection. The concordance ranged from 78.2% to 96.9%, and kappa had substantial agreement for 26 of the 36 studies and moderate agreement for 7 of the 36 studies.
Conclusions:
This study directly compares clinician-collected and self-collected primary HPV screening rates. Studies were conducted in methods which are widely reproducible in the primary care setting. Primary HPV self-collection is a reliable and accurate method for cervical cancer screening.
Introduction
Cervical cancer mortality has decreased from 3.2/100,000 in 1996 to 2.2/100,000 after the initial recommendations for widespread cervical cancer screening over 20 years ago. 1,2 Human papillomavirus (HPV) testing has improved risk stratification, reduced the incidence and mortality from cervical cancer, and altered screening recommendations since first routinely available in early 2010s. 3,4 Cervical cancer screening recommendations were most recently updated by the United States Preventive Services Taskforce (USPSTF) in 2018. 1 Screening options included the following: cytology alone for women aged 21–29 years every 3 years and screening by either HPV alone every 5 years, screening with HPV and cytology every 5 years, or screening with cytology alone every 3 years for women aged 30–65 years. Primary HPV testing is defined as the use of high-risk HPV testing alone for cervical cancer screening.
Primary HPV testing can be performed by either clinician-collected samples or a self-collected cervicovaginal swab. While the USPSTF recommended primary HPV screening as an option, the group did not specify the direct method of testing in their recommendation. Self-collected samples, so-called “self-sampling,” have many acknowledged advantages compared with clinician-collected samples. Self-sampling is less costly, less invasive for patients, and causes less psychological stress. 5 –7 However, the task force identified a gap in research regarding high risk human papilloma virus (hrHPV) testing—self-sampling had not been robustly evaluated in comparison to clinician-collected samples. 1
In addition to the self-sampling advantages above, it also offers a solution to another gap identified by the USPSTF. Individuals in minority groups, those of low socioeconomic status, and those in communities with low access to health care have lower rates of screening for cervical cancer. 8 Self-sampling may benefit these under-screened groups and promote equitable screening strategies as self-sampling may take place at home via mailed kit, reduce the need for pelvic examinations, and reduce visits to the clinician's office. 9
This systematic review aims to fill the USPSTF-identified gap in the literature and identify the rates of concordance and reliability between paired clinician-collected and self-collected hrHPV samples in average-risk women undergoing cervical cancer screening.
Methods
Prospero ID
This systematic review was reported following the Preferred Reporting Item for Systematic Reviews and Meta-Analyses (PRISMA) statement. The study protocol was registered with the PROSPERO ID CRD42021250098 before data extraction.
Sources
Eligible trials were identified by searches of Ovid MEDLINE, Ovid Embase, and Cochrane up to December 31, 2022, using keywords and controlled vocabulary for the concepts of HPV and cervical cancer screening. The full search strategies for each database are included in Supplementary Appendix SA1.
Eligibility criteria
Studies were included if they met the following criteria: (1) the study was published in the peer-reviewed literature before December 31, 2022; (2) the study design was one of the following: randomized control trial, well-designed controlled clinical trial, cohort study, case–control study; (3) target population was average-risk and asymptomatic people with a cervix between 30 and 65 years old; (4) the modality of HPV self-collection was performed via vaginal/cervical swab; (5) the comparison was clinician-collected HPV testing; (6) the outcomes included rate of HPV detection by self/patient collection, rate of HPV detection by clinician collection, rate of concordance (kappa) between self-collection and clinician-collection; and (7) of robust quality, which we defined as fewer than four high-risk categories on the National Institute of Health (NIH) Quality Assessment Tool for Observational Cohort and Cross-sectional Studies. 10
Studies were excluded if they were conference abstracts, commentaries, or review articles. Studies that were not written in English or able to be translated into English were excluded. Studies were excluded if their study populations included individuals with pre-existing cervical cancer, those with signs of high-grade dysplasia or cervical cancer such as abnormal uterine bleeding, those attending a colposcopy clinic, or individuals with other high-risk features for increased cervical cancer screening as defined by the USPSTF.
Study selection
The titles and abstracts of all retrieved articles were screened for inclusion by the two investigators (A.N.H. and S.B.) independently. Disagreements were resolved by a third reviewer (J.W.C.). Next, the two investigators (A.N.H. and S.B.) performed a full-text review on all articles included after the first round of screening. One investigator thoroughly reviewed the studies and extracted relevant data from the articles (the “full reviewer”). A second investigator reviewed and checked the extracted data (the “checker”). Articles were categorized into seven categories based on the primary exclusion criteria: population, preliminary data such as conference abstracts, outcomes, study design, language, article not available, and duplicate data. Finally, the remaining articles were included in another full-text review for data extraction.
