
Abstract
Background:
Cancer survivors are often reluctant to discuss sexual complaints with their oncologists and treatment is frequently unsatisfactory due to paucity of controlled studies and inapplicability of vaginal estrogen. We aimed to evaluate efficacy and tolerability of platelet-rich plasma (PRP) injections alone or in combination with noncrosslinked hyaluronic acid compared with standard therapy with topical hyaluronic acid gel in the management of cancer therapy-induced or aggravated vulvovaginal atrophy.
Materials and Methods:
This prospective, parallel-group comparative study was conducted on 45 female patients with a history of cancer and complaining of symptoms of vulvovaginal atrophy either induced or aggravated by cancer treatment. Patients were randomly divided into three groups (A, B, and C). Group A patients received two submucosal vaginal PRP injections, group B patients received two similar injections of PRP combined with noncrosslinked hyaluronic acid, and group C received a topical vaginal hyaluronic acid gel applied three times weekly for 2 months. Main outcome measures were vulvovaginal atrophy symptom severity and vaginal health index (VHI) scores before treatment (v0), 1 month from baseline (v1), 2 months from baseline (v2), and 3 months after the last visit (v3).
Results:
Both groups A and B showed greater improvement of frequency of intercourse avoidance than group C. Group A showed greater improvement of dyspareunia than group C. Groups A and B demonstrated greater improvement of vaginal pH, fluid volume, and total VHI scores than group C. Short-term topical hyaluronic acid (HA) was not associated with any significant improvement of vaginal elasticity. Group B showed greater improvement of vaginal dryness and moisture scores than group C. Reported adverse events were injection-related pain in all patients of groups A and B and vaginal spotting in groups A and B.
Conclusion:
Both PRP and PRP-HA have comparable efficacy and patient-reported treatment satisfaction. PRP injections were better tolerated by patients than PRP-HA. Clinical trial registration number: NCT05782920.
Introduction
The risk of vulvovaginal atrophy (VVA) is five to six times higher in cancer patients compared with other females. 1 By virtue of the globally increasing incidence of cancer in patients younger than 50 years, 2 VVA or genitourinary symptoms of menopause (GSM) is becoming a frequently encountered problem in young female cancer survivors, who experience premature menopause as a result of their oncologic treatment. 3 The underlying pathology is chronic estrogen depletion secondary to chemotherapy, oophorectomy, pelvic radiotherapy, systemic endocrine therapy, or hormonal treatments such as GnRH analogues, tamoxifen, and aromatase inhibitors. The commonly prescribed endocrine therapy and, importantly, aromatase inhibitors can either induce VVA or aggravate preexisting menopausal VVA symptoms. 3
Chronic estrogen depletion induces several structural changes in the genital tissues such as reduced cellular proliferation and epithelial thickness, increased fragmentation of elastin, and collagen hyalinization. This in turn promotes an inflammatory cell infiltrate causing vascular damage, reduced blood flow, decreased glandular function, epithelial thinning, decreased elasticity, and an elevated vaginal pH. 3,4 Clinically, VVA manifests by a constellation of symptoms of vaginal dryness, itching, irritation, dyspareunia, dysuria, and symptoms of frequent urinary tract infections. These chronic symptoms can negatively affect the patients' sexual function and satisfaction, thereby threatening patients' compliance with the systemic drugs mandatory for maintenance of cancer remission. Patients may discontinue treatment and thereby affect cancer-related outcomes. 5
Many oncologists refrain from prescribing the “gold standard” topical estrogen as it is not applicable in patients receiving antiestrogens and for fear of increased risk of systemic absorption and cancer recurrence in women with hormone receptor-positive breast cancer. 3,5 The recommendations of the international society for the study of vulvovaginal disease propose moisturizers and lubricants are first-line therapy in cancer survivors. 6 Vaginal moisturizers containing water and other ingredients such as hyaluronic acid or polycarbophil, considered first-line treatment can only produce temporary relief. They act by adhering to the vaginal mucosa increasing hydration and improving epithelial integrity and elasticity. 7 Nevertheless, the use of the commonly practiced laser procedures as well is not yet endorsed out of the setting of clinical trials. 6 Treatment of VVA in cancer patients remains inadequate, with several uncontrolled case reports suggesting possible therapeutic effects of submucosal vaginal injections of platelet-rich plasma (PRP) and hyaluronic acid. 8,9
PRP is known to stimulate cellular proliferation, differentiation, angiogenesis, and tissue remodeling through its content of growth factors. Therefore, it was suggested that PRP could assist in tissue repair, healing, regeneration, in addition to skin and vulvovaginal rejuvenation. 10,11 Since hyaluronic acid is naturally present in vaginal tissues, hyaluronic acid (HA) formulations were suggested to be an alternative nonhormonal promising strategy to increase hydration and improve VVA. 12 Hyaluronic acid adheres to the vaginal mucosa and improves diffusion of water and electrolytes to the dermal vasculature, thereby inducing vasodilatation and increasing mucosal blood flow. HA gels were shown to adhere to the mucosa for 3 days until exfoliation of the epithelium occurs. 4
Data from literature suggest that treatment with hyaluronic acid produces comparable improvements of epithelial atrophy, vaginal pH, dyspareunia, and cell maturation when compared with vaginal estrogens. 4 It has been proposed that therapeutic effects of HA could be maximized if injected in the superficial epithelial layers rather than used topically. 13 We aimed to evaluate the efficacy and tolerability of PRP injections alone or in combination with noncrosslinked hyaluronic acid compared with the control group using a control conventional therapy of topical hyaluronic acid gel in the treatment of cancer therapy-induced or aggravated VVA and its impact on sexual function and satisfaction.
Materials and Methods
Patients
This prospective, parallel-group comparative study was conducted on 45 female patients with a history of cancer and complaining of symptoms of VVA induced or aggravated by their cancer treatment. Patients were recruited from the oncology outpatient clinic of the main university hospital of Alexandria University in the period between August 2020 and March 2021. Approval of the local ethics committee (IRB no. 00012098) was obtained (no. 0201349) and a written informed consent was obtained from all subjects before inclusion in the study. The study procedures were carried out according to the principles of the 1975 Declaration of Helsinki.
Sample size calculation
We performed a repeated-measure analysis of variance (ANOVA) considering the number of groups = 3 and the number of measurements = 4 visits. Sample size was calculated using G-power 3 software (Heine University Dusseldorf, Dusseldorf, Germany), adjusting power at 80% and the level of confidence at 95%. The effect size was 0.43 based on mean vaginal health index (VHI) scores of 13.8 with topical hyaluronic acid versus 16.5 in the combined PRP-HA group and 16.59 in the PRP group at 1 month after the end of therapy. 9,14,15 The estimated minimal total sample size was 36 patients approximated to 45 patients divided into 15 patients in each treatment group.
