
Abstract
Background:
This study determined the prevalence of bothersome menstrual symptoms and their association with workability in naturally menstruating women not using hormonal contraception.
Materials and Methods:
A representative sample of community-dwelling Australian women aged 18–39 years selected from two large national electronic databases responded to a survey on general health. This study focuses on self-reported dysmenorrhea and menstrual bleeding and their association with workability and absenteeism in working women, assessed by the Workability Index.
Results:
Of 3,555 women, 1,573 (44.2% [95% CI: 42.6%–45.9%]) reported moderate to severe dysmenorrhea and 774 (21.8% [95% CI: 20.4%–23.2%]) reported heavy to very heavy bleeding. Women with dysmenorrhea were 50% more likely to report poorer work performance and twice as likely to report more days of sick leave in the past year (absenteeism) than other women.
Conclusions:
Despite the availability of safe and effective management options, Australian working women aged 18–39 years continue to experience bothersome dysmenorrhea and menstrual bleeding. Dysmenorrhea is associated with increased absenteeism and poorer workability. Therefore, awareness needs to be raised among women and health care providers of ways to manage dysmenorrhea and heavy bleeding and the unmet need for intervention in the community, respectively.
Introduction
Severe menstrual pain (dysmenorrhea) and heavy bleeding are associated with impaired quality of life and absenteeism. 1 Almost half of participants in a survey in the United States reported absenteeism (5.8 days on average in the previous year) and reported not receiving any support from their manager. 2 While there is increasing recognition of the need to have menstrual policies in the workplace for reproductive-aged women, there is no formal requirement for this in Australia. Endometriosis, a common cause of dysmenorrhea, is associated with significant absenteeism and presenteeism, when an individual is physically present at work but it is not fully functioning, at the workplace. 3
A systematic review of 21,573 young women under 25 years published in 2019 reported an overall estimate of dysmenorrhea prevalence of 71%. However, due to the heterogeneity of studies in the way they defined or measured the severity of dysmenorrhea the authors were unable to report the prevalence of moderate to severe dysmenorrhea. 4 A subsequent nation-wide survey in Australia in 4,202 women aged 13–25 years reported a prevalence of 89% of moderate to severe dysmenorrhea and an association with increased absenteeism and reduced classroom performance. 5 In terms of the impact of menstrual symptoms, including dysmenorrhea, a Dutch survey of women aged 14–45 years reported that 80% of the respondents had reduced work productivity due to menstrual-related symptoms with a median loss of 4.8 days per year due to presenteeism. 1 Nonetheless, these studies recruited women via social media and were specifically about menstrual symptoms, which means that women with more severe pain might have been attracted to these studies. 1,5
Hence, interpretation of findings is likely limited by selection bias. Furthermore, previous studies included women who were using oral contraceptive pills (OCPs) which are widely known to reduce menstrual pain and bleeding. This factor might have potentially impacted the prevalence and severity of dysmenorrhea in these studies. 1,5,6 Of note, more than half of OCP users in the study on “the menstrual health literacy management strategies in young women in Australia” reported reducing dysmenorrhea as the main reason for using OCPs. 7
There is a need for a greater understanding of the prevalence of bothersome menstrual symptoms and their impact on women's workability. The Grollo-Ruzzene Study (GR Study) was a cross-sectional study of physical and psychological well-being of Australian community-dwelling women aged 18–39 years. 8 The GR Study recruited a representative sample of 6,986 women, all of who completed a general health survey, minimizing selection bias. Thus, the GR study provides a unique opportunity to determine the prevalence of self-reported menstrual symptoms (specifically moderate to severe dysmenorrhea and heavy menstrual bleeding) in the community, the association of these symptoms with self-assessed workability, and hence, the burden menstrual symptoms places on women in the workforce.
