
Abstract
Objective:
To evaluate the use of manipulators on the outcome of women who had minimally invasive surgery for endometrial cancer.
Methods:
Retrospective analysis of patients operated with or without an intrauterine manipulator.
Results:
Six hundred ninety-nine patients were included. The median follow-up was 44 months (range, 29–67). Nineteen (8.8%) patients had positive cytology in the manipulator group versus 21 (4.4%) in the comparison group (p = 0.02). Total recurrence rate was similar between the groups (12.3% vs. 11.9%; p = 0.8). Vaginal vault recurrence was the most common site of recurrence with higher incidence in the manipulator group (4.5% vs. 1.3%; p = 0.007). Subgroup analysis of low-risk patients who did not receive adjuvant treatment showed higher recurrence rate (8.3% vs. 3%; p = 0.023) and worse disease-free survival (p = 0.01) for the manipulator group. After controlling for other variables, the use of a manipulator did not affect the risk of recurrence for the whole cohort (hazard ratio [HR], 1.28; confidence interval [95% CI], 0.7–2.1, p = 0.3) and for the low-risk subgroup of patients who did not receive adjuvant treatment (HR, 2.47; 95% CI, 0.8–7, p = 0.08).
Conclusion:
The use of a manipulator increases the risk of positive cytology as well as vaginal vault recurrences, but it does not reduce the overall survival of patients.
Introduction
Currently, the gold standard treatment for patients diagnosed with endometrial cancer is based primarily on staging surgery followed by adjuvant treatment if indicated. 1 Approximately 6%–13% of all patients with endometrial cancer will develop recurrent disease; the majority during the first 3 years after a primary diagnosis with primary location in the vaginal vault. 2
Two minimally invasive surgery (MIS) approaches are used for endometrial cancer staging surgery, total laparoscopic hysterectomy and robotically assisted total laparoscopic hysterectomy. 3 Compared to laparotomy, the benefits of minimal invasive approach hysterectomy for endometrial cancer include reduced blood loss, shorter recuperation time, lower cost, less use of pain medication, faster recovery, similar or fewer postoperative adverse events, and better quality of life up to 6 months after surgery. 4 In addition, no significant difference exists in cancer recurrence or outcome between MIS and laparotomy cases, indicating comparable oncologic safety of MIS. 5
For proper uterine manipulation during minimal invasive hysterectomy, various uterine manipulators are used with or without an intrauterine segment (usually a screw, a rod, or a balloon). 6 The intrauterine component is inserted into the uterine cavity to allow surgeons manipulation of the uterus for better exposure. In addition to the intrauterine component, some of the uterine manipulators have a colpotomizer (cervical cap) that assists in identifying the anatomic landmarks such as the vaginal fornices and allow to increase the distance between the ureter and the vaginal vault. 7
Nevertheless, some surgeons are avoiding the use of the intrauterine component in cases of endometrial cancer, for concern of iatrogenic spillage, uterine perforation, and the potential risk of retrograde dissemination of cancer cells into the peritoneal cavity or the lymphatic spaces. To avoid this potential spread, some surgeons choose either not to use a uterine manipulator at all or to use an uterine manipulator with a colpotomizer but without an intrauterine segment. 8
The aim of this study was to evaluate the effect of the use of an intrauterine manipulator on the recurrence rate and outcome of patients undergoing minimal invasive staging surgery for endometrial cancer.
Methods
A retrospective cohort study identifying consecutive patients who underwent a minimal invasive hysterectomy for endometrial cancer at the McGill university tertiary-care hospitals. Ethical approval and informed consent were waived by the local ethics committee in view of the retrospective nature of the study, and all the procedures being performed were part of the routine care. Surgeries were performed by laparoscopic or robotic approach by six gynecologic oncology surgeons. MIS for staging of endometrial cancer included peritoneal cytology, total hysterectomy and salpingo-oophorectomy, with or without pelvic and/or paraaortic lymph node dissection (LND) or sentinel lymph node detection. In cases where the preoperative histology was papillary serous or clear cell, surgical staging also included omentectomy, examination of the entire abdomino-pelvic cavity, and retroperitoneal spaces. Patients who had uterine perforation, morcellation, or conversion to laparotomy were excluded from the study.