Data abstraction, quality review, and analysis
Data extraction
Data were extracted from the selected articles by two study authors (A.N.H. and S.B.) using a standardized form in Covidence™ software. The following information was extracted from each article: author identification, year of publication, type of study design, country of study location, setting (academic-based or community-based), years study was conducted, and device used by patients or clinician. The inclusion and exclusion criteria of each study were also extracted. Detection rates of HPV positivity for self-collected and clinician-collected swabbing were recorded.
Finally, the concordance and kappa between self-collected and clinician-collected samples were recorded. Data were independently extracted by two investigators (S.B. and A.N.H.). Comparison of the data was reviewed by investigator S.B. Agreements were pushed forward as final data, and disagreements were resolved by discussion and consensus between two investigators (S.B. and A.N.H.). If consensus was not met, a third reviewer resolved the decision (J.W.C.). If there were missing data, this was indicated in the table as “not available.” Final data were exported from Covidence in a Microsoft Excel file.
Quality review
A quality assessment of the 36 studies included in the data extraction review was performed using the NIH Quality Assessment Tool for Observational Cohort and Cross-sectional Studies. 10 This tool consists of 14 criteria to assess various aspects of each study's population, methods, and data analysis. Three of the criteria were removed because they were not applicable to cross-sectional studies according to the NIH guidelines (Question 8 on different levels of exposure of interest, Question 10 on repeated exposure assessment, and Question 13 on follow-up rate). Each criterion was graded with either a “low,” “high,” or “unclear” response to indicate level of potential bias. Two researchers (S.B. and A.N.H.) independently reviewed each study using these guidelines. Disagreements were discussed and resolved by S.B. and A.N.H. Any unresolved disagreements were reviewed and resolved by a third researcher (J.W.C).
Statistical analysis
The primary outcome, the concordance and kappa of the clinician-collected and self-collected samples, is provided as a range of values. The rates of HPV detection by self-collected and clinician-collected swabbing are reported as ranges.
Results
A total of 2381 eligible studies were identified. Of those, 36 articles were included in the final data analysis. The results of the study selection are summarized in a PRISMA diagram (Fig. 1). Overall, there was excellent interrelated reliability in both the primary title and abstract review as well as the full-text review. The proportionate agreement for the decision of inclusion or exclusion of studies in the “Title and Abstract” review was 0.94, with a Cohen's kappa of 0.65. The proportionate agreement for the decision of inclusion or exclusion of studies in the “Full Text” review was 0.97, with a Cohen's kappa of 0.90.
