
Abstract
Objective:
Findings from studies of the long-term effect of premature menopause on risks of all-cause mortality in women are equivocal. We used the approach of propensity score matching to examine the causal association of premature menopause with all-cause mortality and life span among women older than 40 years.
Methods:
The data were from the National Health and Nutrition Examination Survey I Epidemiologic Follow-up Study. We calculated the propensity score of premature menopause using a logistic regression model, then matched premature menopause with nonpremature menopause according to the score and the ratio of 1:1. We estimated mortality hazard ratios (HRs) and 95% confidence intervals (CIs) using Cox proportional hazard models. We also analyzed and plotted the relationship between age at menopause and reproductive life span with all-cause mortality and life span.
Results:
The mean age of 1,210 women was 55.4 ± 10.8 years at baseline. The unadjusted and adjusted HRs of all-cause mortality for women with premature menopause were 1.46 (95% CI: 1.08–1.96) and 1.53 (95% CI: 1.13–2.08), respectively, compared to nonpremature menopause. Nonlinear associations were found between age at menopause, reproductive life span, all-cause mortality, and life span. Menopausal age <37.5 years of age or reproductive life span <24 years increased the risk of all-cause mortality. Women with menopausal age <39 years of age or reproductive life span <24 years had a lower mean life span than the overall average of 76 years.
Conclusions:
Premature menopause significantly increased all-cause mortality risk and shortened life span in women. As women's age at menopause or reproductive life span increases, their overall life span also tends to increase.
Introduction
Women's menopause, defined as 12 months without menstruation, generally occurs between 49 and 52 years of age, and the median age of menopause is 51 years of age in the United States. 1 –3 Menopause is considered an indicator of reproductive and physical aging, subsequently bringing a series of health consequences. 4 Currently, ∼1% of women suffer from premature menopause, defined as the onset of menopause before the age of 40. 5
Previous studies reported that premature menopause could increase the risk of all-cause mortality in women, 6 –9 but not all research had consistent findings. 10 –12 The inconsistency in findings across studies may be attributed to variations in study designs and diverse adjustments for confounding factors. A recent meta-analysis of 16 studies, including 321,233 women, indicated that the hazard ratio (HR) for the association between premature menopause and all-cause mortality was 1.10 with a 95% confidence interval (CI) of 1.01 to 1.21. 4 Despite extensive studies, a clear consensus has not been achieved. 13 –15
There was less research on the relationship between premature menopause and life span in comparison to mortality, yet several studies yielded noteworthy findings. 16,17 A prospective study of 12,134 Dutch postmenopausal women with a mean age of 50 revealed that women who experienced menopause after 55 years of age had a life span that was longer by 2.0 years compared to those who underwent premature menopause. 16 However, a study conducted in Sweden found that the life span of 152 women who underwent bilateral salpingo-oophorectomy before the age of 30 years in the late 1930s did not significantly differ from national statistics about contemporary women (74.8 vs. 74.7 years of age). The researchers concluded that, while early loss of female sex hormones might impact morbidity and mortality patterns, it did not have any significant effect on overall life span. 17
Few studies demonstrated the association of premature menopause with all-cause mortality and life span using causal inference analysis such as the propensity score matching (PSM) approach. PSM is a simulated experimental method in observational studies, in which researchers utilize statistical techniques to match each exposed subject with an unexposed subject with similar characteristics to create a matched cohort. 18 This technique can facilitate the creation of new datasets based on the original data from observational studies through matching, where the distribution of covariates at different exposure levels can be as balanced as possible. This can mitigate bias and enhance comparability across different exposure groups. The effect of exposure or intervention on outcomes is then estimated based on the matched cohort.
Therefore, we aimed to demonstrate the association of premature menopause with all-cause mortality and life span using PSM analysis. We hypothesized that premature menopause would lead to higher risks of all-cause mortality and shorter life span in women older than 40 years in later life.
Materials and Methods
Data source and study population
This study used data from the National Health and Nutrition Examination Survey I Epidemiologic Follow-up Study (NHEFS), a stratified, multistage probability sampling design to investigate the health and nutritional status of American civilians. 19 NHEFS included NHANES I baseline in 1971–1974 and three follow-up visits in 1982–1984, 1987, and 1992, respectively. The baseline survey involved nutritional and health screening with interviews, medical examinations, and laboratory tests for different subgroups. Follow-up visits included data collection by interview and measurement of pulse rate, blood pressure, and weight.
The Institutional Review Board of the National Center for Health Statistics approved the survey and received written consent from the participants. There were 14,407 adult participants 25–74 years of age in the NHEFS baseline survey of 1971–1974. Our study population included female participants who were older than 40 years at the baseline, excluding those who had been diagnosed with any cancer before premature menopause. The study sample included 5,153 women, 605 women with premature menopause and 4,548 with nonpremature menopause.