Uterine manipulators that were used were either a Clermont Ferrand manipulator (Karl Storz, Tuttlingen, Germany), RUMI uterine manipulator with a Koh colpotomizer system (Cooper Surgical, Trumbull, CT), or a ZUMI uterine manipulator (Cooper Surgical). In other cases, either a uterine manipulator was not used or an adjustment was made to the Hohl uterine manipulator (Storz, El Segundo, CA) so that it included only the handle with its colpotomizer without its intrauterine component as described previously by our group. 8 The decision as to the type of intrauterine manipulator or lack of it was left to the discretion of the surgeon.
Data were collected from the department's digital records, including operative reports, pathology reports, chemotherapy records, radiation oncology reports, laboratory results, and radiology reports were reviewed to determine baseline and perioperative characteristics until the end of follow-up period or death for each patient.
Baseline characteristics included age, body mass index (BMI), and medical comorbidities. Perioperative data included the surgical procedure with the type of uterine manipulator or colpotomizer used, stage of malignancy, grade, histology, depth of myometrial invasion, lymph-vascular space invasion, fallopian tube and ovarian involvement, lower uterine segment and cervix involvement, lymph node involvement with total count, and pelvic cytology. Postoperative complications were collected in real time.
For those patients who had recurrence, disease-free survival (DFS) was defined as time from last treatment to the diagnosis of recurrence. Overall survival (OS) was defined as time from diagnosis to time of last follow-up or death. Recurrences were diagnosed clinically or radiologically. All vaginal recurrences were biopsy-proven. During the surveillance period, routine follow-up examinations were performed at intervals of 4 months during the first 2 years, followed by every 6 months for up to 5 years, and then yearly until the end of the follow-up period or death.
To assess the effect of different uterine manipulator types on lymph vascular space invasion (LVSI), positive cytology and patient's outcome, patients were divided into two groups. The first group (Intrauterine manipulator group) included patients who were operated using a uterine manipulator that necessitates a cervical OS dilation before the placement of the intrauterine rod (Clermont Ferrand, RUMI or ZUMI) and a second group (No intrauterine manipulator group) of patients that were operated either without a uterine manipulator or using the intravaginal part of a Hohl uterine manipulator without the intrauterine manipulator, as previously published.
Statistical analysis was done using SPSS software (IBM, SPSS statistics, Version 25, 2017; IBM® corp. Armonk, NY). All statistical analyses were two-sided, and p < 0.05 was considered significant. Continuous variables were compared using either one-way ANOVA or Kruskal–Wallis and Mann–Whitney tests according to distribution of variables. Chi squared test or Fishers' exact test were used to compare categorical variables. DFS and OS were calculated using Kaplan–Meier estimator and compared with log rank test with reverse censoring method. Univariate as well as multivariate cox regression analysis was used to evaluate the association between each of the predictors and DFS and OS.
Results
During the study period, we identified 782 patients who underwent minimal invasive hysterectomy for endometrial intraepithelial neoplasia (EIN) and newly diagnosed endometrial cancer. Eighty-three patients (10.6%) were excluded from the study: 54 patients with EIN, 22 patients required conversion to laparotomy (2.8%), most of those required a simple mini-laparotomy at the end of the procedure to remove the uterus that could not be removed intact via the vagina, and 9 patients had a large uterus that was morcellated within an endobag placed via the vagina (1.1%). After exclusion, 699 patients were included in the analysis and the clinicopathologic characteristics are presented in Table 1.
Patient Characteristics and Surgical Outcomes (n = 699)
Tumor stage is presented according to the 2009 International Federation of Gynecology and Obstetrics stage and histologically classified and graded according to the World Health Organization.
BMI, body mass index; BSO, bilateral salpingo-oophorectomy; CF, Clermont Ferrand; CTx, chemotherapy; PaLND, para aortic lymph node dissection; PLND, pelvic lymph node dissection; RTx, radiotherapy; SD, standard deviation; TH, total hysterectomy.
