
Abstract
Background:
Uterine cavity abnormalities contribute to infertility. The purpose of this study was to evaluate the incidence, recurrence rates, and risk factors for uterine cavity abnormalities in women undergoing infertility workup and treatment, focusing on the utility of routinely repeated imaging.
Methods:
Retrospective cohort study at single academic medical center of 833 infertile women who had uterine cavity evaluations performed at least 9 months apart.
Results:
Of 833 eligible patients, 664 (79.7%) had normal initial imaging and 169 (20.3%) had abnormal initial imaging. Among the former, 10% had abnormal uterine cavity on repeat saline infusion sonohysterography (SIS); among the latter, 32% had abnormal repeat SIS [Chi-square p < 0.0001, risk ratio 2.30 (95% confidence interval 1.85–2.86)]. On average, 23.1 ± 13.6 months passed between studies. Regardless of initial imaging findings, women with abnormal repeat SIS were older than those with normal repeat SIS, with no difference in time elapsed between studies. There were no associations between repeat imaging outcomes and body mass index, uterine instrumentation, number of treatment cycles, or maximum peak estradiol levels in a single cycle between studies. There was no difference in live birth rate among cycles started within 1 year after repeat SIS across groups.
Conclusions:
Uterine cavity abnormalities were found in 10% of patients on repeat imaging despite initially normal testing. No risk factors for cavity abnormality on repeat imaging were identified besides age and prior abnormality. It would be prudent to continue performing routine repeat uterine cavity evaluation for women undergoing fertility treatment, particularly if corrective measures had been taken in the past.
Introduction
Uterine cavity abnormalities are well known to contribute to infertility, accounting for up to 10% of cases of infertility. 1 Evaluation of the uterine cavity has always been an integral part of routine infertility workup. Different imaging modalities have been used in the evaluation of structural uterine abnormalities, including transvaginal ultrasonography, hysterosalpingography (HSG), saline infusion sonohysterography (SIS), and hysteroscopy. Compared to hysteroscopy as the gold standard in the diagnosis of uterine cavity abnormalities, HSG has been noted to be highly sensitive (98%) 2 and SIS has been found to be both highly sensitive (88%) and specific (94%). 3 The detection of uterine cavity abnormalities before undergoing fertility treatment cycles, particularly embryo transfer, allows for intervention to correct the abnormality, including septum and synechiae resection, polypectomy, and/or myomectomy. The correction of such abnormalities may lead to improved in-vitro fertilization (IVF) outcomes, including higher pregnancy and live birth rates. 4,5
Common clinical practice has evolved to perform not only an initial evaluation but also at least an annual evaluation of the uterine cavity before embryo transfer cycles. In some states, repeat testing is insurance mandated; however, little evidence exists to support this practice. Our literature review identified only one study that addressed the value of a repeat SIS in patients undergoing IVF or frozen embryo transfer (FET) cycles. 6
The purpose of our study is to determine the association between initial and repeat cavity evaluation results and to identify risk factors for abnormalities on a repeat test given an initially normal or abnormal cavity. We hypothesized that the presence or absence of uterine cavity abnormalities on initial imaging may predict findings on subsequent “annual” imaging in infertile patients.
Materials and Methods
Selection criteria
Institutional review board approval was obtained before the start of this study, and a waiver of informed consent was granted (Women and Infants Hospital IRB No. 18-0043).
All patients undergoing fertility treatment at the center where this study was conducted routinely undergo uterine cavity evaluation with an HSG and/or an SIS as part of standard workup of infertility. Per protocol and due to insurance requirements, all patients continuing or returning for treatment must undergo repeat cavity evaluation on an annual basis. Using billing codes, we identified all women who had an HSG and at least one SIS performed at our single, large academic institution between January 1, 2007 and December 31, 2017. Of these, we restricted the study population to women who had an SIS ordered by a reproductive endocrinology and infertility (REI) faculty member at the fertility center to identify women who were most likely undergoing continued fertility care at the center. Imaging studies had to be done at least 9 months apart to be considered as “annual” imaging done in anticipation of cycle starts that were at least 1 year from the prior cycle start.
Exclusion criteria were imaging performed without documentation of the results; repeat imaging being HSG alone or both HSG and SIS; no repeat imaging done; unclear infertility treatment history; imaging done for reasons besides infertility (e.g., abnormal uterine bleeding); and patients who underwent infertility treatment before 2007.