Exposure and outcome variables
Premature menopause, the exposure variable, was defined as menopause before the age of 40. 20,21 The history of premature menopause was determined by responses to two questions, including “Have you entirely stopped menstrual?,” and “How old were you when entirely stopping menstrual?.” Those with menopausal age younger than 40 years were identified as the premature menopause group, otherwise the nonpremature menopause group. In addition, age at menopause and reproductive life span as continuous variables were used to examine the associations with outcome variables. Age at menopause referred to the age at which menstruation stopped completely. Reproductive life span was the difference between age at menopause and age at menarche, measured in years. 11 Age at menarche was obtained through the question “How old were you when your periods or menstrual cycle started?.”
The outcome variable was death from any cause or all-cause mortality. NHEFS follow-up data covered information about health and survival status. Subjects' death status was assessed through proxy interviews and death certificates. 19,22 We also investigated life span as an outcome variable, which refers to the duration of a participant's life from birth until death. 23
Covariates
Covariates included age, race, marital status, education, body mass index (BMI), smoking, alcohol use, physical activity, hypertension, diabetes mellitus, age at menarche, number of miscarriages/abortions/stillbirths, number of live births, history of hysterectomy, history of bilateral oophorectomy, and taking female hormones. Age, BMI, age at menarche, number of miscarriages/abortions/stillbirths, and number of live births were continuous variables in the analysis. Race, education, age at menarche, number of live births, and number of abortions/miscarriages/stillbirths were fixed covariates, while other covariates were time varying.
Race was classified as white or other because white accounted for ∼80% of this study. Education levels included high school or below and at least some college/university or above. Marital status was grouped as married and others. Smoking was categorized into three groups, current, former, and never. Alcohol drinking was based on the question “Have you had beer/wine/liquor at least 12 times during the past year?.” Physical activity was determined according to the question “Do you get regular exercise in your usual day?.”
We defined hypertension based on the question, “Did a doctor tell you have high blood pressure?,” “Are you taking a prescription for hypertension?,” or the average systolic blood pressure was ≥140 mmHg or the average diastolic blood pressure was ≥90 mmHg. Diabetes mellitus was identified by the question, “Did a doctor tell you have diabetes?” and “Are you taking antidiabetic medication/insulin?.” Taking female hormones was based on the question, “Have you ever continuously taken hormones?.” The history of hysterectomy or bilateral oophorectomy was self-reported by participants in interviews.
Statistical analysis
We calculated propensity scores for each participant through a multivariate logistic regression model, with premature menopause as the outcome variable and the covariates listed in Table 1 serving as the independent variables. Then we matched participants in the premature menopause group to those in the nonpremature menopause group according to the propensity scores and ratio of 1:1. In this process, we attempted different matching methods of nearest neighbor matching, replacement matching, and optimal matching.
Baseline Characteristics by Premature Menopause Before and After Propensity Score Matching
Denotes continuous variables described by mean ± SD, while others are categorical variables presented by frequency (percentage). Alcohol drinking: Had at least 12 times for beer/wine/liquor during the past year.
Number of AMS = Number of abortions/miscarriages/stillbirths.
BMI, body mass index; PSM, propensity score matching.
The selection of an appropriate caliper width is also crucial when performing the matching. This parameter sets the threshold range for determining the similarity of samples based on their respective propensity scores. 24 Typically, diverse caliper width options are used in various surveys to identify the optimal one. 25,26 In accordance with the relevant references and the actual situation of our sample, 24 we performed experiments with alternative caliper widths of 0.2, 0.3, and 0.4. Ultimately, we opted for the nearest-neighbor matching algorithm with a caliper width of 0.3 without replacement as it produced the most balanced distribution of propensity scores between both groups. The final matched cohort included 605 women with premature menopause and 605 women with nonpremature menopause.
We described baseline characteristics using mean ± standard deviation for continuous variables and frequency (proportions) for categorical variables. The chi-square test was used to compare the proportions between the two groups. t-Tests were used to compare the mean of continuous variables between the two groups. We utilized Kaplan-Meier curves to estimate survival probability, in which the log-rank tests were used to judge differences in the survival probability of the two groups.
We applied Cox proportional hazards models to estimate HRs and 95% CI of all-cause mortality for premature menopause compared to nonpremature menopause. In the matched cohort, we constructed both the unadjusted model and the adjusted model by incorporating potential confounders listed in Table 1. Moreover, we used Cox proportional hazards regression model with penalized spline to estimate HRs and 95% CI for the association of age at menopause and reproductive life span as continuous variables with all-cause mortality. 27
Also, we utilized nonparametric regression with smoothing splines to graphically show the relationship between age at menopause and reproductive life span and life span. 28 –30 This approach enables estimation of the mean life span for a given age at menopause/reproductive life span, while remaining agnostic to the function between outcome and predictor variables, thereby avoiding misspecification errors.