Materials and Methods
Study design and participants
The GR Study was a population-based, cross-sectional survey conducted between November 11, 2016 and July 21, 2017 in Australia. Participants were nonhealth care seeking women aged 18–39 years who lived in the eastern Australia states of Victoria, Queensland, and New South Wales. The recruitment procedures are described in detail elsewhere. 8 Briefly, potential participants listed on two large national electronic databases were invited via email to join the study. Women were only excluded if they could not understand English sufficiently to complete the questionnaire. The participants resembled Australian women aged 18–39 years in key demographic characteristics, including age and geographic distribution, country of birth, education, partnership status, and occupation. 8
As our interest was in the impact of menstrual disorders on workability, participants were included in this analysis if they had ever menstruated, were not currently or recently pregnant, breast feeding, using assisted reproduction, had a surgical menopause, or had premature ovarian insufficiency. Women who were current users of combined oral contraceptives (COCs), injectables, implants, or concurrent long-acting reversible contraceptive (LARC/injectable and COC) were also excluded (Fig. 1). The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) checklist was used to prepare this article. 9
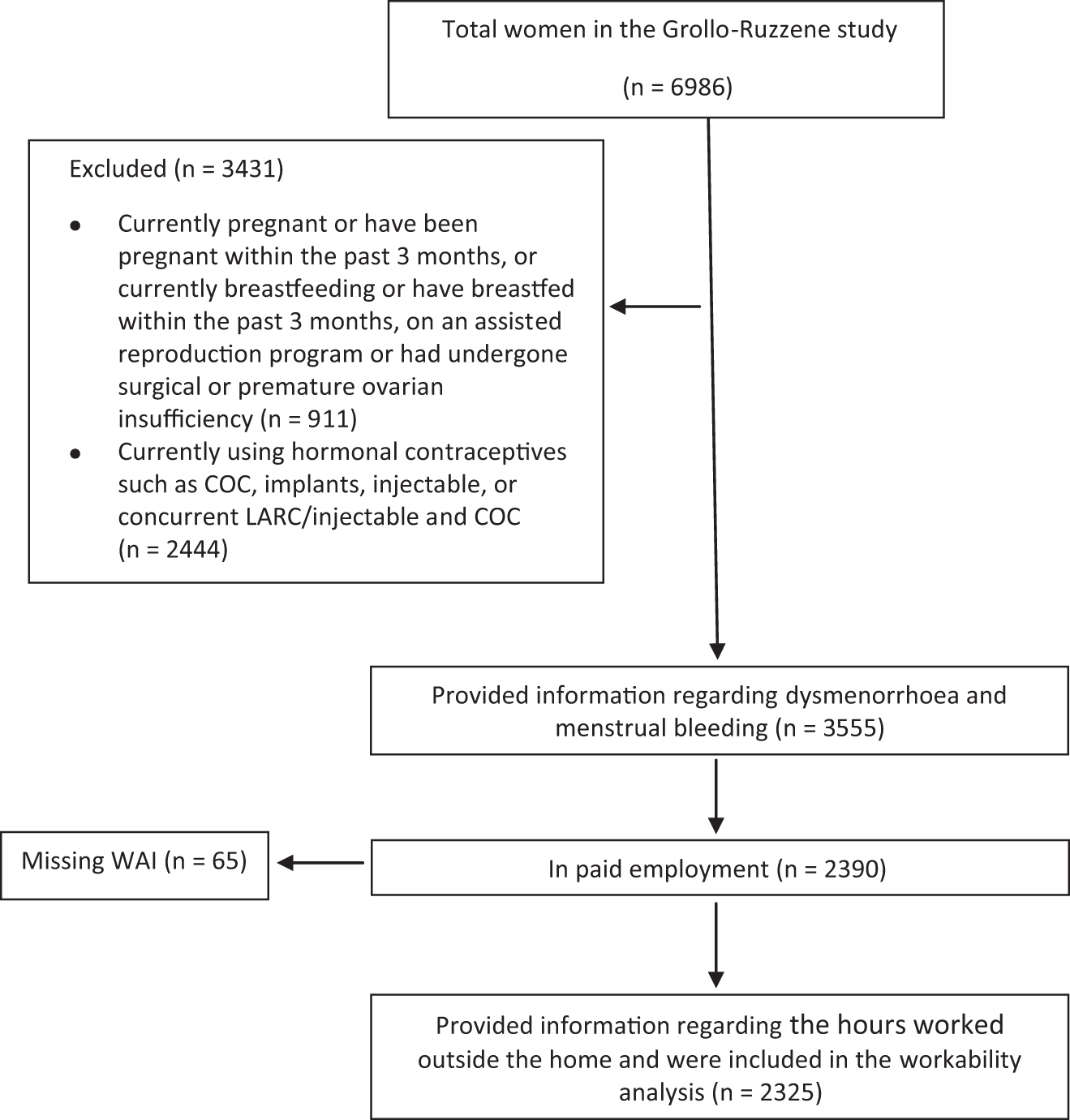
Flowchart of the study. COC, combined oral contraceptive; LARC, long-acting reversible contraceptives that is, implants and the intrauterine system (IUS) and injectables; WAI, workability index.