Characteristics of interest
The following parameters were chart abstracted for all patients: age; body mass index (BMI) at the time of both imaging studies; race and ethnicity; pregnancy history; smoking history; uterine instrumentation history before, in between, and after imaging; time between imaging studies; imaging results; fertility treatment cycle types and outcomes; peak estradiol levels and total gonadotropins used in each IVF cycle; and infertility diagnosis. Fertility treatment cycle types included natural cycle (unassisted conception or intrauterine insemination [IUI]); ovulation induction with oral agents (clomiphene citrate or letrozole) or injectable gonadotropins with or without IUI; IVF (any protocol); FET (natural or programmed); or donor recipient cycle. Uterine cavity abnormalities were defined as filling defects, synechiae, polyps, submucosal fibroids, and/or Müllerian anomalies (including septate, unicornuate, bicornuate, and didelphys uterus). If an abnormality was identified on HSG but follow-up initial SIS was found to be normal, the uterine cavity was considered to be normal.
Imaging technique
At our institution, HSGs were typically performed using standard fluoroscopic technique in the main radiology department with a trained radiologist taking the images. An REI faculty member typically performed the catheter insertion and contrast injection using a 5 French H/S balloon catheter (CooperSurgical).
SISs were typically performed either in the REI office or in the radiology suite in the standard manner using either a 5 French Soules Intrauterine Insemination Catheter (COOK Medical), Goldstein Sonohysterography Catheter (COOK Medical), or H/S balloon catheter (CooperSurgical) at the provider's discretion. All SISs were performed and read by REI faculty or performed by sonographers and read by radiologists who specialize in women's imaging in a stand-alone women's hospital.
If the initial imaging study was an HSG and a uterine cavity abnormality was identified, almost all patients had a follow-up SIS (often the same day).
Data abstraction
All chart reviews were performed by a single author (A.V.D.). Data were obtained from electronic chart review and a clinical database of all IVF cycles performed at the institution. Study data were collected and managed using Research Electronic Data Capture tools hosted at Women and Infants Hospital. 7,8
Statistical analysis