To obtain a comprehensive understanding of the association between premature menopause, all-cause mortality, and potential effect modifiers, we investigated the multiplicative interactions of premature menopause with age, race, hysterectomy, bilateral oophorectomy, and taking female hormones based on prior studies. 5,6,20,31 Briefly, we explored the interactions between premature menopause and age, race, hysterectomy, and bilateral oophorectomy to elucidate disparities in the impact of premature menopause on all-cause mortality across specific populations. In addition, we examined the interplay between premature menopause and taking female hormones to assess its moderating effect on all-cause mortality risk.
We conducted sensitivity analysis for another matching method of optional matching with a caliper width of 0.3. We also attempted sensitivity analysis after removing the covariate of age at menarche when matching the cohort and building the Cox proportional hazard models. All statistical analyses were carried out using SAS version 9.4 (SAS Institute, Inc., Cary, NC) and R software (version 4.3.0). The statistical significance was identified at two-tailed p-values <0.05. The PSM analysis was conducted using the SAS proc psmatch program. We utilized the R packages “survival,” “smoothHR,” and “splines” to perform Cox proportional hazards regression analysis with penalized splines, as well as the “npreg” package for nonparametric regression using smoothing splines.
Results
Basic characteristics of the study population
The matched cohort consisted of 1,210 women with a mean age of 55.4 + 10.8 years. Before PSM, there were statistically significant differences in the proportions of race, education, smoke, hysterectomy, bilateral oophorectomy, and taking female hormones, and in the mean of age, age at menarche, and the number of live births between premature menopause and nonpremature menopause group. After PSM, there was no significant difference in any covariate between the two groups (Table 1). Figure 1 visualizes the standardized mean difference in the covariates before and after propensity scores for women with and without premature menopause.
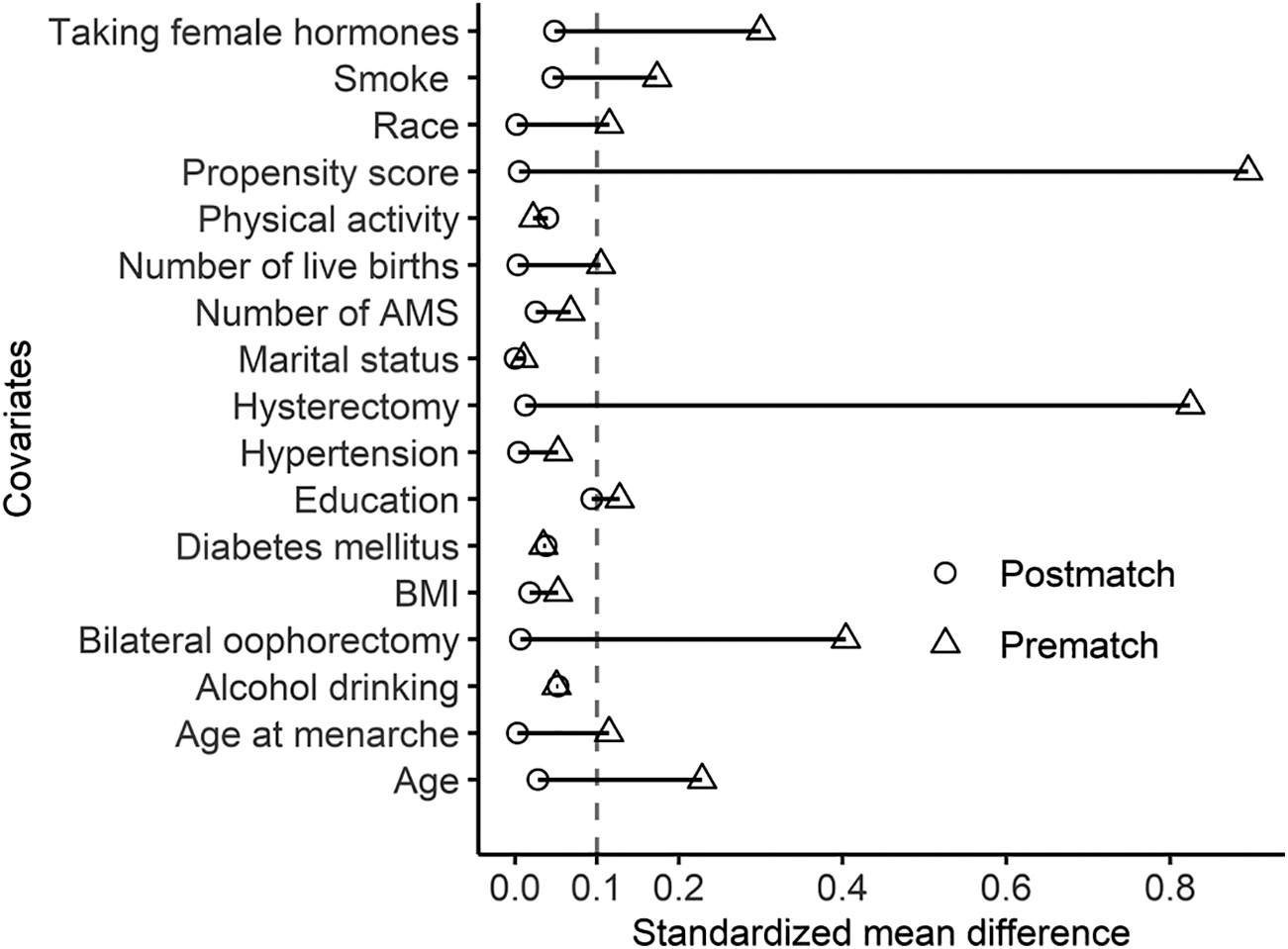
Standardized mean difference in covariates before and after propensity score for women with and without premature menopause.