We enrolled sexually active cancer survivors diagnosed as postmenopausal (at least 12 months of spontaneous amenorrhea or 6 weeks following bilateral oophorectomy, discontinuation of tamoxifen or pelvic radiotherapy with amenorrhea, and serum levels of estradiol ≤30 pg/mL and follicle stimulating hormone ≥50 IU/L) at the time of inclusion into the study. Patients were included if they had at least one of the vulvovaginal symptoms (vaginal dryness, burning, itching, or dyspareunia) self-reported as severe (0—absent, 1—mild, 2—moderate, 3—severe) and/or a VHI <15.
Exclusion criteria of the study included active or recent history of vulvovaginal and/or perineal bacterial, fungal or viral infection or inflammation, and any suspicious undiagnosed vulvovaginal lesions on gynecological examination. Patients with known hypersensitivity to hyaluronic acid, the antiseptic solution, and the local analgesic used in the study were also excluded. We excluded patients with a history of or active autoimmune disease, patients on antidepressant agents within the last month, and patients with a history of recurrent streptococcal infections or acute rheumatic arthritis or toxic shock syndrome. Patients with ongoing or history of vulvar, vaginal, or cervical cancer or ongoing cancer such as hormone-dependent breast cancer and patients on antiestrogen treatment (tamoxifen, aromatase inhibitor) for hormone-dependent breast cancer within 1 year before the study were excluded.
Patients on anticoagulant, antiplatelet agents, non steroidal anti-inflammatory drugs or vitamin C in the previous week, those on targeted electromagnetic treatment of the vaginal mucosa (pulsed CO2 laser, LED, radiofrequency, etc.) within the previous 6 months, patients who used local hyaluronic acid-like hydrating treatment within 4 weeks, patients treated with PRP, HA fillers, noncrosslinked HA within 1 year, and those who received vestibular and/or vaginal treatment with nonresorbable implants were excluded. Patients on topical vaginal or systemic hormonal treatments were excluded from the study. We also excluded patients who received selective estrogen receptor modulator treatment targeted against vaginal dryness (ospemifene, etc.) within the preceding month.
Methods
Patients were randomly assigned into three groups (A, B, and C) of 15 patients, each by the systemic randomization method.
Group A patients received two submucosal vaginal PRP injections into the outer 3 cm of the vagina spaced 1 month apart.
Preparation of autologous PRP
PRP was prepared as per the American Association of Blood Banks Technical Manual. 16 Fifteen milliliters of whole blood was withdrawn by venipuncture and collected in acid citrate dextrose tubes. The blood samples were centrifuged by a Selecta P Centromix centrifuge (Grupo Selecta, Barcelona, Spain), first using a “soft” spin at 2000 rpm for 5 minutes. The supernatant plasma containing platelets was transferred into another sterile tube (without anticoagulant) and then centrifuged at a higher speed (a hard spin) of 4000 rpm for 15 minutes to obtain a platelet concentrate. The platelet-poor plasma was discarded, and the tube was gently shaken to suspend the platelet pellets in plasma. Calcium gluconate was added for activation. 16 This method of preparation was chosen on the basis that double-centrifugation protocol results in higher platelet concentrations than the single centrifugation protocol. 17
Another sample was taken and prepared as previously mentioned for examination of platelet count in PRP. A platelet concentration of more than 1 million/μL (approximately four to seven times the mean levels) was regarded a successful preparation as this count is generally considered a therapeutically effective concentration of PRP. 18
Injection technique
Patients were instructed to wash the vulvar and vaginal areas thoroughly. Careful inspection of the vulvar and vaginal areas was done to exclude the presence of any infections or suspicious lesions before injection. A 3-mL syringe without needle was used as a vaginal applicator to apply a mixture of topical lidocaine 2.5% and prilocaine 2.5% (pridocaine cream; Global Napi Pharmaceutical, Egypt) into the vestibule and the first 3 cm of vagina, 15 to 30 minutes before the injection session. The vaginal and vulvar areas were then cleaned with saline and sterilized with Betadine-soaked sterile dressing. Three cubic centimeters of PRP was injected through mucosal and submucosal injections every 5 mm into the vestibule and the first 3 cm of the lateral and posterior vaginal walls (0.1 mL/point) with a 27-gauge needle and a 5-mL syringe. An amoxicillin–clavulanic acid prophylaxis was prescribed for 48 hours.
Group B patients received two submucosal vaginal injections of PRP combined with noncrosslinked hyaluronic acid injections into the outer 3 cm of the vagina spaced 1 month apart. One milliliter of noncrosslinked hyaluronic acid 3% (Simildiet Laboratorios, Spain) was mixed with 3 cubic centimeters of PRP in a 5 mL syringe converting it to a more viscous solution and then injected in a similar technique to group A.
Group C patients received one applicator (5 gm) of topical hyaluronic acid gel for vaginal application applied three times per week for a 2-month duration. The topical HA gel was prepared in the faculty of pharmacy according to the following protocol. To prepare 100 g of HA gel (1%), 1 g of high-molecular-weight HA 99% purity (Orchidia) and 0.5 g of carbopol (0.5%w/w) and 0.25 hydroxypropyl methyl cellulose were dispersed in 100 mL of deionized water at low pH (3.5), while stirring at 600 rpm at 25°C overnight till complete dispersion of HA, giving a clear solution. The pH was then adjusted to 5.4, where a clear viscous gel formed.
Clinical evaluation
Patients were evaluated for symptom severity regarding vaginal dryness, dyspareunia, and frequency of intercourse avoidance before treatment at the baseline visit (v0), 1 month after the baseline visit (v1), 2 months after the baseline visit (v2), and a follow-up visit 3 months after the last visit (v3). Dryness and dyspareunia were assessed on a visual analogue scale (VAS) from 0 to 10: 0—no symptoms, mild symptoms (1–3), moderate symptoms (4–6), and severe symptoms (7–10). The frequency of intercourse avoidance was assessed on a 4-point frequency rating Likert scale: 0—never, 1—rarely, 2—often, and 3—always.
For assessment of VVA signs, the patients were examined by a single independent blinded gynecologist for calculating the VHI. which is a clinical tool evaluating five parameters (vaginal elasticity, vaginal secretions, pH, epithelial mucous membrane integrity, and vaginal hydration). Each domain was given a score from 1 to 5. Total scores of the VHI range from 5 to 25, with lower scores denoting more severe atrophy. A final total score of less than 15 diagnosed VVA. 19 Assessments of the vaginal pH by vaginal pH test strips (Pangaea LLC, MA), elasticity, epithelial mucosal integrity, fluid secretion (type and consistency), and moisture were made before treatment and during each visit.
Patient-reported treatment satisfaction was evaluated at (v2) as very satisfied, satisfied, neutral, nonsatisfied, and very unsatisfied. Patients were followed for occurrence of side effects during visits including injection-associated pain. Pain duration was noted, and severity was evaluated by asking the patients to rate the severity on a VAS of a 10 cm line, with two ends; 0 representing “no pain,” “1–3” as mild pain, “4–6” moderate pain, and “7–10” severe pain.