The mean patient age was 64 years (standard deviation [SD] 11), and the mean BMI was 31.7 kg/m2 (SD 8.6). Six hundred thirteen patients (88%) underwent robotic-assisted hysterectomy and 86 patients (12%) underwent laparoscopic hysterectomy. In 484 patients (69%), the procedure included pelvic lymph node dissection (PLND) and for 203 patients (29%), para aortic lymph node dissection was performed in addition to PLND. The most common uterine manipulator used was the Hohl retractor (60%) without intrauterine component, followed by the Clermont–Ferrand manipulator (19%).
The majority of patients had stage I disease (n = 528, 75%) and endometrioid histology (n = 546, 78%), whereas 205 patients (29%) had grade 3 disease. Three hundred thirty patients (44%) with moderate-to-high risk factors received adjuvant treatment, either radiotherapy, chemotherapy, or a combination of the two. The median follow-up time was 44 (range 29–67) months.
Out of the 699 eligible patients, 220 (31.4%) underwent surgery with the support of an intrauterine manipulator (Intrauterine manipulator group) and in 479 patients (68.6%), no intrauterine manipulator was used (No intrauterine manipulator group). The distribution is presented in Figure 1. There were no significant differences between the two groups with regard to age at surgery, BMI, histologic type, FIGO stage, LVSI, tumor size, and lymph node retrieval number (Table 2). Women in the intrauterine manipulator group had significantly more grade 1 disease (50% vs. 39%, p = 0.01) and positive cytology (8.8% vs. 4.4%, p = 0.02) compared to women in the no intrauterine manipulator group. Eighty-seven patients (39.5%) in the intrauterine manipulator group compared to 243 (50.7%) in the no intrauterine manipulator were classified to be intermediate/high risk for recurrence and received adjuvant treatment (p = 0.006).
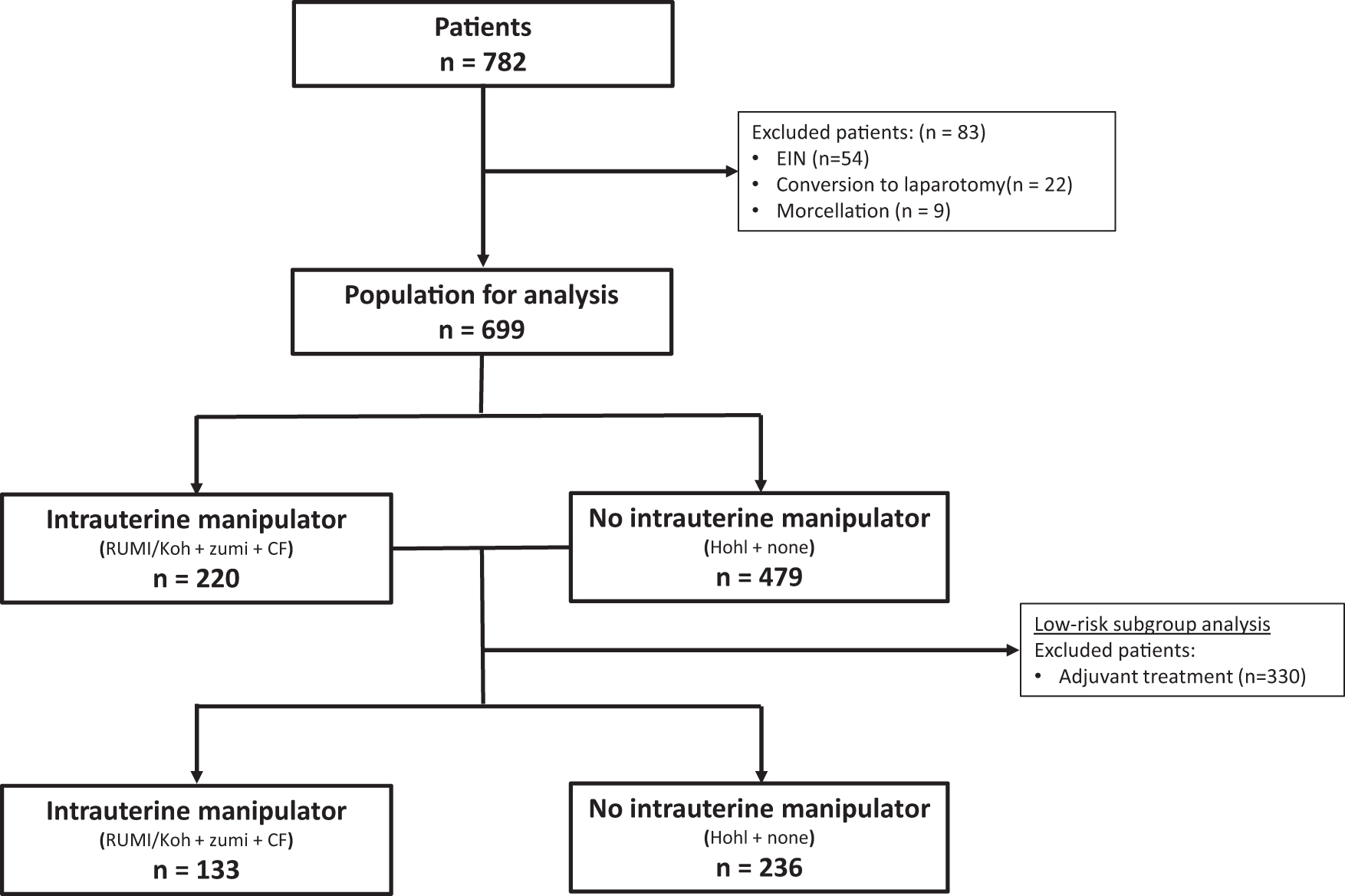
Distribution of patients eligible for analysis. EIN, endometrial intraepithelial neoplasia.