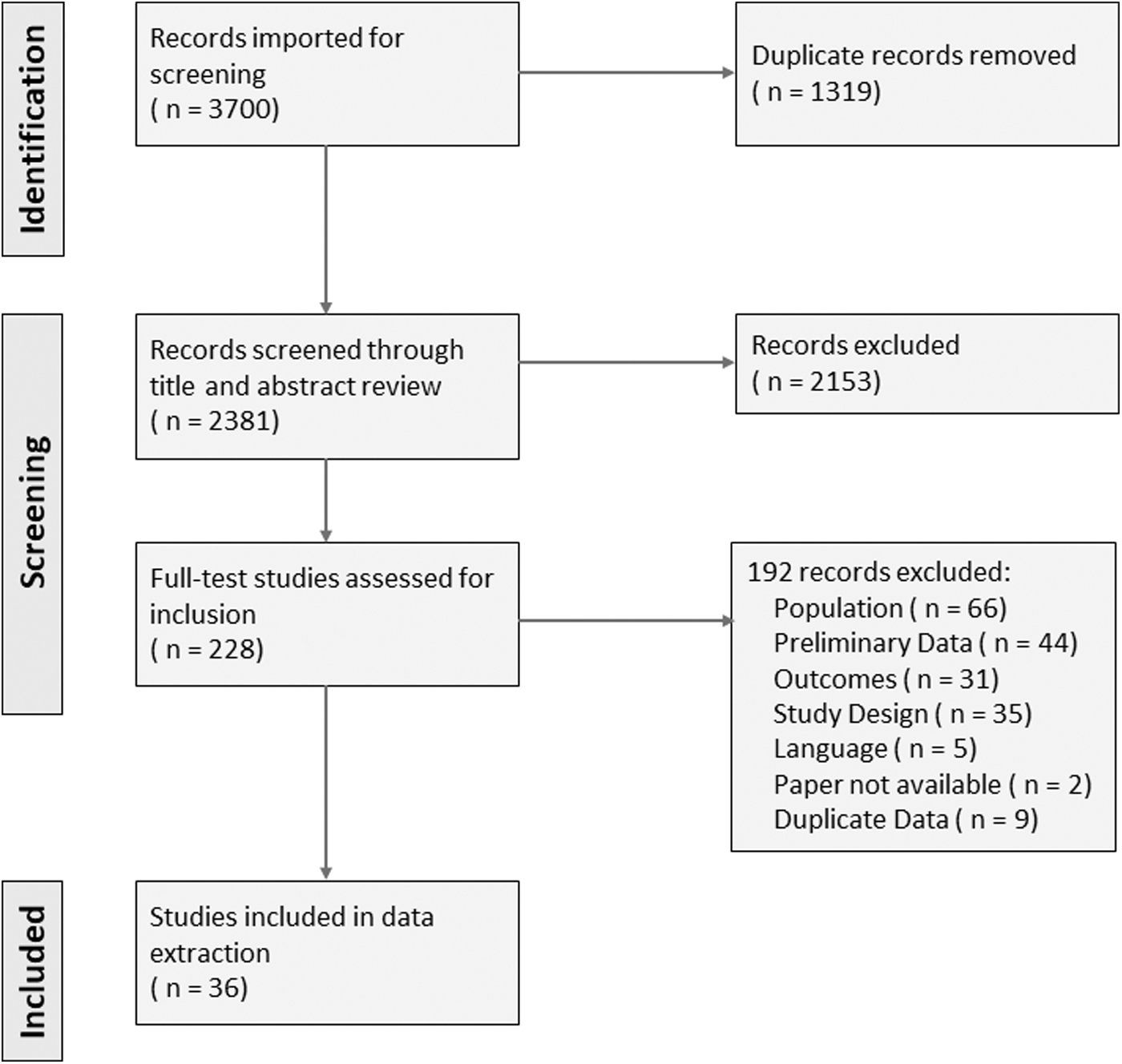
Preferred Reporting Items for Systematic Reviews and Meta-Analyses diagram outlining the inclusionary path of articles available in the peer-reviewed literature (n = number of studies).
Characteristics of the 36 included studies can be found in Table 1. Studies represented 22 countries; 6 studies took place in the United States and 30 were from outside the United States. Twenty-five of the 36 studies took place in a community-based setting, while 8 took place in an academic-based setting, and 2 were combined community-based and academic-based. The age range of participants was 16 to >60 years. Methods and education for self-collection varied between studies, but all used commercially available products such as polyester (Dacron) or rayon tipped swabs, Rovers Vibra Brush®, or similar.
Characteristics of Articles That Met the Inclusion Criteria, Including Author, Title, Years Conducted, Country, Setting, and Type of Device Used by Clinician and Patient
CSCT, Cervical Specimen Collection and Transport; HC2, hybrid capture 2; HPV, human papillomavirus.
Quality analysis
The full quality analysis of all the 36 included studies using the NIH Quality Assessment Tool for Observational Cohort and Cross-sectional Studies is available in Supplementary Table S1.
For each included study, the questions on time frame and exposure were marked as “high” according to guidelines for cross-sectional studies. Cross-sectional studies are conducted where the exposure and outcomes are measured at the same time, thus cross-sectional analyses inherently provide weaker evidence than regular cohort studies regarding a potential causal relationship between exposures and outcomes. For the time frame, since cross-sectional analyses involve the exposures and outcomes being assessed at the same time, they do not allow time to see an effect.
Excluding the exposure and time frame categories, all the studies were robust. Eight studies had a higher risk of bias with three or more categories marked as high risk for bias. The majority of studies had overall low–moderate risk of bias.
Detection rate
The rate of HPV detection in self-collected and clinician-collected samples is reported in Table 2. The rate of HPV detection ranged from 4.7% to 63% in self-collected samples and from 3.7% to 62% in clinician-collected samples. Values varied widely across studies; thus, averages were not calculated; furthermore, the methodology for collection was heterogeneous, making reliability and interpretation of a meta-analysis poor.
Detection Rates, Concordance, and Kappa of Final Included Articles
n, number of studies.