Data analysis
Data were fed to the computer and analyzed using IBM SPSS statistics program version 28 (IBM Corp, Armonk, NY) and R software packages (v4.1.2; R Core Team 2021) at 0.05 significance level. The Shapiro–Wilk test was used to verify the normality of distribution. Quantitative data were described using range (minimum and maximum), mean, standard deviation, median, and interquartile range. The used tests were chi-square test for categorical variables, to compare between different groups, and Fisher's exact or Monte Carlo correction for chi-square when more than 20% of the cells had expected counts less than 5.
We conducted a mixed design repeated-measures ANOVA test to study the main effect of time, main effect of treatment (PRP, PRP-HA, topical HA treatment), and if a significant interaction was present in the form of change pattern of outcomes along different periods between the three groups. Pairwise comparisons were conducted by post hoc Bonferroni test for significant results. Multiple linear regression analysis was done to determine the impact of age, other patients' baseline characteristics, and treatment modality (PRP and PRP-HA vs. the control topical HA gel) on the mean total VHI score at v2 (as a proxy of treatment response).
Results
Clinical characteristics of the studied groups
Patients' age ranged from 26.0 to 55.0 years with mean age of 44.33 ± 8.56, 40.67 ± 6.31, and 48.33 ± 7.68 years in groups A, B, and C, respectively. History of previous deliveries showed that 25 patients (55.5%) in our cohort had undergone vaginal delivery, 12 patients (26.6%) underwent cesarean section, and 2 patients (4.4%) reported both vaginal delivery and cesarean section. Gestational history revealed that 6 females (13.3%) were nulliparous, and 39 patients (86.7%) were multiparous. The predominant cancer was breast cancer in 13 (86.5%), 12 (80%), and 13 (86.7%) patients in groups A, B, and C, respectively. Patients reported receiving chemotherapy alone, chemotherapy and antiestrogen, or both chemotherapy and oophorectomy with pelvic radiotherapy.
Menopausal symptoms were induced by cancer therapy in 14 (93.3%), 15 (100%), and 11 (73.3%) patients in groups A, B, and C, respectively, and were worsened by cancer treatment in 1 (6.7%) and 4 (26.7%) patients in groups A and C, respectively. Table 1 summarizes the oncologic history and associated menopausal status of the studied groups.
Patients' Characteristics in the Three Studied Groups
Group A: PRP- treated females. Group B: Combined PRP noncrosslinked hyaluronic acid-treated females. Group C: Topical hyaluronic acid gel-treated females.
PRP, platelet-rich plasma.
Results of the mixed ANOVA comparisons for VVA symptoms
Vaginal dryness
A significant interaction effect was demonstrated denoting that the pattern of change of mean dryness outcomes differed along time by treatment groups (p c = 0.011). The mean vaginal dryness scores of the three studied groups decreased from baseline scores over the study visits, more so in the PRP and PRP-HA groups than the topical HA group till v2. Mean vaginal dryness scores then showed a substantial increase in the topical HA group returning to nearly pretreatment scores at v3, whereas mean scores were still significantly lower than pretreatment scores in the PRP and PRP-HA groups (Fig. 1). Analysis also revealed an overall significant main effect of time where there was a significant change of mean dryness scores at v1, v2, and v3 from baseline visit (v0) (p a < 0.001). A significant difference existed at each time point from baseline (v0) for the PRP and combined PRP-HA groups (p < 0.05).
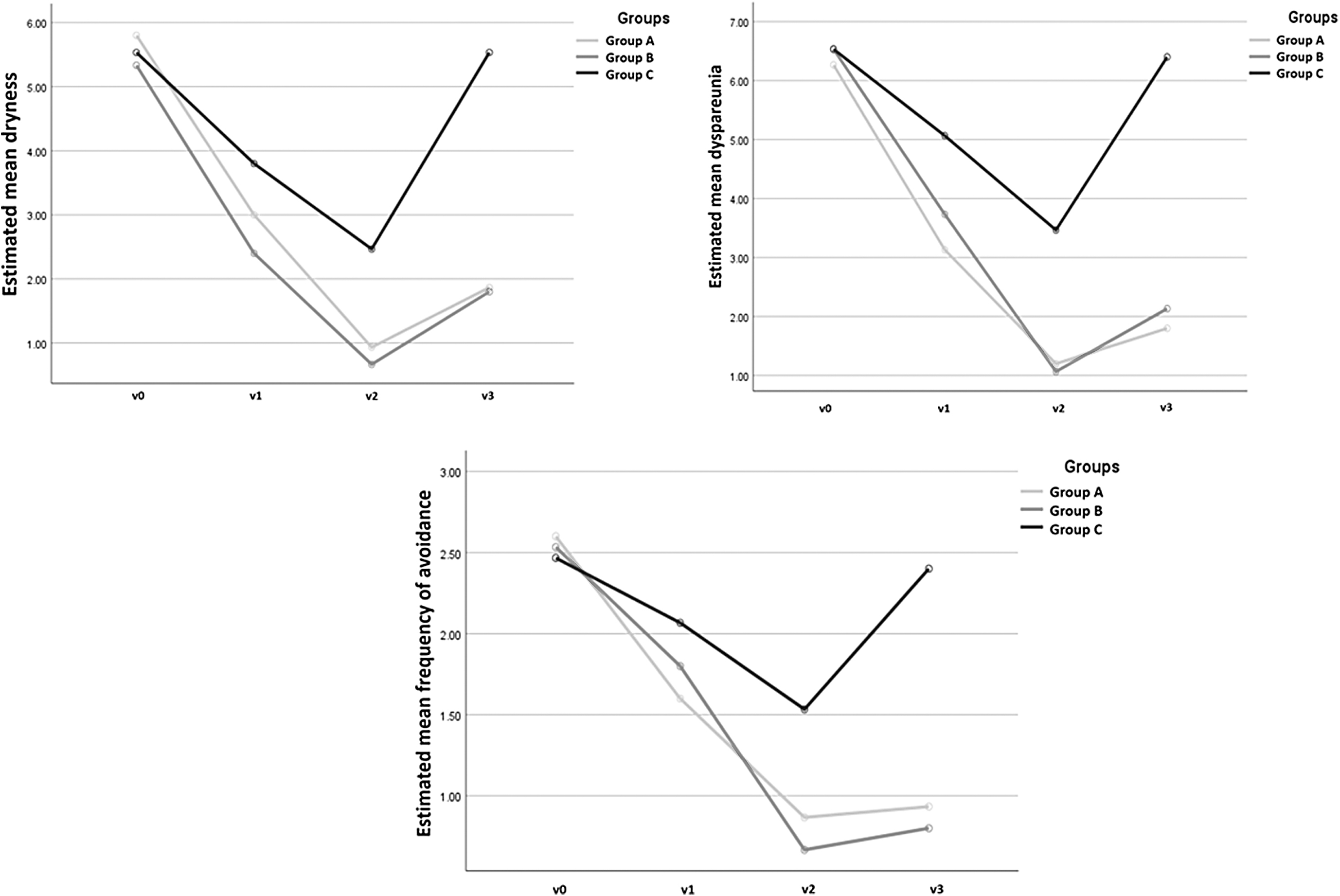
Vulvovaginal symptoms (vaginal dryness, dyspareunia, and frequency of intercourse avoidance) throughout the study period in the three studied groups. Group A: PRP-treated females. Group B: Combined PRP noncrosslinked hyaluronic acid-treated females. Group C: Topical hyaluronic acid gel-treated females. V0: Baseline, V1: 1 month, V2: 2 months, V3: 3 months of follow-up. PRP, platelet-rich plasma.