Patient Characteristics and Surgical Outcomes with Patterns of Recurrence for Patients Who Did Not Receive Adjuvant Treatment (n = 699) and Subgroup Analysis for Patients Who Did Not Receive Adjuvant Treatment (n = 369)
Significant values are in bold.
Tumor stage is presented according to the 2009 International Federation of Gynecology and Obstetrics stage and histologically classified and graded according to the World Health Organization.
Twenty-seven patients (12.3%) recurred in the intrauterine manipulator group, compared to 57 (11.9%) patients in the no intrauterine manipulator group (p = 0.88). Vaginal vault recurrence was the most common site of recurrence, occurring in 10 (4.5%) patients in the intrauterine manipulator group versus 6 (1.3%) patients in the no intrauterine manipulator group (p = 0.007). Nine patients (4.1%) in the intrauterine manipulator group had pelvic recurrences versus 9 pelvic recurrences (1.9%) in the no intrauterine manipulator group (p = 0.08). Lower-limb lymphedema was the most prevalent postoperative complication, occurring in 16 (7.3%) patients of the manipulator group compared to 12 (2.5%) patients in the no manipulator group (p = 0.003). Less common complications were wound and urinary infections but did not show statistical difference. Median DFS and OS were not reached and were not statistically different between the two groups.
To further assess the effect of uterine manipulation on patient's outcome, we have performed a subgroup analysis of all low-risk patients who did not receive adjuvant treatment (Table 2). In the intrauterine manipulator group, 11 (8.3%) patients recurred as compared to 7 (3%) in the no intrauterine manipulator group (p = 0.02), with a 5.3% rate of vaginal vault recurrence compared to 0.8% (p = 0.01). Median DFS was not reached; however, in a Kaplan–Meyer survival analysis, patients in whom no intrauterine manipulator was used had significantly better DFS (Fig. 2B, p = 0.01). When all the patients were included, whether they received adjuvant treatment or not, no significant differences in DFS could be observed between the groups (Fig. 2A).