We examined patient characteristics and fertility-related care details among patients with initially normal imaging results and patients with initially abnormal imaging results. We first compared initial to repeat imaging results with a Chi-square test. Subsequent analyses were stratified by initial imaging result: normal or abnormal. In each stratum, characteristics of patients with repeat SIS normal versus abnormal were compared using Chi-square, t-test, or Wilcoxon Rank Sum test, as appropriate. Finally, we categorized patients based on the results of both imaging tests: 1st test normal—2nd test normal, 1st test normal—2nd test abnormal, 1st test abnormal—2nd test normal, or 1st test abnormal—2nd test abnormal, and compared fertility treatments and outcomes across groups using chi-square tests or Kruskal–Wallis tests. For each comparison, we conducted a complete case analysis. Deviations from the total sample size are noted in the tables. The SAS statistical software version 9.4 was used for all analyses (SAS Institute Inc., Cary, NC, USA).
Results
We evaluated 2252 women who had an SIS ordered by one of the REI faculty at the fertility center. After excluding patients who did not meet our inclusion criteria (Fig. 1), 833 general infertility patients qualified for the study and contributed chart-abstracted data.
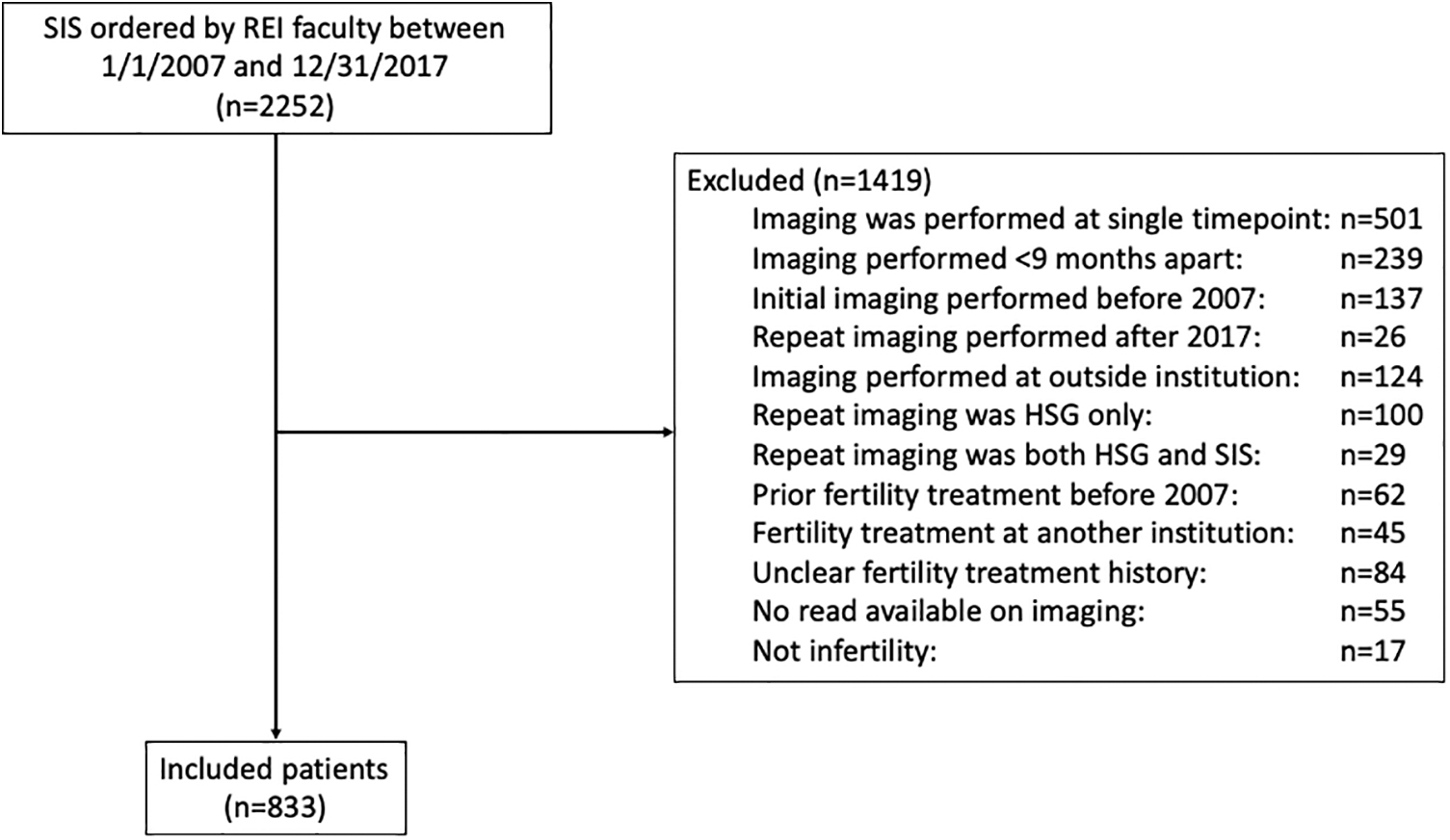
Flowchart of study population. HSG, hysterosalpingography; REI, reproductive endocrinology and infertility; SIS, saline infusion sonohysterography.
Baseline demographic characteristics are shown in Table 1. On average, 23.1 ± 13.6 months passed between imaging studies. If an abnormality was found on initial imaging, 47.3% of women underwent uterine instrumentation to correct the abnormality, with the majority of those being for endometrial polyps or fibroids (88.8%). Most patients (84.5% with initial test normal, 78.1% with initial test abnormal, 83.2% overall) had at least one fertility treatment cycle started between imaging studies, with 28.4% of those who had at least one documented pregnancy attempt between imaging studies achieving a live birth (29.2% with initial test normal and 25.0% with initial test abnormal).
Population Demographic Characteristics
Mean [SD] for continuous variables.
n (%) for categorical variables.
Median {range} for number of cycles overall and by type.
BMI, body mass index; IVF, in-vitro fertilization; MVA, manual vacuum aspiration; SD, standard deviation; SIS, saline infusion sonohysterography.
Our first objective was to identify the rate of uterine cavity abnormality on repeat imaging (Table 2). Of the 833 patients included in the study, 664 (79.7%) had normal initial imaging and 169 (20.3%) had abnormal initial imaging. Among the former, 10% had an abnormal uterine cavity on repeat SIS; among the latter, 32% had an abnormal repeat SIS [Chi-square p-value <0.0001, risk ratio (RR) 2.30 (95% confidence interval 1.85–2.86)].
Outcome of Repeat Saline Infusion Sonohysterography Stratified By Initial Imaging Result
Chi-square 39.01; p-value <0.0001.