However, for the topical HA treatment group, there was an insignificant difference of mean dryness from baseline (v0) at v3 assessment (p > 0.05). Also, a significant main effect of the type of treatment existed (p b < 0.001*), with a significant difference existing between groups B and C where group B patients had significantly lower mean vaginal dryness scores that group C patients (p = 0.013) (Table 2).
Mixed Design Repeated-Measures Analysis of Variance Test of Mean Vulvovaginal Atrophy Symptoms at Different Follow-Up Periods for Groups A, B, and C
Mixed design repeated-measures ANOVA test. p a for the main effect of time on different parameters averaged across groups; p b for main effect of different treatment groups averaged across time; p c for the interaction to assess the pattern of change of each quantitative variable along time by treatment groups; p GroupA/p GroupB/p GroupC: for post hoc comparisons.
Significant results ≤.05. #Significant pairwise comparison with baseline.
Group A: PRP-treated females. Group B: Combined PRP noncrosslinked hyaluronic acid-treated females. Group C: Topical hyaluronic acid gel-treated females.
ANOVA, analysis of variance; HA, hyaluronic acid.
Dyspareunia
A significant interaction effect was observed denoting that the pattern of change of mean dyspareunia outcomes along time differed by treatment groups (p c < 0.011). The mean scores of dyspareunia declined from baseline scores over the visits till the end of treatment (v2) in the three studied groups, but more so with the PRP and PRP-HA groups. Mean dyspareunia scores then increased to nearly pretreatment scores in the topical HA group at v3 and less in the PRP-HA and PRP groups to mean scores lower than baseline scores (Fig. 1). Analysis revealed an overall significant main effect of time, implying a significant change in dyspareunia scores at v1, v2, and v3 from baseline visit (v0) (p a < 0.001). A significant difference existed at each time point from baseline (v0) for the PRP and combined PRP-HA groups (p < 0.05).
However, for topical HA treatment group, there was an insignificant difference of mean dyspareunia scores at v3 from baseline v0 assessment (p > 0.05). Also, a significant main effect of type of treatment existed (p b < 0.001), with a significant difference existing between groups A and C where group A patients showed significantly lower mean dyspareunia scores than group C patients (p < 0.001) (Table 2).
Frequency of intercourse avoidance
A significant interaction effect was demonstrated denoting that the pattern of change of mean frequency of avoidance outcomes along time differed by treatment groups (p c = 0.009). The mean scores of frequency of intercourse avoidance in the three studied groups decreased over the visits till v2, more with the PRP-HA and PRP groups. Mean scores then increased to nearly pretreatment scores in the topical HA group at v3, but less with the PRP-HA and PRP groups to mean scores significantly lower than baseline scores (Fig. 1). Analysis also revealed an overall significant main effect of time where there was a significant change in mean frequency of intercourse avoidance scores at v1, v2, and v3 from baseline visit (v0) (p a < 0.001). A significant difference existed at each time point from baseline (v0) for the PRP and combined PRP-HA groups and at v2 for the topical HA group (p < 0.05).
For the topical HA treatment group, there was an insignificant difference from baseline (v0) at v3 assessment (p > 0.05). Also, a significant main effect of type of treatment existed (p b < 0.001) with a significant difference existing between groups A and C (p = 0.029) and between groups B and C (p = 0.016), where both groups A and B showed significantly lower mean frequency of avoidance scores compared with group C (Table 2).
Results of the mixed ANOVA comparisons for total VHI and its domains
Vaginal pH
A significant interaction effect was shown denoting that the pattern of change of mean pH outcomes along time differed by treatment groups (p c = 0.004) (Fig. 2). Mean pH scores increased in the three groups but more so in the PRP and PRP-HA groups till v2. Mean pH scores then declined in the three groups to nearly pretreatment scores in the topical HA group at v3, but decreased less with the PRP and PRP-HA groups to scores still higher than baseline scores. There was a significant main effect of time, where there was a significant change of mean pH over time at v1, v2, and v3 from baseline (v0) (p a < 0.001). There was a significant difference observed at each time point from baseline (v0) for groups A and B. However, for group C, an insignificant difference was noted at v3 from baseline (v0) (p > 0.05).
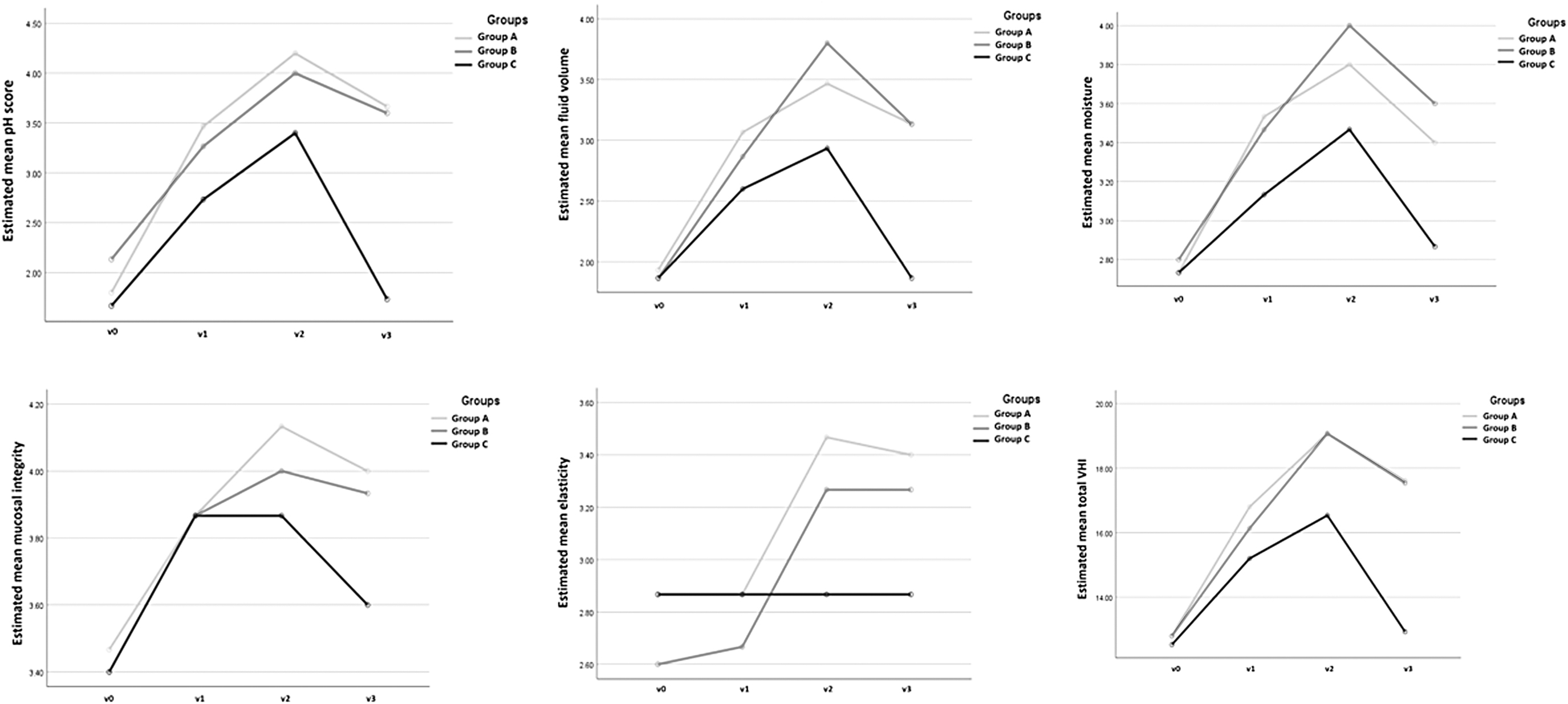
Vaginal health index (total and domain) scores during the study period in the three studied groups. Group A: PRP-treated females. Group B: Combined PRP noncrosslinked hyaluronic acid-treated females. Group C: Topical hyaluronic acid gel-treated females.