Disease-free survival, Kaplan–Meyer curves compare disease-free survival in the manipulator versus no manipulator groups, for patients who received adjuvant treatment
To better assess the association between the use of intrauterine manipulator and recurrence rate as well as outcome of patients, a univariate (Table 3) and multivariate analysis were performed (Table 5). Figo stage, grade, LVSI, positive cytology, and adjuvant treatment were all independently associated with risk of disease recurrence and decreased OS. For the whole cohort, the use of a uterine manipulator was not associated with the risk of relapse of endometrial cancer in both univariate (hazard ratio [HR], 1.1; confidence interval [95% CI], 0.7–1.8, p = 0.5) and multivariate analysis (HR, 1.28; 95% CI, 0.7–2.1, p = 0.3). However, the use of a uterine manipulator reached statistical significance for risk of relapse on a second univariate analysis performed on the subgroup of patients who did not receive adjuvant treatment (HR, 3.2; 95% CI, 1.2–8.3, p = 0.016) (Table 4), but was not significant for risk of relapse on multivariate analysis performed for this low-risk subgroup of patients (HR, 2.47; 95% CI, 0.87–7.01, p = 0.08) (Table 5).
Univariate Analysis of Association Between Predictors of Disease-Free Survival and Overall Survival
Significant values.
CI, confidence interval; HR, hazard ratio; LVSI, lymph vascular space invasion.
Low-Risk Subgroup Univariate Analysis of Patients Without Adjuvant Treatment
Significant values.
Factors Associated with Patient Outcome on Multivariate Analysis
Significant values are in bold.
Discussion
Concerns remain that the introduction of a device into the endometrial cavity may cause disruption of endometrial cancer cells and affect patient's outcome. Available data are limited especially regarding the possible effect of the use of intrauterine manipulators on the long-term outcome. As a result, debates still take place in the gynecologic oncology community raising concern about the use of these devices.
Two previous studies have tried to analyze survival after laparoscopic surgery for endometrial cancer using a uterine manipulator. However, those were largely underpowered to investigate long-term outcomes (<70 patients included in each group). 9,10 In a multicenter study by the Italian society of gynecological endoscopy, authors reviewed data from 951 consecutive patients who underwent laparoscopic surgery for endometrial cancer with or without intrauterine manipulator. In this study, data regarding the effect of the manipulator on the rate of positive cytology and LVSI were not reported but results showed a nonsignificant difference in the recurrence rate (13.5% vs. 11.6%) between the manipulator and no manipulator groups. 11
Results of our study raise some safety concerns regarding the use of uterine manipulators during MIS for endometrial cancer. For the entire cohort, total recurrence rate was similar between the two comparison groups but with higher rates of local vaginal recurrence for patients in whom a uterine manipulator was used during surgery. After excluding patients who received adjuvant treatment (low-risk subgroup), the rate of vaginal vault recurrence and total recurrence was significantly higher with a worse DFS in the intrauterine manipulator group compared to the no manipulator group. However, the use of a uterine manipulator was not found to be a predictor of worse outcome on multivariate analysis that was performed for the entire cohort but was close to statistical significance when performed for the low-risk subgroup of patients who did not receive adjuvant treatment.
A multicenter study by the Spanish society of gynecology and obstetrics, followed over 2000 women with uterus confined endometrial cancer who underwent MIS and found, in concordance with the results presented here, that low-risk uterus-confined, Figo grade 1–2 endometrial cancer patients that were operated using a uterine manipulator had worse oncological outcome. 12 We can only assume that a neglectable number of patients received adjuvant treatment in this low-risk group of patients.
A possible explanation might be that local recurrence may be salvageable by either surgery or radiotherapy, with good long-term outcomes. 13 Following recurrence, most patients in our cohort were either operated or received radiotherapy with or without chemotherapy. This is also in accordance with the previously reported LAP2 study that found a potential increased risk of uterine cancer recurrence with manipulator-assisted laparoscopic hysterectomies compared to hysterectomies via laparotomy, but this risk was quantified and found to be small. 5 We can speculate that the effect of higher recurrence rates on long-term outcome of patients in the manipulator group, was eventually diluted by additional treatment modalities and that the presence of a uterine manipulator during surgery did not negatively affect the outcome of endometrial cancer patients on multivariate analysis.