Assessment of dysmenorrhea and menstrual bleeding
Participants responded to a series of online questions, including age of menarche and menstrual profile. To assess dysmenorrhea, participants were asked if they had period pain and if so, how much it bothered them (not at all, somewhat, moderately, or severely). Dysmenorrhea was later dichotomized as not at all/somewhat dysmenorrhea or moderate/severe. The menstrual bleeding questions were preceded with advice that “bleeding” meant needing to use a tampon or sanitary pad, not discharge (spotting) for which only a panty-liner was required. “Days between periods” (interval) was defined as days from the first day of one menstrual bleed to the first day of the next menstrual bleed (21 days or less, 22–35 days, more than 35 days, or too irregular to say).
Further questions included duration of their menstrual bleeding (less than 7 days, 7–10 days, or more than 10 days). Women were asked to indicate how heavy their menstrual bleeds were on a scale of 1–6, with descriptors provided. For 1, light bleeding the descriptor was “on the heaviest day of bleeding I only need to change my pad or tampon every 4 hours or more” and for 6, heavy or very heavy bleeding, “I experience clotting, ‘flooding’, and need to use double protection and have to change at least every 2 hours.” Women were also asked how many days the bleeding was heavy (never, 2 days or less, 3–7 days, and more than 7 days). For the analysis, we combined the scores 5 (heavy bleeding) and 6 (very heavy bleeding with clotting) and light to moderate (scores 1–4).
Assessment of workability
Participants who reported working outside home were asked to report hours of work. Women were presented with a list of 17 different occupations, including the option to select “other” if their occupation was not included.
The self-reported workability was determined by the workability Index 10 which covers seven domains: current workability compared with best of lifetime, workability in relation to job demand, number of current diseases diagnosed by a physician, estimated work impairment due to disease, sickness absence during the past 12 months, own prognosis of workability 2 years from now, and mental resources of the worker's life in general, both at work and during leisure time. The total score ranges from 7 to 49 points, with a score of 44 to 49 indicating “excellent,” 37 to 43 “good,” 28 to 36 “moderate,” and 7 to 27 “poor” workability. The workability was further categorized as either poor to moderate (scores 7 to 36) or good to excellent (scores 37–49). For absence from work, participants were asked to choose one of the categories of 100–365, 25–99, 10–24, 9 days or less, or none for the number of days of sick leave over the past year. 10 We dichotomized sick leave in the past year to either 0–9 days or 10 or more days.
Sociodemographic factors
Sociodemographic variables included age, place of residence, ethnicity, relationship status, parity, smoking status, alcohol consumption, student status (full-time or part-time), caregiving responsibilities for another person, and housing insecurity. The body mass index (BMI) was calculated using self-reported height and weight.
Statistical analysis
Categorical and numerical data are described using frequency (%) and median (interquartile range; IQR), respectively. A 95% confidence interval (CI) is reported for the prevalence of moderate to severe dysmenorrhea and heavy to very heavy bleeding. The association between moderate to severe dysmenorrhea and menstrual bleeding was examined using Chi squared test. The univariate logistic regression was performed to examine the likelihood of having poor to moderate workability versus good to excellent workability between women with moderate to severe dysmenorrhea and no/somewhat dysmenorrhea. Similarly, univariate logistic regression was performed to examine the likelihood of 10 or more days of sick leave versus 0–9 days between women with moderate to severe dysmenorrhea and no/somewhat dysmenorrhea.
Model 1 assessed an unadjusted association between dysmenorrhea and workability and dysmenorrhea and absence from work in the last year. Model 2 included dysmenorrhea and controlled for sociodemographic factors, including age (<30 or ≥30), BMI, relationship status, smoking status, parity (nulliparous vs parous), housing insecurity, and being a carer. 11 The sociodemographic factors included in model 2 were chosen based on our previous work on menopausal vasomotor symptoms and workability 11 and whether the result of univariate logistic regression analysis for a variable gave a p-value of p ≤ 0.1. Model 3 incorporated the variables from model 2, as well as menstrual bleeding. An α level was set at 0.05. Analyses were performed using Stata Software V.16 (Stata Corporation, College Station, TX).
