
Abstract
Background:
This study aimed to determine whether birthing people who experience severe maternal morbidity (SMM) are more likely to be diagnosed with a postpartum mental illness.
Materials and Methods:
Using the Massachusetts All Payer Claims Database, this study used modified Poisson regression analysis to assess the association of SMM with mental illness diagnosis during the postpartum year, accounting for prenatal mental illness diagnoses and other patient characteristics.
Results:
There were 128,161 deliveries identified, with 55.0% covered by Medicaid. Of these, 3.1% experienced SMM during pregnancy and/or delivery hospitalization, and 20.1% had a mental illness diagnosis within 1 year postpartum. In adjusted regression analyses, individuals with SMM had a 10.6% increased risk of having any mental illness diagnosis compared to individuals without SMM, primarily due to an increased risk of a depression or post-traumatic stress disorder diagnosis among people with SMM than those without SMM.
Conclusions:
Individuals who experienced SMM had a higher risk of a mental illness diagnosis in the postpartum year. Given increases in SMM in the United States in recent decades, policies to mitigate mental health sequelae of SMM are urgently needed.
Introduction
Severe maternal morbidity (SMM) occurs in ∼1%–2% of births, has more than doubled in recent decades, and is associated with both short- and long-term health consequences. 1 –3 In addition to persistent racial and ethnic disparities in SMM incidence, 4 –6 some studies have found disparities in SMM by insurance type, with higher rates among Medicaid-insured versus commercially insured individuals. 7 –9 These insurance disparities seem to be driven, in part, by differences in the hospitals where people with Medicaid versus private insurance receive care. Recent research findings show limited within-hospital SMM disparities by insurance, while SMM rates are higher in hospitals with larger numbers of Medicaid-insured births. 7
Childbirth can prompt new onset or recurrent episodes of a range of psychiatric disorders. 10 –12 SMM is often experienced as a traumatic event, 13 –15 which could potentially lead to negative mental health outcomes during the postpartum period. Several studies have examined the relationship between SMM and mental health outcomes.
A recent US study used a large statewide database of inpatient and emergency department (ED) utilization from 2005 to 2015 and found that individuals who experienced SMM had 70% higher odds of an ED visit or hospital admission for psychiatric conditions in the postpartum year compared to those who had not experienced SMM, 16 but this study did not examine treatment in more common outpatient settings. A study based in Sweden found that birthing people who experienced SMM were more likely to receive psychiatric treatment through inpatient psychiatric hospitalization and psychiatric outpatient clinics, and to be prescribed psychotropic drugs than people who had not experienced SMM. 17
A small body of research has assessed the correlation between SMM and post-traumatic stress disorder (PTSD) specifically. A systematic review conducted in 2012 identified 11 studies assessing the relationship between SMM and PTSD and found inconsistent findings across the studies. 18 However, no study in the review used a definition of SMM that was broadly consistent with the definition by the Centers for Disease Control and Prevention (CDC).
The CDC defines SMM as “unexpected outcomes of labor and delivery that result in significant short- or long-term consequences to a woman's health,” including conditions such as eclampsia, sepsis, shock, or requiring ventilation, and specifies International Classification of Diseases (ICD) diagnosis and procedure codes that can be used to identify 21 indicators of SMM in administrative data. 19 For example, in the one US-based study in the review, maternal morbidity was based on report of a “birth complication” and did not provide a more specific definition. 18,20 Other studies from Europe defined maternal morbidity based on the presence of preeclampsia only, 18,21,22 which is not as severe a complication as those included in the CDC definition we use.
In addition, the studies did not require a PTSD diagnosis, but instead were based on PTSD symptoms. 18 Furthermore, a number of these studies excluded people with conditions such as preterm delivery, pregnancy complications, or preexisting mental illness, 18 all of which may be associated with SMM. 23,24 Another study using data from a maternity unit in England found a higher risk of PTSD symptoms at 6–8 weeks postpartum among individuals who had experienced SMM, 25 but did not examine specific diagnoses or a longer postpartum period.