There was a significant main effect by treatment group (p b < 0.001), where both groups A and B had significantly higher mean pH scores compared with group C (p = 0.009, p = 0.012, respectively (Table 3).
Mixed Design Repeated-Measures Analysis of Variance Test of Mean Vaginal Health Index Scores (Total and Domains) at Different Follow-Up Periods for Groups A, B, and C
Mixed design repeated-measures ANOVA test. p a for the main effect of time on different parameters averaged across groups; p b for main effect of different treatment groups averaged across time; p c for the interaction to assess the pattern of change of each quantitative variable along time by treatment groups; p GroupA/p GroupB/p GroupC: for post hoc comparisons. Group A: PRP-treated females. Group B: Combined PRP noncrosslinked hyaluronic acid-treated females. Group C: Topical hyaluronic acid gel-treated females.
Significant results ≤0.05.
Significant pairwise comparison with baseline.
VHI, vaginal health index.
Vaginal elasticity
There was a significant main effect of time, where there was a significant change of mean elasticity scores over time from baseline (v0) (p a < 0.001). A significant difference was observed only at v2 and v3 from baseline in groups A and B. For group C, however, an insignificant difference was noted for elasticity at each visit v1, v2, and v3 from baseline (v0) (p > 0.05) (Fig. 2). Although there was a significant change of elasticity over the study visits, the main effect by treatment type was insignificant (p b = 0.247) and the visit–group interaction did not reach significance (p c = 0.096) (Table 3).
Moisture
A significant interaction effect existed, which denoted that the pattern of change of mean moisture outcomes along time differed by treatment groups (p c = 0.040). Mean moisture scores of the three groups increased from baseline in the three groups over the study visits, but more so in the PRP-HA and PRP groups than the topical HA group till v2. Mean scores then declined to baseline scores in the topical HA group, but to scores greater than pretreatment scores in the PRP-HA and PRP groups (Fig. 2). There was a significant main effect of time denoting a significant change of mean moisture scores over time at v1, v2, and v3 from baseline (v0) (p a < 0.001).
There was a significant difference observed at each time point from baseline (v0) for groups A and B. However, for group C, an insignificant difference was noted for moisture at v3 from baseline (v0) assessment (p > 0.05). There was also a significant main effect by treatment group (p b = 0.012), where group B had significantly higher mean moisture scores than group C (p = 0.013) (Table 3).
Vaginal fluid volume
A significant interaction pattern existed denoting that the pattern of change of mean fluid volume outcomes along time differed by treatment groups (p c = 0.004). Pretreatment mean scores increased over the study periods more with PRP-HA and PRP groups till v2. Mean scores then decreased more so with the topical HA reaching baseline scores, but to a lesser extent in the PRP-HA and PRP groups to scores significantly better than pretreatment scores (Fig. 2). We demonstrated a significant main effect of time denoting a significant change of mean fluid volume scores over time at v1, v2, and v3 from baseline (v0) (p a < 0.001). There was a significant difference observed at each time point from baseline (v0) for groups A and B. However, for group C, an insignificant difference was noted for fluid volume at v3 from baseline (v0) assessment (p > 0.05). There was also a significant main effect by treatment group (p b < 0.001), where groups A and B had significantly higher mean fluid volume scores than group C (p = 0.012, p = 0.010, respectively) (Table 3).
Mucosal integrity
There was a significant main effect of time denoting a significant change of mean mucosal integrity scores over time at v1, v2, and v3 from baseline (v0) (p a < 0.001). There was a significant difference observed at each time point from baseline (v0) for groups A and B. However, for group C, an insignificant difference was noted for mucosal integrity at v3 from baseline (v0) assessment (p > 0.05). Although there was a significant change of mucosal integrity over the study visits, the main effect by treatment type was insignificant (p b = 0.334) and the interaction effect did not reach significance (p c = 0.261) (Table 3).
Total VHI
A significant interaction effect was shown denoting that the pattern of change of mean total VHI outcomes along time differed by treatment groups (p c < 0.001). Pretreatment mean scores showed an increase over the study visits, more so with the PRP-HA and PRP groups than the topical HA group till v2. Mean scores then decreased, more with topical HA, but more steadily in PRP-HA and PRP groups to scores significantly higher than pretreatment scores (Fig. 2). We reported a significant main effect of time denoting a significant change of mean total VHI scores over time at v1, v2, and v3 from baseline (v0) (p a < 0.001). There was a significant difference observed at each time point from baseline (v0) for groups A and B. However, for group C, an insignificant difference was noted for total VHI at v3 from baseline (v0) (p > 0.05).
There was also a significant main effect by treatment type (p b < 0.001), where both groups A and B had significantly higher mean total VHI scores than group C (p = 0.01, p = 0.003, respectively) (Table 3).
Vaginal tightening at v2
At v2, 6 patients (40%) and 10 patients (66.6%) in groups A and B, respectively, reported a sense of vaginal tightening, which was not reported by any of the patients in group C (p = 0.001). There was no statistically significant difference between groups A and B (p = 0.143), while the difference between group C and each of the groups A and B was significant (p = 0.001).
Patient-reported treatment satisfaction at v2
In group A, 10 patients (66.7%) and 4 patients (26.7%) reported being satisfied and very satisfied, respectively, at v2. Only 1 subject (6.7%) reported being very unsatisfied. In group B, nine patients (60%) and three patients (20%) reported satisfied and very satisfied, respectively, at v2. Three patients (20%) reported being neutral. In group C, two patients (13%) and six patients (40%) reported being satisfied and very satisfied at v2, whereas five patients (33.3%) reported being neutral and two patients (13.3%) reported being very unsatisfied. There was a statistically significant difference between the three studied groups regarding patient-reported treatment satisfaction at v2 (p = 0.013). Both group A and B patients showed significantly higher satisfaction than group C (p < 0.001), with no statistically significant difference between groups A and B (p = 0.246).