Sample size
The original sample size of 7,000 women of the GR study was based on the prevalence of polycystic ovary syndrome as the main outcome being 10%, with a margin of error of ±2%. This provided us with adequate sample to perform multivariate logistic regression following the rule of maintaining a ratio of 10 observations per variable included in a regression analysis. 12
Ethical considerations
The recruitment process commenced after receiving ethical approval from the Monash University Human Research Ethics Committee (CF16/2322-2016001166 [7703]), and all participants provided informed consent. Deidentified data were collected and stored under the Data Protection and Privacy Procedure of the Monash University. All authors share responsibility and accountability for the results.
Results
Participant characteristics
In total, 6,986 women completed the GR Study survey, and 3,555 women were asked about menstrual pain and bleeding (Fig. 1). Of these 3,555 women, 2,413 (67.9%) were of European ancestry, 1,627 (45.9%) were overweight or had obesity, 1,712 (48.3%) were married/defacto, 1,284 (36.1%) were parous, and 2,390 (67.2%) were currently working full-time or part-time (Table 1). Seventy-six women said that they had never menstruated, of whom eight said that they had at least one child. We speculate that these women did not understand the question. Of 3,555 women, 304 (8.6%) were using a hormonal intrauterine system and 41 (1.2%) were using progestin-only pills containing norethisterone acetate or levonorgestrel.
Characteristics of Study Participants at the Time of Completion of the Questionnaire
Characteristics of menstrual cycles
The median (IQR) age of menarche was 13.0 (2.0) years (Table 2). The current menstrual cycle length was reported as 22–35 days by 70.0% of the participants with a duration of bleeding that was less than 7 days in 2,790 (78.5%). Of 3,555 women, 1,573 women (44.2% [95% CI: 42.6%–45.9%]) reported moderate to severe dysmenorrhea and 774 women (21.8% [95% CI: 20.4%–23.2%]) reported heavy to very heavy bleeding. Of the 774 women reporting heavy bleeding, 535 (69.1% [95% CI: 65.8–72.3]) reported dysmenorrhea, whereas only 1,038 of 2,781 women who did not report heavy bleeding (37.3% [95% CI: 35.5–39.1]) reported dysmenorrhea (chi 2 = 248.2, p < 0.001).
Characteristics of Menstrual Cycles (n = 3,555)
Nineteen women were excluded because they reported values under 7 and over 21 years for the age of menarche.
The following instructions were given to women for the question of “Please indicate on a scale of 1–6, how heavy your periods are.”
Light - On the heaviest day of bleeding I only need to change my pad or tampon every 4 hours or more; Moderate bleeding - On the heaviest day of bleeding I change my pad or tampon every 2–4 hours or more; Heavy bleeding - On the heaviest day of bleeding I need to use double protection such as a pad and a tampon or 2 pads and change every 2 hours. Very heavy bleeding - I experience clotting, “flooding”, and need to use double protection and have to change at least every 2 hours.
IQR, interquartile range.
Association of moderate to severe dysmenorrhea with workability
Information about the hours worked was reported by 2,325 (97.3%) of the 2,390 participants working outside home. The most common occupations of these 2,325 women were professional and managerial roles (882, 38.0%), followed by clerical/admin positions (385, 16.6%), sales jobs (317, 13.6%), and community and personal services (266, 11.4%) sectors.
Poor-moderate workability was reported by 600 (25.8%), and 10 days or more of sick leave in the past year was reported by 325 (14.0%) (Table 3). Women with moderate to severe dysmenorrhea reported higher poor-moderate workability compared with women with no/somewhat dysmenorrhea (31.5% vs. 21.4%, Table 3; p < 0.001). Women with moderate to severe dysmenorrhea were also more likely to report 10 or more days of sick leave in the past year (18.8% vs. 10.3%, p < 0.001).
Self-Reported Workability and the Number of Days of Sick Leave in the Last Year
A score of 37–49 of the Workability Index is considered “Good-excellent,” and 7–36 “Poor-moderate” workability.
Of the 2,390 women working outside the home, 2,325 (over 97%) provided information about the hours worked and were included in the analysis.