It is not known whether US birthing people who experience SMM are more likely to be diagnosed with a mental illness in the postpartum period across health care settings, including outpatient settings. Also, although birthing people with Medicaid insurance are more likely to experience SMM than commercially insured individuals, it is not known if the relationship between SMM and mental health outcomes varies by insurance type. Individuals with Medicaid coverage may be less likely to receive a mental health diagnosis during the postpartum period—even if they are experiencing mental health challenges—due to lower rates of postpartum follow-up care receipt among this population. 26
Some studies have also found lower rates of depression screening for those who do have a postpartum visit, 27,28 although others have not. 29 This study expands on previous research by using a statewide dataset to examine the association between SMM and mental illness diagnosis in the postpartum year, distinguishing by insurance type at delivery. We hypothesize that individuals who experienced SMM are more likely to have a mental illness diagnosis in the postpartum year, and that the relationship between SMM and mental illness varies based on insurance type.
Materials and Methods
Overview
Using the Massachusetts All Payer Claims Database (MA APCD), we estimated the association between experiencing SMM during pregnancy and delivery and postpartum mental illness. We used a modified Poisson regression model with clustered standard errors by patient ZIP code to assess the association of SMM with overall and specific mental illnesses, adjusting for prenatal diagnosis of mental illness and other factors associated with postpartum mental illness.
Data and analytic sample
We used data on deliveries to Massachusetts residents from the MA APCD (v.8.0, 2014–2018), maintained by the Massachusetts Center for Health Information and Analysis. The MA APCD includes health insurance enrollment and claims data for individuals with private and Medicaid (both fee-for-service and managed care) insurance. We identified births in data using procedure codes and International Classification of Diseases, Ninth Revision (ICD-9), and International Classification of Diseases, Tenth Revision (ICD-10) codes, as defined in the Alliance for Innovation on Maternal Health's Birth Admissions algorithm. 30
We limited the sample to singleton live births between October 1, 2014, and December 31, 2017, to individuals who were covered by Medicaid or private insurance at delivery and who were continuously observed during the 12 months postpartum; this allowed us to observe prenatal diagnoses as well as diagnoses 1 year postpartum for all deliveries. To measure prenatal diagnoses, we defined the prenatal period as 280 days before the delivery date. Due to privacy restrictions, all ICD-9 and ICD-10 codes have been redacted from claims that include a primary or secondary substance use disorder (SUD).
Measures
The primary outcome measure was a binary variable indicating “any mental illness,” defined as the presence of at least one diagnosis code indicating the following mental health conditions occurring between the delivery date and 1 year postpartum: bipolar disorder, depression, anxiety disorder, PTSD, and schizophrenia and other psychoses (Supplementary Appendix Table SA1). 31 –39 We included this range of indicators of mental illness to capture associations of SMM with the spectrum of type and severity of mental illness. As secondary outcome measures, we created separate binary variables for each postpartum mental health condition.
The key independent variable was SMM during pregnancy or the delivery hospitalization. We defined SMM using ICD-9, ICD-10, and Current Procedural Terminology codes based on guidance from the CDC (Supplementary Appendix Table SA2). 40 We defined SMM with and without the most common indicator, blood transfusion. The version of SMM omitting blood transfusion was used to conduct sensitivity analyses.
Statistical analysis
We first calculated descriptive statistics and tested for significant differences between deliveries with and without SMM using t-tests (for continuous variables) and chi-square tests (for binary variables). To examine whether postpartum mental health diagnoses differed by experience of SMM, we estimated modified Poisson regression models for each binary outcome, with a binary indicator of SMM as the key independent variable. To adjust for other factors, we included measures of prenatal mental illness diagnoses, as well as sociodemographic characteristics as covariates. Prenatal mental health diagnoses were a series of binary variables indicating mental health diagnoses that occurred during pregnancy (280 days before delivery) or at the time of delivery, including the same categories of mental health conditions used in the outcome variables. Each model included individual indicators for prenatal or delivery diagnosis for each of mental health condition.