We then identified risk factors for having an abnormality noted on repeat SIS stratified by first imaging result. As represented in Table 3, for both types of initial imaging findings, women with abnormal repeat SIS were older than those with a normal repeat SIS, although there was no difference in the time that elapsed between imaging studies in either stratum. Women with initially normal uterine cavity evaluation were more likely to have had a live birth in the interim if their repeat imaging was normal rather than abnormal (30.8% vs. 15.5%, p = 0.015). A similar trend was seen among women with an abnormal initial imaging, although it did not reach statistical significance (27.5% vs. 19.5%, p = 0.328). There was no association identified between repeat imaging outcomes and BMI, uterine instrumentation between imaging studies, total number of fertility treatment cycles [IVF, FET, ovulation induction, or natural cycle (timed intercourse or IUI)] performed between imaging studies, or the maximum peak estradiol levels.
Relationship Between Patient Characteristic and Abnormal Repeat Saline Infusion Sonohysterography, Stratified By Result of Initial Test
n (%) with p-value for chi-square for categorical patient characteristics.
Mean [SD] with p-value for t-test for continuous patient characteristics.
Median {range} with Wilcoxon Rank Sum test for number of cycles overall and by type.
Among the 169 patients who had abnormal initial imaging, a total of 256 different abnormalities were identified, reflecting that more than one abnormality could be present at a time. Of these, 230 were noncongenital abnormalities; 110 of these were specified as polyps (n = 77), submucosal fibroids (n = 18), or synechiae (n = 15); 24 were nonspecific fibroids; and 96 were documented just as filling defects. Among these, 29 (12.6%) recurred at the time of repeat imaging (e.g., polyp identified both at initial and repeat imaging). Notably, different abnormalities were identified at the time of repeat imaging (e.g., polyp at initial imaging and a submucosal fibroid at repeat) in 45 cases (19.6%).
Evaluating specific uterine cavity defects, among patients who had polyps identified on initial SIS/HSG and had subsequent uterine instrumentation (n = 57), 15 (26%) had a recurrence noted on repeat SIS. Among patients who had uterine instrumentation for submucosal fibroids identified on initial imaging (n = 18), one (6%) had a submucosal fibroid identified on repeat SIS. For synechiae that were taken down after initial identification, no recurrences were noted (0 of 8).
Finally, we evaluated patient outcomes after repeat imaging (Table 4). Of the 121 patients who had abnormal repeat imaging (67 Normal–Abnormal +54 Abnormal–Abnormal), 80 (66.1%) had uterine instrumentation subsequently performed with 68 (56.2%) having polyps and/or fibroids removed. This is compared to only 14 (2.0%) patients having uterine instrumentation performed after normal repeat imaging [n = 712 (597 Normal–Normal +115 Abnormal–Normal)]. Of note, among women who had normal initial imaging followed by abnormal repeat imaging (n = 67), 48 (71.6%) had subsequent uterine instrumentation to correct the identified pathology. There was no difference in live birth rate across groups (normal–normal, normal–abnormal, abnormal–normal, abnormal–abnormal initial-repeat imaging) among 739 patients who attempted conception in the 1st year after repeat imaging (p = 0.312).
Outcomes After the 2nd Saline Infusion Sonohysterography
n (%) for categorical variables with p-value for chi-square.
Median {range} with p-value for Kruskal–Wallis test by ranks for number of cycles overall and by type.
Discussion
In this study, we evaluate the utility of a repeat SIS in patients undergoing fertility treatment and identify risk factors for abnormality recurrence or the development of new abnormalities after an initially normal uterine cavity evaluation. We found that 10% of patients had abnormal uterine cavity on repeat imaging if their initial imaging was normal, compared to 32% who had abnormalities found on repeat imaging if their initial imaging was abnormal. The recurrence rate of specific abnormalities in this study was 12.6%. Regardless of initial imaging findings, women with abnormal repeat SIS were older than those with normal repeat SIS, although there was no difference in time elapsed between studies. There were no associations between repeat imaging outcomes and BMI, uterine instrumentation, total number of treatment cycles performed, maximum peak estradiol levels, or maximum total gonadotropins used in a single cycle between studies. There was no difference in live birth rate among cycles started within 1 year after repeat SIS across groups.
The overall rate of uterine cavity abnormalities identified in this study (20.3%) is concordant with prior published rates, which range from 11% to >35%. 9 –11 Although studies have evaluated the rate of uterine cavity abnormality recurrence after treatment in women with abnormal uterine bleeding, 12,13 very little has been published on this condition in the general infertility population.