Kappa/concordance
The concordance between self-collected and clinician-collected samples and the kappa for the comparative detection rates are reported in Table 2. The concordance ranged between 78.2% and 96.9% for all the included studies. The kappa values for all the included studies ranged from 0.34 to 0.90. The kappa results between 0.01 and 0.20 are classified as none to slight agreement, 0.21–0.40 as fair, 0.41–0.60 as moderate, 0.61–0.80 as substantial, and 0.81–1.00 as almost perfect agreement. 11 Among the 36 included studies, 2 studies had fair agreement, 7 had moderate agreement, 26 had substantial agreement, and 1 study has almost perfect agreement.
Discussion
This systematic review identifies the validity and accuracy of self- versus clinician-obtained primary HPV testing to fill the knowledge gap presented by the USPSTF. There was high concordance between the self-collected and clinician-collected samples, with ranges between 78.2% and 96.9%; the kappa values varied, but the majority of studies (26/36) had substantial agreement. Primary HPV detection through self-collection is a reliable and accurate screening method for cervical cancer screening.
The studies included in this analysis were conducted with robust protocols, specimens were obtained in an easy-to-understand method, tools are commercially available, and results are reproducible from study to study. Based on these findings, it is plausible and appropriate to use self-collected HPV in U.S. settings. Findings from qualitative research have demonstrated that self-collection is generally accepted and or even preferred by patients for self-collection compared with clinician-collection. 48
Clinician-collected primary HPV testing has been recommended by the USPSTF for nearly 5 years yet has not been routinely used. 49 As such, it is important to consider how self-collection would be implemented into practice. Studies analyzed in this systematic review offered several options for testing: clinic-based self-collection during which a nurse or staff member provided education, home self-collection with swabs and instructions provided by a study team or clinic staff, and home self-collection with mailed swabs and instructions. It is feasible to suggest a similar approach to widespread adoption where multiple testing options are offered, as one single method may not work for all clinics.
The exclusion criteria of this study bring forth points of applicability to the general population. Many available studies reviewed were excluded due to study participant characteristics. Studies were excluded if the majority of participants were not in the USPSTF-defined age group of women 30–65 years old who are appropriate for HPV testing. In addition, studies were excluded if the majority of participants had high-risk characteristics that would not be prevalent in the majority of women in the regular screening population (i.e., HIV-positive women, those with atypical squamous cells of undetermined significance, or seen in a colposcopy clinic). Thus, the populations included in this evaluation are generalizable to the U.S. screening population. A limitation of using these exclusion criteria is that our concordance range does not have external validity to those with history of HPV+ or abnormal cytology. Further research is needed to compare the concordance in high-risk populations compared with general screening populations to elucidate if significant differences exist between concordances.
Another possible limitation of the study is the varying methodologies used to obtain cervical samples. As reflected in Table 1, the device used to collect samples varied. Studies included devices such as cytobrushes, cotton swabs, Dacron swabs, and spatulas—common in U.S. clinical practice. We excluded non-cervicovaginal swab methods such as tampons, sanitary pads, and urine samples as they are not standardized, validated instruments used in the United States. Further research is needed to assess validity of these methods compared with typical clinician-collected samples using cervicovaginal swabs.
It is reasonable to provide self-collected primary HPV screening options as a method for screening for cervical cancer. The quality of samples provided by patients is equivalent to that of clinician-collection. To optimally and equitably implement self-collection, commercial testing kits should be made available, clinicians should be coached on discussing this with patients, and public health messaging should include this as an option to remain up-to-date with cancer screenings.
Footnotes
Acknowledgments
The authorship team would like to thank the Virginia Commonwealth University Department of Family Medicine and Population Health for their support of this research.
Authors' Contributions
S.B.: Conceptualization, formal analysis, investigation, methodology, project administration, visualization, writing—original draft, writing—review and editing. J.W.C.: Methodology, formal analysis, software, writing—review and editing. A.N.H.: Conceptualization, data curation, formal analysis, methodology, resources, supervision, visualization, writing (original and review and editing).
Author Disclosure Statement
No competing financial interests exist.
Funding Information
The authorship team did not receive any funding for the work or publication of this article. Covidence access was sponsored by the C. Kenneth and Dianne Wright Center for Clinical and Translational Research (CTSA Award No. UL1TR002649 from the National Center for Advancing Translational Sciences).
Supplementary Material
Supplementary Table S1
Supplementary Appendix SA1
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.