We included the following control variables, which prior research has found to be associated with SMM and/or perinatal mental illnesses: Delivery mode (vaginal vs. cesarean), 41,42 preterm birth, 43,44 any diagnosis of diabetes (prepregnancy or gestational), 45,46 and any diagnosis of hypertensive disorders of pregnancy. 47 –49 We also included variables measuring the individual's insurance type in the delivery month (Medicaid vs. private insurance), age at delivery (categorical), year of delivery (categorical), and characteristics of the ZIP code of residence. ZIP code characteristics included the percentage of the population that was Black, the percentage of the population that was Hispanic/Latino, concentrated poverty (>30% of population with income less than federal poverty line), 50 and whether the ZIP code was in the bottom quartile of median income.
We present relative risk ratios for each outcome, comparing those with and without SMM. We also present the predicted number of deliveries with a mental illness diagnosis per 100 deliveries, as well as the adjusted risk difference for some key outcomes. In an additional analysis, we estimated models stratified by insurance type to examine the association of SMM with mental illness outcomes for people with Medicaid and for those with private insurance.
As a sensitivity analysis, we estimated models using the SMM variable, excluding blood transfusion. In additional sensitivity analyses, we estimated separate models with the outcome of any mental illness diagnoses postpartum, in which we included indicator variables for (1) any transition in insurance type in the 12 months postpartum (including transitioning from Medicaid to Medicaid managed care and vice versa);( 2) any ZIP code change in the 12 months postpartum; (3) multigravida versus nulliparous; and (4) insufficient prenatal care (using ICD-9/10 codes, as listed in the notes of Supplementary Appendix Table SA5).
Standard errors were clustered at the five-digit ZIP code of patient residence to account for correlation of error terms among people in the same region, as well as to account for correlation that occurs due to inclusion of multiple deliveries for the same individual. The delta method was used to calculate standard errors for the predicted number of events from adjusted models. 51 An alpha of 0.05 was considered significant. Analyses were conducted in SAS 9.1 (SAS Corporation, Cary, NC) and Stata-MP 16.0 (StataCorp, College Station, TX). This study was performed in accordance with the ethics standards of the University of Massachusetts Institutional Review Board, which approved this study.
Results
We identified 128,161 live-born singleton deliveries to individuals residing in Massachusetts, who were continuously observed for the 12 months postpartum (Supplementary Appendix Fig. SA1). Over half (55.0%) the deliveries were covered by Medicaid (Table 1). Around 3.1% of deliveries experienced SMM during pregnancy or delivery, and 32.6% of deliveries were by cesarean. Nineteen percent of deliveries had any diagnosis of mental illness during the prenatal period or delivery hospitalization.
Descriptive Statistics of Analytic Sample
p < 0.001.
Mean presented in “%” column.
p-Values calculated using t-test for continuous variables and chi-square test for binary/categorical variables.
PTSD, post-traumatic stress disorder.
The most common mental illness diagnoses were depression (14.3%) and anxiety disorders (12.0%). Deliveries with SMM were more likely to be by cesarean (p < 0.001), to be preterm (p < 0.001), and to be complicated by a hypertensive disorder of pregnancy (p < 0.001) and/or diabetes (p < 0.001) compared to those without SMM. Prenatal mental illness was also significantly associated with SMM, with those with any prenatal mental illness diagnosis significantly more likely to experience SMM (28.0% of those with SMM had any mental illness vs. 18.7% of those without SMM, p < 0.001).
Overall, 20.1% of the sample experienced any mental illness in the postpartum year (Table 2). Both indicators of any mental illness and each specific disorder were significantly more common among those with SMM than those without (p < 0.01 for each comparison). Among deliveries with SMM, in the postpartum year, 16.5% had depression, 17.1% had an anxiety disorder, and 3.7% had PTSD.