Our data suggest that having an abnormality identified on initial imaging puts women at a greater than twofold higher risk (RR = 2.3) of having a uterine cavity abnormality seen again on repeat imaging at least 9 months later. However, even among women who had a normal initial cavity evaluation, one in ten will have an abnormality identified on repeat imaging. In the one other study that we identified in the literature that evaluated repeat uterine imaging, 11 of 36 patients (30.5%) who had a normal uterine evaluation in the past had a new finding on SIS. Seven of these patients had an intervention undertaken to correct the anomaly before embryo transfer. 6 Although our finding of 10% of patients having a new abnormality on repeat imaging is substantially lower than the 30.5% identified by Gera et al., 6 we believe that it remains clinically significant. We suspect that these represent de novo lesions that develop after an intervening pregnancy, simply over time (for over one third of study participants, the second imaging test occurred 2 years or more after the first test), or they could be due to false negative results on the initial imaging.
As reviewed by Seshadri et al., the detection of intrauterine lesions by SIS in infertile women has the following test characteristics depending on the study: sensitivity 75%–100%; specificity 40%–100%; positive predictive value (65%–100%); and negative predictive value 77%–100%. 14 The test characteristics of HSG are also variable compared to hysteroscopy, generally with better sensitivity (60%–98%) than specificity (15%–80%). 15 Given the high rate of false positives on HSGs is why our institutional protocol is to perform an SIS for any abnormal HSG to confirm the findings before considering taking the patient to the operating room for an operative hysteroscopy.
It is notable that less than half (47.3%) of women who were found to have an abnormality on initial imaging underwent uterine instrumentation to correct the identified abnormality. Patients did not undergo corrective surgery for a variety of reasons, including unassisted pregnancy before intervention, abnormality felt not to be clinically significant by the REI provider, and patient preference to attempt conception before instrumentation.
Although our data identified that women with abnormal repeat cavity evaluations tended to be 1.3–1.7 years older than those with normal uterine cavities, this finding is likely not clinically significant enough to risk-stratify by age when considering whether a patient should have a repeat uterine cavity evaluation performed.
The finding that women with normal repeat imaging tended to be more likely to have a live birth between studies than their counterparts with abnormal uterine cavities on repeat imaging suggests the de novo development of abnormalities or the possibility that an abnormality may have been missed on initial cavity evaluation, understanding that even in the most experienced hands false negatives are possible.
This study contributes to sparse literature on the utility of uterine cavity re-evaluation in the workup and management of infertility. All imaging studies were either performed and read by REI faculty or performed by sonographers and read by radiologists who specialize in women's imaging in a stand-alone women's hospital. As ultrasound imaging is highly operator dependent, the performance of imaging by highly-specialized providers in this institution decreases the chance that abnormalities were missed or that there were false positives due to operator performance. Similarly, the use of institutional protocols for ovarian stimulation decreases the potential for variability in clinical practice affecting outcomes.
Nevertheless, our study is limited by its retrospective nature. Some patients underwent uterine instrumentation based on uterine cavity abnormalities that were identified during routine follicle scans during ovarian stimulation; these findings were not able to be accounted for with the design of this study. The time between scans varied considerably, with hypothesized contributing factors, including whether pregnancy was achieved after the first imaging study, insurance status, and the time when a subsequent pregnancy was desired. Therefore, while this study addresses the utility of repeat imaging during continued fertility care, the findings are not able to suggest the duration of time after which repeat imaging is recommended.
Furthermore, while we do not have pathologic confirmation of the hysteroscopic findings to correlate with SIS findings, ultimately removal of any lesion demonstrates that the cavity evaluation was prudent. While a randomized controlled trial could be designed to evaluate if repeat uterine cavity is necessary, it is unlikely that such work is ethically plausible given the relatively high rate of new abnormality identification of 10% that we identified in this study.
Conclusions
Based on the results of this study, we believe that it would be prudent to continue performing repeat uterine cavity evaluation for women undergoing fertility treatment cycles. This is particularly true in women who have a history of an abnormality identified on their initial imaging, and we believe that most clinicians would feel that 10% is a high enough rate of new abnormality identification to warrant follow-up imaging even in women with normal uterine cavities on initial workup.
Footnotes
Authors' Contributions
Andrey V Dolinko: conceptualization; methodology; formal analysis; investigation; writing—original draft; writing—review & editing; visualization; project administration. Valery A Danilack: methodology; formal analysis; writing—review & editing; visualization. Ruben J Alvero: conceptualization; methodology; writing—review & editing; supervision. Victoria V Snegovskikh: writing—conceptualization; review & editing; supervision.
Author Disclosure Statement
The authors have no competing interests to declare that are relevant to the content of this article.
Funding Information
V.A.D. effort was supported by Agency for Health care Research and Quality. “Comparative effectiveness of interventions for labor induction.” (1K01HS025013 [Danilack]) 9/2016–5/2021.