Women with moderate to severe dysmenorrhea were 1.5 (95% CI: 1.3–1.9, p < 0.001) times more likely to report poor to moderate workability compared with women with no/somewhat dysmenorrhea (Model 1, Fig. 2). Adjusting for sociodemographic factors (model 2), followed by Inclusion of a term for heavy menstrual bleeding (Model 3), did not appreciably change the odds ratio (OR) for the dysmenorrhea term, and the term for heavy menstrual bleeding was not statistically significant in its own right (Model 3). Women with moderate to severe dysmenorrhea were more likely to report 10 or more days of sick leave compared with women with no/somewhat dysmenorrhea (Model 1, Fig. 2), even after including other sociodemographic factors (Model 2) and menstrual bleeding (Model 3, OR 1.9 [95% CI: 1.5–2.5], p < 0.001).

Modeling of dysmenorrhea on poor-moderate workability, as well as dysmenorrhea on the likelihood of absence from work in the preceding year.
Although collinearity of dysmenorrhea and heavy bleeding may have influenced our findings, we consider this unlikely as the beta coefficient for dysmenorrhea remained stable irrespective of what else was entered into the model. However, to explore this further a four-way variable that included all options of dysmenorrhea (yes/no) and heavy bleeding (yes/no) was generated and examined in model 3. The results were that heavy bleeding alone (no dysmenorrhea) did not affect workability or sick days, whereas dysmenorrhea only or dysmenorrhea with bleeding was significant. This demonstrated that the effect of dysmenorrhea on work was seen in women with and without heavy bleeding.
Discussion
In this large community-based, cross-sectional study, 44% of naturally menstruating Australian women, aged 18–39 years, not using hormonal contraception, experienced moderate to severe dysmenorrhea and 20% reported heavy to very heavy menstrual bleeding. Women with dysmenorrhea were 50% more likely to report poorer work performance and twice as likely to report more days of sick leave in the past year than other women.
A direct comparison between our study and other studies for the prevalence of dysmenorrhea is not possible due to high variation in data quality, study settings (community vs. clinics vs. postal or online survey), or sampling methods (using social media platform vs. a random representative sample). Furthermore, studies might have focused only on menstrual symptoms or on different health aspects, and might have included participants from different age groups and with varying usage of hormonal contraception. These studies also utilized different measures for assessing the severity of dysmenorrhea (numeric Likert scale vs using categories such as mild, moderate, or severe). However, despite the limitations of direct comparison, our findings lend further support to the body of literature highlighting the high prevalence of dysmenorrhea in women and underscore the importance of addressing this common issue through effective management strategies.
Similarly, heavy menstrual bleeding is a common health issue among women of reproductive age which has a profound negative impact on women's life. 13 –16 In a community-based survey of 2,833 women aged 25–44 in the United Kingdom, 35.2% reported their periods as heavy or very heavy along with a range of bothersome menstrual symptoms such as pain (most bothersome symptom), heaviness, mood changes or tiredness, and irregularity. 14 In the subsequent qualitative study, women with heavy or very heavy bleeding viewed this as problematic as it interferes with their usual roles at home or at work. 14 Similarly, findings from a large survey among 4,506 women aged 18–57 in five European countries revealed that more than 25% of women had experienced excessive menstrual bleeding within the previous year. Accordingly, just under half the women reported symptoms typical of iron deficiency, such as fatigue, while almost half women with heavy bleeding had never consulted a physician. 13
Dysmenorrhea can have significant individual, societal, and economic consequences. 17,18 Absence from work and school and interfering with life activities are some examples of the negative impact of dysmenorrhea reported by women of different ages. 18 –20 In terms of the economic impact, dysmenorrhea and associated symptoms contributed to an estimated annual loss of 600 million hours or $2 billion in the United States due to missed work or reduced functionality. 21
In terms of the impact of heavy bleeding, two third of women with heavy bleeding reported moderate to major negative impact on their productivity at work. 13 Another large representative sample of 3,133 community-based women aged between 18 and 64 years in the United States showed that of the 373 women with heavy blood flow, 31% were aged 18–39 years and that women with a heavier flow were only 72% as likely to be working as were women with a lighter or normal flow.
When it comes to the economic implications, an annual work loss of $1,692 per woman was estimated to be due to increased menstrual blood flow. 15 In our study we found a strong association between the symptoms of dysmenorrhea and heavy bleeding. In our models for reduced workability and absenteeism, once dysmenorrhea was taken into account, there was no extra significant contribution from heavy bleeding to these outcome measures. Therefore, previous studies that have reported an association between poorer workability and heavy bleeding without considering menstrual pain may be overlooking the fact that heavy bleeding as a symptom is confounded by dysmenorrhea.