Descriptive Statistics of Postpartum Mental Illness Outcomes, by Severe Maternal Morbidity
p < 0.001. p-values calculated using t-test for continuous variables and chi-square test for binary/categorical variables.
In adjusted analyses, SMM was significantly associated with a 10.6% increased risk of having any mental illness diagnosis postpartum (Supplementary Appendix Table SA3 for full results). For individuals with SMM, 22.2 deliveries of every 100 were predicted to have any mental illness diagnosis postpartum compared to 20.0 deliveries per 100 for individuals without SMM (adjusted risk difference = 2.2 deliveries per 100) (Fig. 1). This increase was primarily due to the finding that in adjusted analyses, individuals with SMM had a significantly increased risk of having a diagnosis of depression and of PTSD compared to those without SMM. For individuals with SMM, there was a 22.6% increased risk of having a depression diagnosis versus those without SMM (95% confidence interval [CI]: 15.0–30.7). For individuals with SMM, there was a 22.6% increase in the risk of having a PTSD diagnosis (95% CI: 5.3–42.9) versus those without SMM.
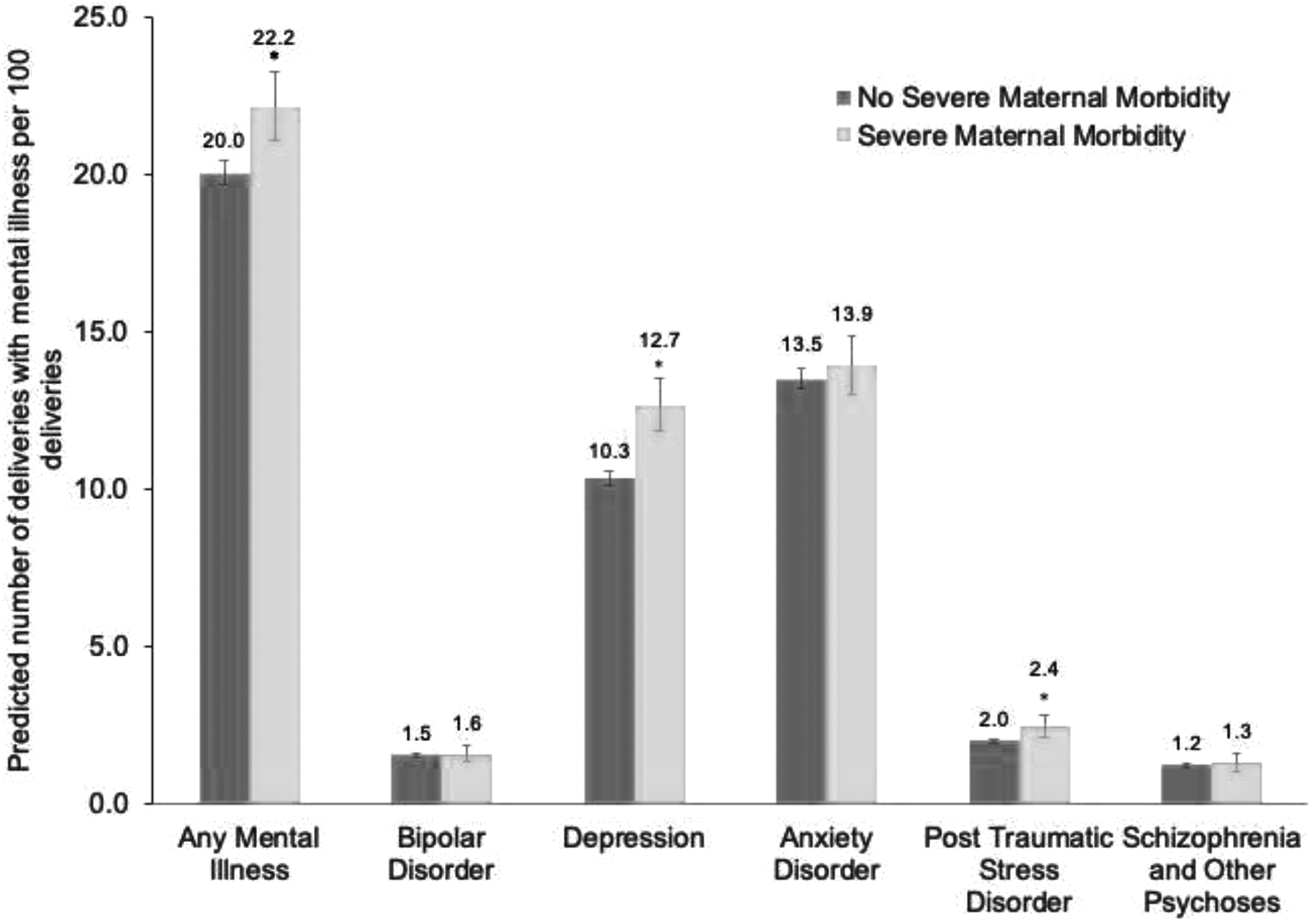
Regression adjusted predictions of postpartum mental illness, by SMM. “*” Indicates risk difference is statistically significant at the 5% level. Vertical bars show 95% CIs around predictions. Predictions are generated using modified Poisson models with clustered standard errors adjusting for age (categorical), insurance type (Medicaid vs. private insurance), delivery mode, preterm birth, any diabetes, any hypertensive disorder of pregnancy, delivery year (categorical), and binary prenatal mental illness diagnoses. Standard errors are clustered by five-digit ZIP code of patient residence. CI, confidence interval; SMM, severe maternal morbidity.
Individuals with Medicaid had a 6.7% higher risk of at least one mental illness diagnosis in the postpartum period in adjusted analyses (Supplementary Appendix Table SA3). In stratified models for those with private insurance and Medicaid, the association of SMM with higher risk of any mental illness was present for both insurance types, but was only statistically significant for those with Medicaid (Supplementary Appendix Table SA4). The association between SMM and higher risk of depression was significant for both Medicaid-insured and privately insured individuals. In these models, we additionally found that, although there was a higher risk of PTSD among those with SMM for both insurance types, the association was only significant for privately insured individuals and not among Medicaid-insured individuals.