Side effects in the three studied groups
Reported adverse events were injection-related vaginal pain in all patients of groups A and B, and vaginal spotting was observed the day after the injection in two patients (13.3%) and one patient (6.6%) in groups A and B, respectively. The mean score of the first PRP or PRP-HA injection-related pain on VAS was 6.27 ± 1.16 in PRP+HA group and 2.87 ± 2.03 in PRP group (p < 0.001). The pain duration was 1.69 ± 0.75 and 3.93 ± 2.49 days in groups A and B, respectively (p = 0.004). At the second injection, the mean pain score was 4.73 ± 1.33 in PRP+HA group and 2.27 ± 1.83 in PRP group (p = 0.001). The pain duration was 1.09 ± 0.30 and 3.27 ± 2.12 days in groups A and B, respectively (p = 0.002). No side effects were reported in any of the patients of group C.
Multivariate linear regression of factors affecting mean total VHI score of the study subjects at v2
Results of the multivariate linear regression analysis showed that the treatment modalities, that is, PRP and PRP-HA, were the only significant predictors of treatment response in groups A and B (p = 0.002, p = 0.004, respectively) (Tables 4 and 5).
Multiple Linear Regression Analysis for the Different Predictors Affecting Mean Total Score Vaginal Health Index at v2 in Groups Receiving Platelet-Rich Plasma and the Group Receiving Topical Treatment (n = 30)
B, regression coefficient; F, the overall model is significant, p = 0.006 * ; R 2, 47.5% of the variability in VHI is accounted for/attributed to significant factors in the model (the intervention/PRP); B, receiving PRP increases the total vaginal health index at visit 2 (VHI at v2) by 2.695 units compared with receiving topical treatment (B = 2.695). The intervention is the only significant predictor of mean total VHI at v2 in the model.
Statistically significant at p < 0.05.
CI, confidence interval; LL, lower limit; UL, upper limit; VHI, vaginal health index.
Multiple Linear Regression Analysis for the Different Predictors Affecting Mean Total Score at v2 After Second Treatment in Groups Receiving Platelet-Rich Plasma+Hyaluronic Acid and the Group Receiving Topical Treatment (n = 30)
B, regression coefficient; F, the overall model is significant, p = 0.005 * ; R 2, 48% of the variability in VHI is accounted for/attributed to significant factors in the model (the intervention/PRP+HA); B, receiving PRP+HA increases the total vaginal health index at visit 2 (VHI at v2) by 2.292 units compared with receiving topical treatment (B = 2.292). The intervention is the only significant predictor of mean total VHI at v2 in the model.
Statistically significant at p < 0.05.
Discussion
There are several obstacles to the management of VVA in cancer patients. First, sexuality is not routinely addressed during oncologic counseling of cancer survivors. Affected females are often shy to report their symptoms. 20 Furthermore, available treatment options for women with VVA secondary to cancer and/or cancer therapy are of poor efficacy. Estrogen hormonal therapy is the preferred option 1 in addition to vaginal estrogens, dehydroepiandrosterone, and ospemifene. 21 but believed by the majority of oncologists to increase the risk of cancer recurrence. 1,22 Alternatively, nonhormonal treatment options are therefore preferred among many cancer survivors. Vaginal lubricants offer symptomatic relief of vaginal dryness during intercourse, but are not an effective option for this chronic problem. Radiofrequency and several laser sources, such as microablative carbon dioxide (CO2; 10,600 nm) and nonablative erbium-YAG (2940 nm), have been proposed for the treatment of GSM. 23,24
Fractional CO2 laser was shown to be an effective modality for treatment of VVA in menopausal females with no serious complications encountered for up to 6 months of follow-up after treatment. 25 A recent systematic review of nine studies also concluded that fractional CO2 laser was safe and effective in managing vaginal atrophy and sexual dysfunction in gynecological cancer survivors. Fractional CO2 laser is suggested to act through thermal-dependent matrix remodeling and angiogenesis, thereby increasing vaginal elasticity, moisture, and epithelial integrity. 26 Furthermore, a combination of hyaluronic acid, curcumin, quercetin, and chondroitin sulfate was suggested to be effective in reducing the occurrence of recurrent urinary tract infections and urinary symptoms in menopausal 27 and premenopausal females. 28
PRP and hyaluronic acid have shown efficacy in enhancing tissue regeneration and rejuvenation. 29,30 This supports a possible indication in the management of VVA symptoms. Available HA fillers are composed of crosslinked HA, which is less appropriate for areas of thin dermal layer and less subcutaneous tissue fat. Nodules are also reported as a complication of crosslinked HA injection. Given, the safety for superficial injections, noncrosslinked HA may offer less side effects and greater safety in such areas. However, it is well known that noncrosslinked HA has a much shorter duration of action, Therefore, it is worthy to combine other active ingredients with noncrosslinked HA. 31 We attempted to compare the efficacy and tolerability of using PRP, PRP combined with noncrosslinked HA versus the standard topical HA gel in management of VVA in female patients with a history of cancer treatment.
In our study, patients' ages ranged from 26.0 to 55.0 years. This relatively young age for menopause reflects the worldwide reported increased prevalence of cancer in younger ages, who are therefore exposed to the risk of early menopausal symptoms. Normally in young ages, the vaginal epithelium exfoliates releasing glycogen that is acted upon by lactobacilli to produce lactic acid that helps maintain the healthy acidic pH of the vagina (3.5–4.5). Iatrogenic estrogen depletion predisposes to vaginal epithelial thinning with decreased exfoliation of glycogen-rich cells and increased vaginal pH (5–7.5) and thereby an altered vaginal microbiota and pathogenic bacterial overload predisposing to urogenital infections that present clinically by vaginal dryness and pain.