There is an array of therapies available to Australian women, supported by national health care, for both dysmenorrhea and heavy bleeding, including, but not limited to anti-inflammatories, antifibrinolytic agents, and oral and nonoral hormonal contraceptives. In this context, the high prevalence of each of dysmenorrhea and heavy to very heavy bleeding in our study sample is of concern as it appears to be the prevalence among women not receiving adequate treatment. Health care providers (HCPs) are in a unique position to offer help and advice to women using a shared-decision making model. In caring for women of reproductive age, clinicians should assess menstrual problems at different time points and encourage women to talk about menstrual problems in their broadest sense and clarify presenting symptoms and their impact on personal life and work.
Raising women's awareness regarding symptomology, especially dysmenorrhea, self-care, and when to visit an HCP, is imperative to ensure timely investigation and treatment, if required. 7 Information can be delivered to women via different ways such as mobile app or pamphlets or verbally in each visit. A recent study on using a fertility tracking mobile app to track physical and psychological symptoms through the menstrual cycle has shown promising results in increasing workability and decreasing days of sick leave in a U.S. study. 2
To reduce the burden of menstruation morbidity and provide support to working women, “menstrual policy” has been introduced with Spain recently announcing plans to legislate menstrual leave for women who experience severe menstrual pain. Some Asian countries such as Japan, South Korea, and Indonesia and also Soviet Union (in the past) have already introduced menstrual leave with some other countries such as Australia starting the conversation about having a similar policy. 22,23 In a large global survey, more than half of study participants who have menstruated said that having a day off to rest would make their period a better experience. 24
Following this survey, the Victorian Women's Trust in Australia introduced a menstrual policy in May 2016 and has published a blog to encourage other workplaces to adopt their policy. 24 The policy includes offering work flexibility, using a comfortable workstation, and the right to access paid leave without providing a doctor's certificate. After implementing their menstrual policy at the Victorian Women Trust, while employees appreciated personal support given at their workplace, they reported being more involved in their self-care, which, in return, increased their commitment to the team and productivity at work. 23 Nonetheless, the first step for any women with dysmenorrhea and/or menorrhagia should be formal medical assessment to exclude pathological causes and provide management options.
This study has strengths and limitations. The women in the study were similar to young Australian women aged 18–39 years on a range of different parameters with a relatively small difference in the proportion who were married or working full-time. That the women were recruited to a study of women's health not menstruation disorders minimized the likelihood of selection bias. Women using systemic and intra-uterine hormonal contraceptives were not included, and many of these women could have been using these therapies to manage their dysmenorrhea and/or heavy bleeding. Therefore, our prevalence estimates for these conditions are highly conservative. Unfortunately, we did not ask women if they had ever consulted an HCP for their symptoms or if they had been diagnosed with specific conditions associated with these menstrual problems. Some factors that may influence workability were not controlled for in the analysis, such as workplace conditions and access to menstrual hygiene products.
Conclusions
Dysmenorrhea and moderate to heavy bleeding remain common among Australian working women aged 18–39 years, despite the availability of safe and effective management options. Dysmenorrhea negatively impacts workability and is associated with absenteeism. Awareness needs to be raised among women and HCPs of ways to manage dysmenorrhea and heavy bleeding and the unmet community need for intervention, respectively.
Authors' Contribution
E.F.: Formal analysis (lead), Writing—original draft (lead); R.J.B.: Conceptualization, Funding Acquisition, Methodology, Supervision, Writing—review & editing; P.J.R.: Formal analysis, Writing—review & editing (equal); M.S.: Data Curation, Writing—review & editing (equal); S.R.D.: Conceptualization (lead), Funding Acquisition, Supervision, Writing—review & editing (equal).
Footnotes
Author Disclosure Statement
S.R.D. has been paid for developing and delivering educational presentations for Besins Health care, Abbott, Mayne Pharma, and BioFemme, has been on advisory boards for Theramex, Abbott Laboratories, Mayne Pharma, and Roche and a consultant to Lawley Pharmaceuticals, Southern Star Research, and Que Oncology, and has received institutional grant funding from Que Oncology and Ovoca Bio. Other authors have no conflict of interest to report.
Funding Information
The study was supported by the Grollo-Ruzzene Foundation, Melbourne Australia. This study forms part of the PhD thesis -for M.A.S. who has been awarded a PhD Scholarship Australian Postgraduate Award. S.R.D. is an Australian NHMRC Senior Principle Research Fellow (Grant No. 2016627).