When we examined the sensitivity of our results to the definition of SMM, excluding transfusion, we found that the association of SMM with any mental illness was consistent with the main analysis, with an increased risk of 7.8% for those with SMM, excluding transfusion, versus those without SMM (95% CI: 2.1–13.8; adjusted risk difference = 1.6 deliveries/100) (Fig. 2). The statistically significant association of SMM with a postpartum diagnosis of depression persisted when transfusion was excluded from the definition of SMM; individuals with SMM, excluding transfusion, had a 21.9% increase in the risk of depression (95% CI: 13.6–30.8). When transfusion was excluded from the definition of SMM, there was no longer a statistically significant association between SMM and postpartum diagnosis of PTSD.

Regression adjusted predictions of postpartum mental illness, by SMM, excluding transfusion. “*” Indicates risk difference is statistically significant at the 5% level. Vertical bars show 95% CIs around predictions. Sensitivity analysis where primary variable of SMM does not include blood transfusion. Predictions are generated using modified Poisson models with clustered standard errors adjusting for age (categorical), insurance type (Medicaid vs. private insurance), delivery mode, preterm birth, any diabetes, any hypertensive disorder of pregnancy, delivery year (categorical), and binary prenatal mental illness diagnoses. Standard errors are clustered by five-digit ZIP code of patient residence.
Results from other sensitivity analyses indicated that when we adjusted for indicators of postpartum insurance stability, housing stability, insufficient prenatal care, and multiparity, the relationship between SMM and postpartum mental illness diagnosis was consistent with our main results (Supplementary Appendix Table SA5). In each of these sensitivity analyses, the association between SMM and postpartum mental illness diagnosis was similar in direction and magnitude as in our main results, suggesting that these factors were not driving our results.