Estrogen deficiency also leads to a reduced vaginal blood flow, vaginal canal shortening, mucosal thinning, and loss of vaginal elasticity secondary to elastin fragmentation and collagen fiber hyalinization. As estrogen normally increases HA synthesis (up to 11-fold), HA level also declines severely with estrogen depletion. 12 Patients suffer from thinning of the labia minora, decreased subcutaneous fat of the labia majora, and contraction of the introitus. The reduced blood flow and reduced vaginal secretions result in pallor and dryness of the vaginal epithelium. These changes are secondary to reduced proliferation of the vaginal epithelial cells, altered extracellular matrix remodeling, and reduction of glycosaminoglycans particularly HA. 12
In our cohort of PRP-treated females, we reported an improvement of VVA symptoms as early as 1 month. Similarly, Cynthia et al. 32 reported considerable improvement of VVA symptoms after two sessions of PRP injections in a case series of seven patients with vaginal penetration disorders. We also reported significant improvements of vaginal fluid volume, pH, mucosal integrity, and moisture as early as the first month after PRP injection. The elasticity domain, however, showed a significant improvement later at 2 months. In agreement with our study, Melo 8 reported an improvement of total VHI score from a pretreatment score of 9 to 20 after 4 months of monthly PRP and platelet poor plasma application to the vaginal walls and introitus in one patient following pelvic radiotherapy. PRP was also reported to restore normal vaginal lubrication in 60% of treated females after pelvic irradiation. 33
Saleh and Abdelghani 14 similarly reported a highly significant improvement of the total VHI in females with postmenopausal vaginal atrophy. They reported statistically significant differences between pre- and post-treatment parameters of all VHI domains for 1 month following two sessions of PRP injections in postmenopausal vaginal atrophy. These findings support the role of PRP in managing cancer therapy-induced VVA. PRP is believed to exert its biological effect through stimulation of regeneration by virtue of its content of concentrated growth factors (platelet-derived growth factors, transforming growth factors b, epithelial growth factors, vascular endothelial growth factor, insulin-like growth factor, basic fibroblast growth factors), which stimulate cell proliferation, differentiation, neoangiogenesis, and extracellular matrix production. 9
It can be suggested that PRP injection in the female genital tract through stimulation of neoangiogenesis, cellular proliferation, and differentiation, glandular (Skene's glands) and neuronal proliferation can improve symptoms of VVA such as vaginal dryness and pain. The increased neuronal growth, collagen, and extracellular matrix synthesis can improve vaginal responsiveness, which improves further vaginal elasticity and reduces coital pain and discomfort. 32 Our findings also suggest that the effect of PRP injections starts early. The later onset of elasticity improvement observed at 2 months versus the rest of VHI domains in our study might be explained by the time required for PRP-stimulated extracellular matrix synthesis and remodeling.
However, at the 3-month follow-up of the PRP-treated cohort, we demonstrated recurrence of symptoms, but severity scores were still significantly better than pretreatment scores. Also, there was a relapse of total VHI and individual domain scores, however, still significantly better than pretreatment scores. The reduction of improvement observed in our cohort of PRP-treated patients at the 3-month visit suggests that monthly PRP injections may be needed for maintenance of improvement. Further research is useful to provide more insight regarding the number of injections needed to maintain the therapeutic effects and determine the maximal duration of therapeutic effect of PRP injections.
In our cohort of PRP-HA-treated females, an improvement of vaginal dryness, dyspareunia, and frequency of intercourse avoidance started similarly at 1 month. Aguilar et al.
34
similarly reported improvement of VVA and sexual symptoms in a 39-year-old female patient with vaginal laxity and vaginal mucosal atrophy following injection of purified fat cells and PRP-HA into the posterior vaginal wall and perineum. Hersant et al.
9
also reported efficiency of PRP-HA injections in reducing dyspareunia and vaginal dryness in menopausal women with a history of breast cancer in 100% of their studied patients
These findings support the effectiveness of combined PRP-HA in VVA induced by oncologic treatment. Evidence suggests that HA increases water retention and hydration, wound healing, angiogenesis, stimulates collagen synthesis, and increases the expression of CoL1A1 and CoL3A1 from dermal fibroblasts. 13 It also promotes epidermal keratinocyte proliferation. 35 Few histopathological studies reported evident histopathologic tissue changes in vulvar–vaginal atrophic tissue supporting its use in patients with VVA. 35
Our observed improvements of the total VHI score as well as fluid volume, pH, mucosal integrity, and moisture scores at 1 month following the first injection and that of elasticity at 2 months suggest a more gradual nature of extracellular matrix synthesis and collagen remodeling by PRP and HA. We suggest that PRP besides being regarded as a growth factor reserve can serve as delivery system in combination with other modalities. Combined PRP-HA takes advantage of moisturizing, wound healing, and the angiogenesis stimulation properties of HA in addition to the growth factor reserve of PRP and HA acting as a biomaterial scaffold. 9 Eppley et al. 36 suggested that hyaluronic acid (HA) potentiates PRP-stimulated wound healing, enhances the hydration of tissues, and facilitates the use of PRP by converting it into a more viscous solution. Combined PRP-HA can therefore be regarded an effective alternative for treatment of VVA in cancer patients.
Nevertheless, we observed partial recurrence of the mean VVA symptom scores in group B, but were still better than pretreatment mean scores at the 3-month follow-up. We also observed a reduction of total and individual domains of VHI scores at the follow-up visit at 3 months following the second injection. On the contrary, Hersant et al. 9 reported significant improvement of VHI total and domain scores up to 6 months after treatment with one session of intramucosal PRP-HA injections. The difference might be attributed to them injecting a larger volume of HA (2 mL). Furthermore, in their study, they mentioned inclusion criteria of cancer patients in remission after surgery only, with no details of types of cancer therapies used.
Berreni et al. 13 also reported a highly significant improvement of 75% of VHI persisting to 2 months after a single injection of sodium hyaluronate crosslinked interpenetrating polymer network such as 19 mg/g+mannitol (antioxidant). The high improvement and longer duration might be due to their choice of a longer lasting crosslinked filler and the added mannitol, which reduced filler breakdown. Furthermore, their study was conducted on menopausal women in contrast to our cancer patients who had received anticancer treatment with further compromise of vulvovaginal mucosa. Further research may help optimize treatment parameters in terms of injection interval, injected volumes, type of hyaluronic acid, and optimal number of injections required to maintain the therapeutic effect.
In group C, we observed an improvement of VVA symptomatology after 1 month of daily topical HA application. However, frequency of intercourse avoidance showed significant improvement later at 2 months. We suggest that the immediate effect of hydration by HA gel improved dryness and pain, but a longer duration of application was required for improvement of VVA and thereby improve frequency of intercourse. In agreement, Jonasson et al. 37 reported an insignificant reduction in avoidance of sexual activity at 4 weeks and further reduction after 12 weeks of therapy with topical HA water-based cellulose gel. This supports our observation that a longer duration of application of topical HA is required for greater improvement of frequency of avoidance. These findings support the role of HA-based preparations in improving hydration and clinical symptoms and signs related to VVA.
We reported that despite improvement of total VHI, pH, mucosal integrity, moisture, and fluid volume with topical HA, the vaginal elasticity domain showed no improvement with treatment at any of the visits. We believe that the large molecular size of HA in the gel does not allow it to cross the intact epithelium to the desired site 35 where it exerts its biological effects as an active signaling molecule, through interaction with proteoglycans or cell surface receptors to induce collagen and extracellular matrix synthesis. 12
All three symptoms showed recurrence to scores insignificantly different from pretreatment levels at the 3-month follow-up visit in group C. The total and individual VHI domain scores also recurred to nearly pretreatment values after 3 months of discontinuation of application. On the contrary, Jonasson et al. 37 reported a significant improvement of vaginal pH at 4 weeks and further improvement observed at 12 weeks after continuous HA daily application. Their opposing results suggest that a longer duration of application is required for maintenance of the results. Nappi et al. 38 reported that vaginal HA pessaries induced a significant improvement of VHI items (elasticity, fluid volume, pH, moisture, and epithelial integrity) at 3 months of treatment. Their results suggest that a longer duration of application or use of controlled release delivery as pessaries might be associated with improvement of elasticity.