Association between premature menopause and all-cause mortality
Kaplan-Meier curves show that premature menopause was positively associated with the cumulative incidence of all-cause death in the matched cohort (p < 0.05) (Fig. 2). The HR for the association between premature menopause and all-cause mortality was 1.46 (95% CI: 1.08–1.96) compared to nonpremature menopause in the matched cohort. After adjusting for the covariates in Table 1, the adjusted HR (aHR) was 1.53 (95% CI: 1.13–2.08). In addition, each additional year in age at menopause or reproductive life span could reduce risks of all-cause mortality by 4% (aHR: 0.96, 95% CI: 0.94–0.98), controlling for potential confounders (Table 2).

Kaplan-Meier Curve for all-cause death among women older than 40 years in the matched cohort.
Hazard Ratios for the Association of Premature Menopause with All-Cause Mortality in the Matched Cohort
Adjusted for the covariates in Table 1.
CI, confidence interval; HR, hazard ratio.
Comparison of life span between two groups
In the matched cohort, 386 participants died by the end of follow-up in 1992, with a mean life span of 76.0 ± 9.8 years. The mean life span for premature and nonpremature menopause groups was 75.2 ± 10.0 and 76.9 ± 9.5 years, respectively (p = 0.0386). Figure 3 illustrates the distribution of deceased participants' life span in each group, displaying median life span ± interquartile range (IQR) of 77 ± 12 and 80 ± 14 years in the two groups(p = 0.0108). The violin plot indicates that the highest probability in premature and nonpremature menopause groups corresponds to the life span of 77 and 83 years, respectively. The area below the dotted line denotes the proportion of participants with a life span less than 60 years in each group, which is 11% for those undergoing premature menopause and 5.6% in the nonpremature menopause group.
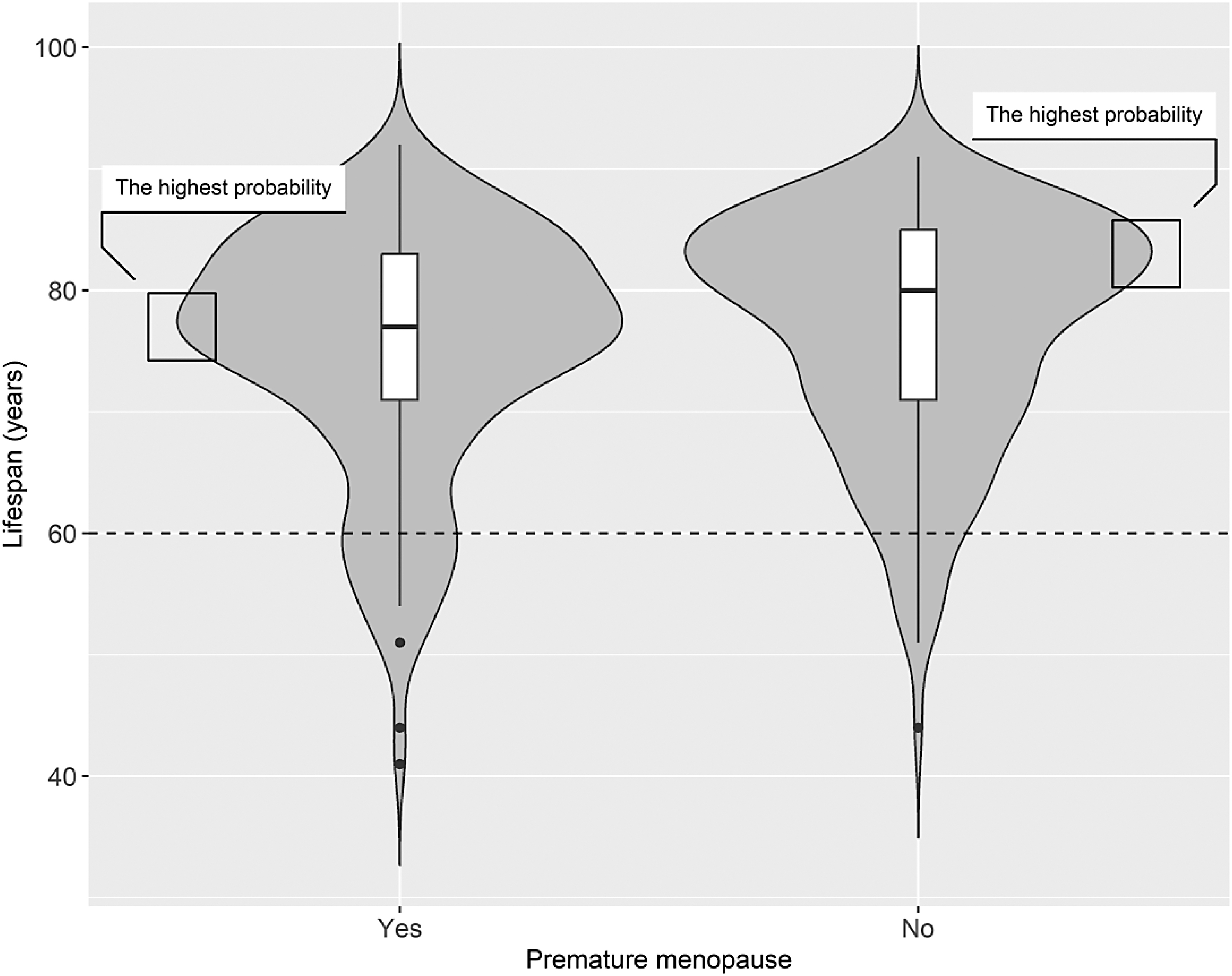