Discussion
Findings from this large retrospective cohort study showed that individuals who experience SMM are at an increased risk of mental illness diagnosis in the year postpartum. In further analyses identifying specific mental illness diagnoses, we found that the increase in risk is largely driven by increases in diagnoses of depression and PTSD. In analyses using a measure of SMM that did not include transfusion, the association between SMM and PTSD diagnosis was no longer statistically significant, but the association with depression diagnosis persisted. There was no association between SMM and other mental illness diagnoses such as bipolar disorder or schizophrenia and other psychoses. Medicaid-insured individuals were more likely to experience SMM and more likely to have a postpartum mental illness diagnosis; however, contrary to our hypothesis, the association between SMM and overall mental illness diagnosis did not vary by insurance type.
Our findings are consistent with prior studies linking experience of SMM to postpartum mental health. 16 –18,23 –25 One of the few prior population-based studies examining SMM and postpartum mental health diagnosis in hospital and outpatient treatment settings was conducted in Sweden; our findings indicate a similar association in the US context, in the state of Massachusetts. An earlier US study conducted using data from Florida examined SMM and postpartum mental illness diagnosis in ED visits and hospital inpatient admissions. 16
Our findings show an association between SMM and mental health diagnosis in all treatment settings, including outpatient settings; the latter may represent clinically significant, but less severe mental illness presentations than those requiring care in the ED and/or inpatient setting. The prior study did not report on an association between SMM and PTSD specifically, due to the very low prevalence of PTSD diagnoses in the sample. 16 Although we find that PTSD in the postpartum period is relatively uncommon in this cohort, in comparison to depression and anxiety disorders (2.0% PTSD vs. 10.4% depression, 13.5% anxiety disorder), it was common enough for us to detect that the overall increase in the risk of postpartum mental health diagnoses was partly attributable to more frequent PTSD diagnoses among individuals who had experienced SMM.
We also found that individuals with a mental illness diagnosis prenatally were more likely to experience SMM. This aligns with findings from other recent studies 23,24,52 and suggests that the relationship between SMM and mental illness may be bidirectional. Given that perinatal mood disorders are estimated to impact at least one in seven perinatal individuals, 53,54 better understanding how to deliver high-quality care to this population in a way that improves maternal mental and physical health outcomes is critical.
Our findings indicate that there is a need to develop policies and clinical practices to offer follow-up, communication and support to birthing people who have experienced SMM. This support could start during the birth hospitalization if SMM occurs, and include mental health support. One suggested clinical practice has been to have a postpartum debriefing session with a maternity care provider or other trained clinician, which would create an opportunity to process potentially traumatic events, provide information to the postpartum individual, and allow them to ask any question that they might have. 14,55 However, there is no high-quality evidence to support the efficacy of this practice. 56
We found that the association of SMM with higher risk of any mental illness, depression, and PTSD was present for those with both Medicaid and private insurance, although statistical significance of results varied. Medicaid-insured birthing people may face more barriers to receiving mental health treatment, given the higher rates of insurance churn, including spells of uninsurance, in this population. 57 –61 The comprehensive postpartum visit is a key place where mental health issues requiring further treatment may be identified 29,62 ; birthing people with Medicaid have been shown in a recent systematic review to have lower rates of postpartum visit attendance. 26
In addition, a recent study found that individuals experiencing postpartum insurance instability were less likely to report having discussed mental health at a postpartum visit, and less likely to receive mental health services. 63 These insurance-related barriers may compound the known noninsurance-related challenges with access to perinatal mental health care. 64 Policy responses to inadequate treatment access include extending postpartum Medicaid coverage through at least 1 year, which a number of states are in the process of implementing, 65 as well as creating and expanding programs that reduce other barriers to treatment access. For example, Massachusetts has a program that expands the capacity of obstetric care providers to treat mental health disorders by providing training and creating access to telephone consultation with and referrals to perinatal psychiatrists. 66
Limitations
There are several limitations of the analysis. First, we cannot distinguish new postpartum diagnoses of mental illness from preexisting mental illness. However, we have controlled for prenatal diagnoses of mental illness, including those recorded during the delivery hospitalization. As we include diagnoses from all settings of care, we are accounting for diagnoses arising from treatment for mental illness and comorbid diagnoses. Despite the controls for prenatal diagnoses, our analysis does not account for mental illness diagnoses before pregnancy, which do not appear on claims during the prenatal period.