Our results show that the use of an intrauterine manipulator in MIS for endometrial cancer was not associated with an increase in rates of LVSI; however, we found higher incidence of positive cytology in patients for whom a uterine manipulator was used during surgery. Previously published studies regarding LVSI and positive peritoneal cytology are conflicting, with some suggesting that the use of manipulators does not affect positive peritoneal cytology and/or LVSI, 14 –18 while other studies show an association between uterine manipulator use and positive peritoneal cytology and/or LVSI. 19,20 In the current study, LVSI was found in 27% of patients, which is in agreement previously published data.
With regard to positive cytology, we found that the rate of positive cytology was significantly higher in the group of patients who had an intrauterine manipulator. Positive cytology was an independent prognostic factor for both DFS and OS on univariate and multivariate analysis. Other reports showed similar results that peritoneal washings were significantly more likely to be positive in women in whom a uterine manipulator had been used. 19 –21 To elucidate whether the use of intrauterine manipulator increases the risk of positive cytology, its necessary to obtain cytology twice in the same individual, before and after the insertion of the intrauterine manipulator and compare them. In our study, cytology was taken after the insertion of the manipulator.
In concordance with the results presented in our study, a recently published, large meta-analysis of 18 studies (3 prospective studies, 13 retrospective studies, and 2 randomized controlled trials [RCTs]) investigated the influence of uterine manipulators on oncological outcomes in MIS of endometrial cancer. A positive association between malignant cytology and hysterectomies in which a uterine manipulator had been used in MIS were compared to open hysterectomies. The conclusion supports the use of uterine manipulators for minimally invasive treatment of endometrial cancer and found that the use of uterine manipulators does not increase the rate of recurrence and LVSI. 22
The current study offers several strengths; data were collected from a large cohort of patients who underwent surgery by a team of surgeons who share a joint surgical protocol and unified approach. This enhances the impact of the use of intrauterine manipulators and allows the current comparison. Moreover, in our study we were also able to perform a subgroup analysis that excludes the effect of adjuvant radiation treatment on the outcome measures. In addition, the follow-up time in our study is relatively long and was previously shown to include over 90% of recurrences from initial treatment. 23 However, this study is not without limitations including the inherent limitations that results from its retrospective nature. In addition, we did not perform coagulation of the tubes at the beginning of the procedure, and this might have an effect with regard to positive cytology.
Conclusions
Results of the current study show that the use of an intrauterine manipulator is associated with a minimal impact on the oncological outcomes of patient who undergo MIS and adjuvant treatment for endometrial cancer but may have implications on outcome for low-risk patients who do not receive adjuvant treatment.
Footnotes
Authors' Contributions
I.L.: Conceptualization, Methodology, Software, Validation, Formal analysis, Investigation, Resources, Data curation, Writing—original draft, Writing—review and editing, Visualization, Supervision, Project administration. N.M.: Methodology, Software, Validation, Formal analysis, Investigation, Data curation, Writing—original draft, Visualization. X.Z.: Resources, Investigation, Data curation, Writing—review and editing. S.S.: Resources, Investigation, Data curation, Writing—review and editing. S.L.: Resources, Investigation, Data curation, Writing—review and editing. L.G.: Resources, Investigation, Data curation, Writing—review and editing, Supervision. W.H.G.: Conceptualization, Methodology, Investigation, Resources, Data curation, Writing—original draft, Writing—review and editing, Supervision. R.K.: Conceptualization, Methodology, Validation, Formal analysis, Investigation, Data curation, Writing—original draft, Writing—review and editing, Visualization.
Ethics Approval
Ethical approval was waived by the local Ethics Committee in view of the retrospective nature of the study, and all the procedures being performed were part of the routine care.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This work was supported by grants from the Israel Cancer Research Fund and the Gloria's Girls.