Violin plot for the distribution of the life span by premature menopause in the 386 dead participants of the matched cohort. It exhibits the kernel density estimates of the data distribution through its outermost symmetric curves. The top and bottom lines of the central box represent the first and third quartiles, respectively, while the bold black line in the center depicts the median life span. The vertical black line extends from the low adjacent value (first quartile −1.5 interquartile range) to the high adjacent value (third quartile +1.5 interquartile range), with outliers represented by black dots. The highest probability in premature and nonpremature menopause groups corresponds to 77 and 83 years, respectively. The area below the dotted line denotes the proportion of deceased participants with a life span of fewer than 60 years in each group, which is 11% for those experiencing premature menopause and 5.6% for the nonpremature menopause group.
Association of age at menopause and reproductive life span with all-cause mortality
Figure 4 illustrates the nonlinear association of age at menopause and reproductive life span with all-cause mortality in the matched cohort of 1,210 women. Women who experienced menopause before 37.5 years of age or had a reproductive life span shorter than 24 years were at significantly higher risk for all-cause mortality, whereas those with menopause occurring between 45.5 and 53 years of age or reproductive life span of 30.5 to 39 years exhibited reduced risks.
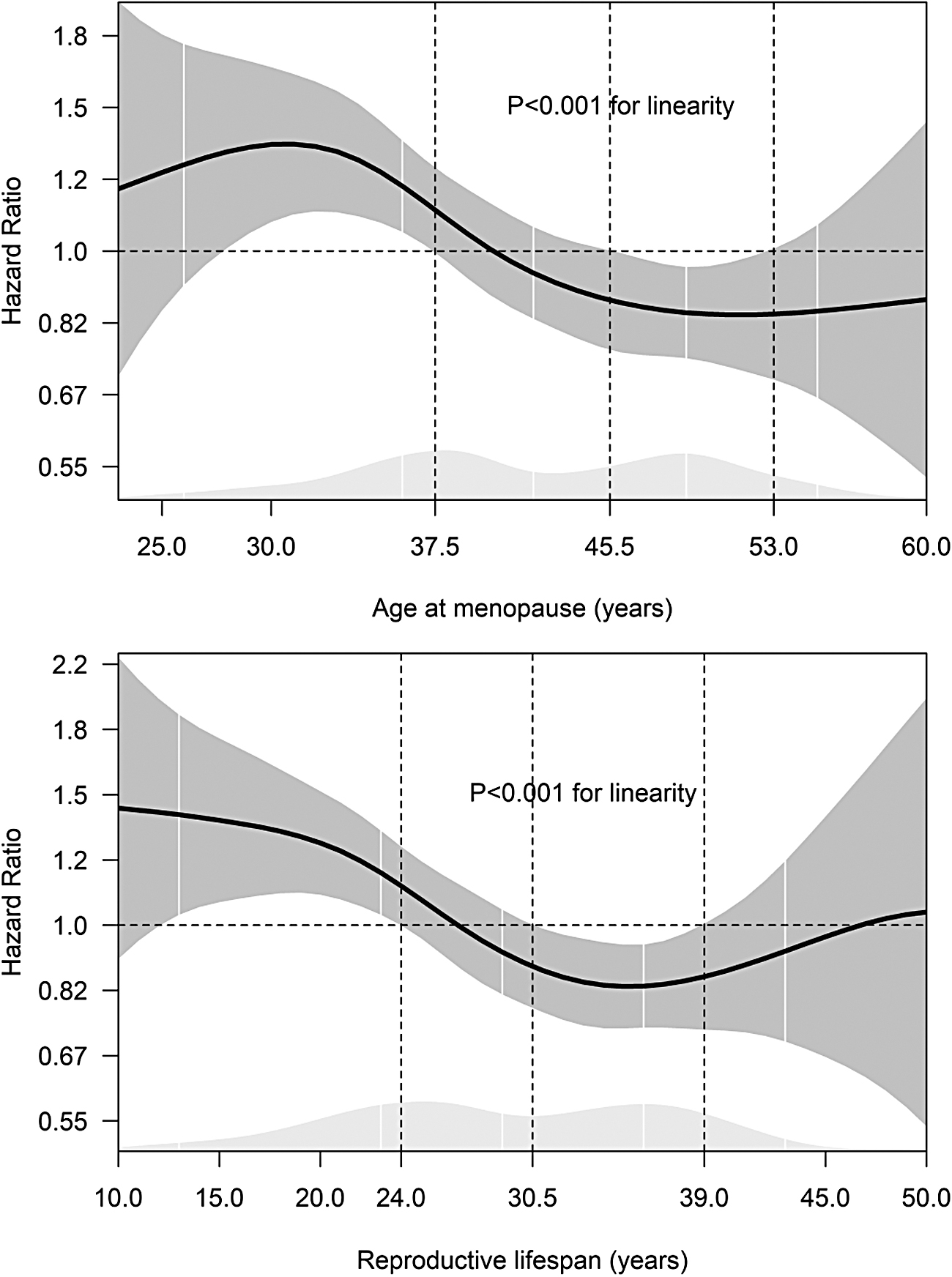
The HRs and 95% CI for the association of age at menopause and reproductive life span with the risk of all-cause mortality among 1,210 women older than 40 years in the matched cohort. The dark gray shaded area represents the HRs and 95% CIs, with the dashed line set to 1.0 as a benchmark. The vertical dashed line on the left points out that age at menopause <37.5 years of age or reproductive life span <24 years significantly increased the risk of all-cause mortality. The vertical dashed line on the right-hand side shows that menopausal age of 45.5–53 years or reproductive life span of 30.5–39 years was associated with reduced risks of all-cause mortality. The light gray plot at the bottom shows the distribution of age at menopause or reproductive life span among the 1,210 participants, where the white vertical lines represent the percentiles at 5th, 25th, 50th, 75th, and 95th percentiles from left to right. CI, confidence interval; HRs, hazard ratios.