Second, as claims data are generated for billing purposes, it is possible that some mental illness diagnoses may be included for people who do not fully meet diagnostic criteria for the disorder 67,68 A strength of claims data is that it captures all interactions with the health care system across a period of time through insurance transitions and across health care settings, which is particularly relevant during the perinatal period when insurance transitions are common and individuals may seek care from a number of different sources. 61
Future research examining similar questions, but using forms of data that may be able to more accurately capture psychiatric disorders is warranted. Third, all diagnosis codes on claims containing an SUD diagnosis are redacted. This restricts our ability to measure SUD-related diagnoses, an important contributor to preventable maternal mortality. 67 Fourth, there are multiple methods of measuring SMM, which can result in different rates across data sources and methods. 68 We used the definition from the CDC, and included SMM based on claims from the prenatal period and delivery hospitalization. Use of the CDC definition of SMM is a strength as it is validated and has been used in most recent research on SMM using claims data. 8,69 –72
Fifth, there are known inequities in SMM and in mental health care access based on race and ethnicity, but this information is not available in the data source and therefore could not be included in our analysis. Sixth, there may be unobserved confounding due to the limited demographic and socioeconomic characteristics available in the data; therefore, identified associations should not be interpreted as causal. Seventh, due to the Gobeille Supreme Court decision, the MA APCD includes full reporting of Medicaid and Medicaid-managed care plans, but only partial reporting of private insurance plans. 73 Therefore, the sample in our analysis is disproportionately covered by Medicaid compared to the overall birthing population in Massachusetts, and unadjusted results cannot be interpreted as directly representative at the state level.
Finally, our study is based on data from Massachusetts, which may not be generalizable to the rest of the United States, particularly those with high uninsurance rates. States that are expanding health insurance coverage overall and specific to perinatal populations through the Affordable Care Act Medicaid expansion and extended Medicaid eligibility postpartum 74 –76 may become more similar to Massachusetts in terms of health insurance coverage, but the health care context in Massachusetts may continue to be an outlier in some ways, as a state with a high per capita supply of physicians and among the top 10 states in health care quality rankings. 77,78
Conclusions
Individuals who experienced SMM were more likely to be diagnosed with any mental illness, and specifically depression and PTSD, during the postpartum year compared to those who did not experience SMM. Given increases in SMM in the United States in recent decades, policy attention to mitigating the psychiatric sequelae of SMM is urgently needed. Future research and practice changes ensuring that individuals with a new diagnosis or exacerbation of existing mental illness get timely and appropriate care during the postpartum period and beyond are essential, particularly for those who have experienced SMM.
Footnotes
Acknowledgments
The authors would like to thank Michael Cooper and Valerie Evans, who provided research assistance.
Authors' Contributions
L.A.: Conceptualization, writing—original draft, writing—review and editing, and funding acquisition; C.J.: Methodology, data curation, formal analysis, and writing—review and editing; and K.H.G.: Conceptualization, writing—original draft, writing—review and editing, funding acquisition, methodology, and formal analysis.
Disclaimer
The article's contents are solely the responsibility of the authors and do not represent the official views of the Commonwealth Fund or the National Heart, Lung and Blood Institute.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This work was supported by the Commonwealth Fund and the National Heart, Lung and Blood Institute (R56HL151636). The funders had no role in study design, analysis, interpretation of data, or in the preparation, review, or approval of the article, or the decision to submit the article for publication.
Supplementary Material
Supplementary Appendix Table SA1
Supplementary Appendix Table SA2
Supplementary Appendix Table SA3
Supplementary Appendix Table SA4
Supplementary Appendix Table SA5
Supplementary Appendix Figure SA1
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.