To the best of our knowledge, this is the first study to compare the efficacy and tolerability of using PRP, PRP combined with noncrosslinked HA injections versus the standard HA gel treatment in VVA in patients with a history of cancer. Results of the mixed-effect model showed that combined PRP-HA-treated patients showed greater improvement of vaginal dryness compared with the topically treated group. This supports the add-on effect of noncrosslinked hyaluronic acid with its known water retaining properties . We also noted that both the PRP- and combined PRP-HA-treated groups had greater improvement of frequency of intercourse avoidance over the treatment visits than the topical HA-treated patients, which is mostly the result of better improvement of VVA and both can be regarded superior than topical HA in our cohort. We also reported that the PRP-treated patients had greater improvement of dyspareunia over the treatment visits compared with the topical HA-treated group mostly secondary to the PRP-induced neuronal growth and increased extracellular matrix synthesis and hence higher efficacy.
Furthermore, the therapeutic effect of improving VVA symptoms was lost 3 months after the end of treatment in opposition to the PRP and combined PRP-HA groups denoting a longer duration of effect. These suggest superiority of either PRP or combined PRP-HA injections compared with the conventional topical HA in improving symptomatology of VVA.
Our results also suggest that both PRP and combined PRP-HA are superior to topical HA regarding vaginal pH, fluid volume, and total VHI score improvement over time. Furthermore, the combined PRP-HA group showed a significantly higher improvement of moisture scores than group C emphasizing the importance of HA molecule in improving hydration and the synergistic effects of HA and PRP. Topical HA in opposition to the other two groups failed to induce any significant improvement of vaginal elasticity over the treatment visits. We suggest that topically applied HA cannot reach the submucosa easily and might require longer duration to elicit such effects, whereas injections of PRP alone or combined with HA help deliver the active molecule at the desired site of action.
We demonstrated that the improvement of the VHI (total and domain) scores was lost 3 months after the end of treatment with topical HA in opposition to the PRP and combined PRP-HA groups, denoting a longer duration of effect. The observed insignificant relapse in the PRP- and PRP-HA-treated females at the 3-month follow-up might be the result of the waning of short-acting noncrosslinked HA by 3 months and the probable need for repeated PRP injections to maintain the effect. We suggest that repeated injections of noncrosslinked HA or use of crosslinked longer acting HA preparations or increasing the number of PRP injections might be needed to achieve longer term effects. The topical HA-treated group showed a significant recurrence to pretreatment scores implying that continuous use might be needed to maintain the therapeutic effect.
Reported side effects in our study were injection-related pain and bleeding, which were regarded minor and self-limited. The pain severity and duration were significantly greater in the PRP-HA-treated group compared with the PRP-treated group at each of the treatment visits. This is probably due to the liquid nature of PRP compared with the more viscous PRP-HA combination accounting for the better tolerability of PRP injections. On the contrary, Park et al. 39 reported a case of hyaluronic acid pulmonary embolism. Their accident is probably secondary to use of a crosslinked HA as well as injection into the anterior vaginal wall with an extensive venous plexus. We avoided injection into the anterior vaginal wall. The topical HA-treated group reported no side effects signifying excellent tolerability.
Nappi et al. 12 and Jonasson et al. 37 demonstrated similarly excellent tolerability of the topical HA vaginal pessaries in 100% of their patients, re-enforcing the safety and tolerability of topical HA.
We demonstrated significantly higher patient-reported treatment satisfaction in groups A and B over group C. However, we reported no significance between the PRP and PRP-HA groups. This could be due to the better tolerability and hence high acceptability and satisfaction by the patients for PRP. With regard to the patient-reported sense of vaginal tightening, none of the topical HA-treated patients reported an improvement. Cynthia et al. 32 reported in a series of seven patients that patients observed a sensation of tightening of their vaginal tract after two sessions of PRP injections spaced 4 weeks apart. We suggest that the liquid characteristics of PRP compared with the more viscous PRP-HA gel allows PRP to flow more freely with a better and more even distribution into the tissues, which might explain the comparable tightening in both groups A and B.
Nevertheless, further studies are needed to clarify if more frequent injections of combined PRP-HA to prolong the action of noncrosslinked HA could offer advantage over PRP alone with regard to tightening.
The demonstrated improvement of vaginal dryness and moisture in the present study by PRP-HA suggests that the PRP-HA combination might be a more suitable modality for patients with VVA presenting mainly with decreased lubrication and with predominantly disturbed moisture parameter on the VHI scale. As PRP injections were associated with similar treatment satisfaction, and significantly lower injection-related pain severity and duration, it could be a good choice for patients presenting with dyspareunia or patients with mainly impaired pH and epithelial integrity domains of VHI scale. We believe though that increasing the number of injection sessions might be needed to evaluate any superiority of PRP-HA over PRP treatment injections for specific VVA symptoms or VHI parameters.
We conclude that submucosal injections of PRP and combined PRP with noncrosslinked HA are associated with comparable control of VVA symptomatology with a better tolerability and treatment satisfaction of PRP. Short-term topical HA is not associated with improvement of vaginal elasticity. Considering its easy application, feasibility, short-term efficacy, and safety, PRP represents a promising effective and safe modality of managing VVA in cancer patients.
Our findings are limited, however, by the duration of follow-up, which is needed to determine the maximal duration of therapeutic effects and optimum injection intervals. Due to the sample size of our study and the frequent use of combined anticancer treatment lines in our study sample, determining whether the treatment efficacy of PRP, PRP-HA, and topical HA varied in patients treated by different cancer management lines was not possible in this study. However, it is known that the VVA symptoms induced or aggravated by the different lines of cancer therapy all share a common pathogenesis, which is estrogen depletion. We also acknowledge the limitation of lack of device-based objective assessment of efficacy as biopsies were refused by the patients. Nevertheless, the VHI scoring is a widely used assessment score and was applied by a well-trained single gynecologist, who was blinded to the treatment used. To validate our results, we recommend further studies using more injection sessions of HA and PRP, different volumes of injection, and a longer follow-up to define the optimal strategy for touch-up treatments.
Data Access
The data sets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.
Ethics Approval
This study was performed in line with the principles of the Declaration of Helsinki. Approval was granted by the Ethics Committee of the Faculty of Medicine of University of Alexandria (Date 21-05-2020/No. 0201349).
Consent to Participate
Informed consent was obtained from all individual participants included in the study.
Consent to Publish
The authors affirm that human research participant provided informed consent for publication of the images in Figure 3a–c.
Footnotes
Authors' Contributions
S.S.O.: Conceptualization, methodology, data curation, writing—original draft, writing—review and editing, and supervision; K.F.E.: Conceptualization, writing—review and editing, and supervision; N.A.A.: Conceptualization, writing—review and editing, and supervision; A.A.B.: Conceptualization, writing—review and editing, and supervision; A.M.H.: Conceptualization, writing—review and editing, and supervision; L.A.H.: Conceptualization, writing—review and editing, supervision, and resources; E.N.R.: Conceptualization, writing—review and editing, investigation, and resources; W.O.A.: Conceptualization, writing—review and editing, and supervision.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.