Relationship between life span and age at menopause and reproductive life span
Figure 5 exhibits the relationship between life span and age at menopause and reproductive life span in 386 deceased participants. Overall, life span was positively correlated with the extension of age at menopause or reproductive life span. The mean life span of women with menopause at <39 years of age or reproductive life span <24 years was significantly lower than the overall average life span of 76 years, whereas those with menopause at >49 years of age or reproductive life span >35 years had a significantly greater mean life span exceeding 76 years.
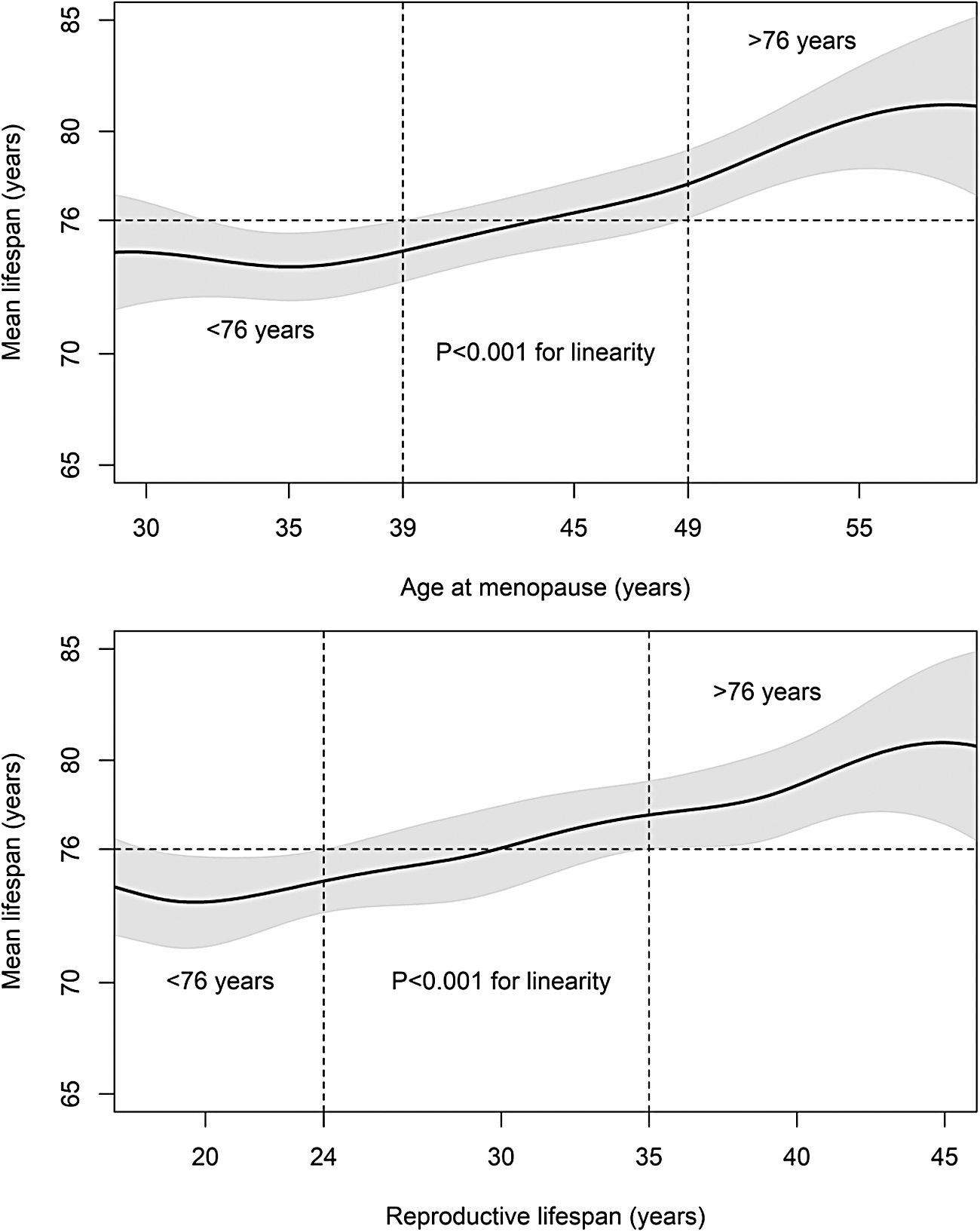
The estimated mean life span and 95% CI based on age at menopause and reproductive life span of 386 deceased participants in the matched cohort. The horizontal dashed reference line represents the overall average life span (76 years) in the 386 dead participants. The left vertical dashed line displays those participants with menopause at <39 years of age or reproductive life span <24 years had significantly lower mean life span than 76 years. The right vertical dashed line indicates that the mean life span in participants with menopause at >49 years of age or reproductive life span >35 years was higher than 76 years.
Subgroup analysis and sensitivity analysis
Results from the stratified analysis showed no significant interaction between premature menopause by age, race, hysterectomy, bilateral oophorectomy, and taking female hormones according to the statistical criteria of p < 0.05 (Supplementary Fig. S1). The sensitivity analysis results for the alternative method of optimal matching showed similar aHRs to this analysis, not changing the overall explanation. In addition, the sensitivity analysis based on the matched cohort of removing the covariate of age at menarche demonstrated similar results (Table 2).
Discussion
We demonstrated the significant association between premature menopause and increased risk of all-cause mortality, as well as reduced life span compared to nonmenopausal women in the matched cohort. Age at menopause and reproductive life span exhibited nonlinear associations with all-cause mortality and longevity when treated as continuous variables. Menopausal at <37.5 years of age or reproductive life span <24 years increased the risk of all-cause mortality. Women with menopause at <39 years of age or reproductive life span <24 years had a lower mean life span than the overall average of 76 years. Conversely, women with menopause at 45.5–53 years of age and reproductive life span of 30.5–39 years benefited from reduced risk for all-cause mortality.
Our findings demonstrated that relative to the nonpremature menopause group, premature menopause was associated with a 53% increased risk of mortality and a reduction in the average life span of 1.7 years. A prospective study with 9.2 years of follow-up of 4,683 Japanese women found a similar risk of mortality in women with premature menopause of 2.1 times compared to those with menopausal age of 45–49 years. 6 Conversely, the Health, Well-Being, and Aging study from Brazil indicated that premature menopause was insignificantly associated with all-cause mortality in 1,265 women with a median age of 71 years compared to age at menopause of 50–54 years. 32 Also, Jacobsen et al. in a cohort study with 37 years of follow-up did not observe a significant association of premature menopause with mortality in Norwegian postmenopausal women relative to menopausal age of 50–52 years. 33
The study of 16,251 women in the Women's Health Initiative reported that later age at menopause could increase the probability of surviving to 90 years regardless of natural or surgical menopause compared to premature menopause. 8 With one accord, another prospective study of more than 12,000 females with a mean age of 50 years in Dutch found each additional year of age at menopause was associated with a 2% lower risk of all-cause mortality, despite natural or surgical. 34 This also kept in line with our findings that a 4% decrease in risk of all-cause mortality for every year increase in age at menopause (Table 2).
We observed nonlinear associations between age at menopause and mortality, whereby menopause occurring before 37.5 years of age was associated with increased risks of all-cause mortality, while menopause at 45.5–53 years of age was linked to low risks of all-cause mortality (Fig. 4). However, Cooper and Sandler found no association of age at menopause with all-cause mortality after controlling for potential confounders among more than 3,000 women 50–86 years of age. 10 The Iowa Elderly Cohort study of 1,684 women ≥65 years of age also observed that age at menopause was not associated with an increased risk of all-cause mortality, regardless of the type of menopause after adjusting for potential confounders. 12
In addition, our findings suggested that increasing age at menopause was positively related to increased life span, where women with menopause before 39 years of age had a lower average life span, while those after 49 years of age had a higher one, compared to the overall average life span. This was in line with the findings of some studies. For example, a population-based prospective study of 3,650 postmenopausal women older than 45 years of age revealed that those with age at menopause ≤44 years had a reduced life expectancy by 3.1 years compared to those with menopause age between 45–54 years and by 3.5 years compared to those with menopause age ≥55 years. 31 Similarly, Ossewaarde et al. reported that life span in women with menopausal age over 55 years was extended by 2.0 years compared to those undergoing menopause below the age of 40 years. 16
Increasing studies reported the relationship between reproductive life span and mortality; however, there was no consistent evidence to draw conclusions about the associations. 34 Our results overall showed that a reproductive life span <24 years resulted in shorter average life span, while a reproductive life span >35 years was inversely proportional to life span. In line with our results, Shadyab et al. reported that women with reproductive life ≥33 years were 13% more likely to survive to 90 years of age than women with reproductive life <33 years. 8
Inconsistently, some researchers reported that reproductive life span increased the risk of all-mortality. 11,35 For example, a prospective cohort study of ∼4,000 women ≥55 years of age from the Netherlands found that every year increase in reproductive life span could elevate 2% risk of all-cause mortality after controlling for confounders (HR: 1.02, 95% CI: 1.00–1.05). The authors concluded that longer reproductive life span and estrogen exposure were harmful to all-cause and cardiovascular disease (CVD) mortality. 11
The pathways by which premature menopause was associated with mortality risk and life span are not yet fully disentangled. 8,36 Shuster et al. explained that this association may be due to comorbidities and poor health in women with premature menopause, resulting in increased mortality and reduced life span. 37 It is well known that reproductive life span is the difference between age at menopause and age at menarche, indirectly representing estrogen exposure. 38
Some researchers claimed that late menopausal age and a lengthy reproductive life span that ensured long-term exposure to endogenous estrogen had a cardioprotective effect on women, thereby reducing the risk of all-cause and CVD mortality. 39,40 However, this interpretation remains currently controversial, with some findings that estrogen replacement led to increased risks of adverse CVD events and breast cancer among postmenopausal women. 41,42 Besides, a genome-wide study found that age at menopause was associated with genetic variants related to DNA replication and repair pathways that are central to aging. 43 Nebel et al. reported that DNA repair gene exonuclease 1 was related to age at menopause and longevity in women. 44
Our study's strengths included applying PSM analysis, which reduced confounding bias. To our knowledge, few research used causal inference technology to investigate the association between premature menopause and all-cause mortality. Besides, based on the matched cohort, we also conducted comprehensive analysis for the associations of age at menopause and reproductive age with all-cause mortality and life span when treated as continuous variables, and we performed subgroup analysis and sensitivity analysis to verify the robustness and stability of the results.
Regarding the limitations of this study, the sample size of female participants with premature menopause was only 605 due to the low prevalence rate of 1%. As a result, we were unable to further categorize premature menopause into natural and surgical types, nor could we effectively stratify surgical premature menopause based on hysterectomy type (hysterectomy alone or hysterectomy with single oophorectomy or bilateral oophorectomy). Besides, most variables were collected through self-reported interviews, which might introduce bias. In addition, the database covered the years 1971–1992, representing slightly earlier years. However, analyzing earlier sample data allowed us to observe death occurrences and analyze life span among deceased participants. Therefore, we believe that these results have significant research value, particularly for women in the United States.
Conclusion
We utilized the causal inference approach of PSM to examine the association of premature menopause with all-cause mortality and life span in women older than 40 years in the United States. We found that premature menopause enhanced risks of all-cause mortality and shortened life span in women. When considered continuous variables, both age at menopause and reproductive life span exhibited nonlinear association with all-cause mortality and life span. Age at menopause below 37.5 years of age or reproductive life span less than 24 years significantly increased the risk of all-cause mortality. As women's age at menopause or reproductive life span increases, their overall life span also tends to increase. More extensive causal inference studies with contemporary and sizable sample sizes are imperative to authenticate our findings.
Footnotes
Acknowledgments
We are grateful to the Centers for Diseases Control and Prevention, United States, for providing the National Health and Nutrition Examination Survey I Epidemiologic Follow-up Study data for this study.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.
Supplementary Material
Supplementary Figure S1
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.