
Abstract
Background:
Severe perineal lacerations (SPLs), common worldwide, are associated with short- and long-term complications: pelvic floor disorders, fecal incontinence, fistula, and profound psychological impacts. Limited research suggests that experiencing SPL may influence future reproductive intentions, but research on outcomes is lacking.
Methods:
We analyzed the effect of experiencing SPL during a first delivery among a large cohort of Swedish births between 1992 and 2013. We used linear and multinomial logistic regression to estimate the associations between SPL and four reproductive outcomes: subsequent total birth number, probability of a second birth, interpregnancy interval (IPI), and subsequent scheduled cesarean birth.
Results:
Among 947,035 singleton live-born first-births, we found that experiencing SPL was associated with slightly fewer overall births in fully adjusted models (a decrease of −0.020 births; 95% confidence interval [CI]: −0.028 to −0.012), but no difference in the probability of a second birth (risk ratio [RR]: 1.00; 95% CI: 0.99 to 1.00) or IPI. Scheduled cesarean was increased in births after SPL (adjusted RR: 4.57; 95% CI: 4.42 to 4.73). A secondary comparison of SPL to severe postpartum hemorrhage suggests that some of these observed differences may be related to experiencing any severe outcome, and some specifically to perineum disruption.
Conclusion:
This study provides a deeper understanding of the long-term impacts of SPL, which may be useful in informing best clinical practices for supporting women who have experienced SPL.
Introduction
Worldwide, severe perineal lacerations (SPLs) are among the most common maternal morbidities, experienced by ∼3%–5% of women who deliver vaginally. 1 SPLs are third or fourth degree tears which involve disruption of the perineum, anal sphincter (third), and rectal mucosa (fourth). SPL are associated with both short- and long-term physiologic complications: pelvic floor disorders, fecal urgency and incontinence, rectovaginal fistulas, and risk of recurrent injury in subsequent deliveries. 1 –3 Experiencing SPL can also have profound psychological impact and personal meaning, as it affects a woman's well-being, sexual function, and mental health. 4 –6 Women who have experienced SPL report physical and psychological problems, difficulty re-establishing a sexual life, increased worries for their future health and pregnancies, and wishes to postpone or abandon plans for a second child. 4 –6
Scant research explores how these physiological and psychological consequences may be associated with a woman's later reproductive course and birth outcomes. While a small body of research suggests that experiencing trauma during delivery may influence a woman's future reproductive desires and intentions, there is limited information on how these intentions translate to outcomes. 4,6 –11 One large study found that among Swedish women who had a third or fourth degree perineal laceration during their first delivery, only 68% went on to have their expected second births. 12
However, another study found that despite reporting a wish to abandon plans for more than one child, Swedish women who sustained a complete anal sphincter rupture (i.e., fourth degree laceration) had the same likelihood of having a second delivery as matched cesarean section and vaginal delivery controls with no severe laceration. 6 Another Australian study found that women experiencing SPL were less likely to have a subsequent birth (10% decreased odds), but those who did were not less likely to deliver vaginally. 13
We set out to characterize the effect of experiencing SPL during a first delivery on subsequent reproductive outcomes, including total number of births and interpregnancy interval (IPI). To address the multiple mechanisms through which subsequent reproductive outcomes may be impacted, we utilized a nation-wide population-based cohort of Swedish women. We compared subsequent reproductive outcomes among women with SPL in their first delivery to women in two distinct comparator groups: (A) women without SPL and to (B) women without SPL but who did have another potentially traumatic childbirth experience, severe postpartum hemorrhage (PPH). 8 We hypothesized that women who experienced SPL may have fewer overall children, longer IPIs, and an increased frequency of planned cesarean delivery during subsequent pregnancies compared with women who did not experience SPL, but that their subsequent reproductive outcomes would be similar to those of women who experienced a severe PPH.
Methods
Data sources
This study was based on prospectively collected data from the nationwide Swedish Medical Birth Register (MBR), which includes more than 98% of births in Sweden since 1973. 14 The MBR includes information collected in early pregnancy on demographic data, reproductive and medical history, and information from the pregnancy, delivery, and neonatal period. Data were linked to other national population-based registers using the person-unique identification number assigned to each citizen at birth or immigration to Sweden. 15 Information on maternal country of birth, highest level of maternal education at first birth, and date of death were retrieved from the Total Population Register, Education Register, and Cause of Death Register, respectively. 16 This study was approved by the Regional Ethics Review Board No. 4 in Stockholm, Sweden: 2008/1182-31/4. Institutional Review Board approval was waived by Oregon Health and Science University.
Study population
Between January 1, 1992, and December 31, 2013, there were 947,035 singleton live-born first-births recorded in the MBR (Fig. 1). We excluded first births with missing infant identification number, sex, or gestational age at birth. Exposure status was defined relative to the woman's first birth (i.e., the index birth); outcomes related to characteristics of subsequent births. In an effort to isolate any potential impact of SPL-related trauma in first birth on future fertility from trauma due to preterm birth or fetal losses, we also excluded first birth stillbirths, births with major malformations, and births that occurred before 37 weeks gestation (preterm birth). We further excluded nonvertex or missing presentation, and to only include first births occurring vaginally (and therefore at risk for SPL), we excluded those delivered via cesarean section.
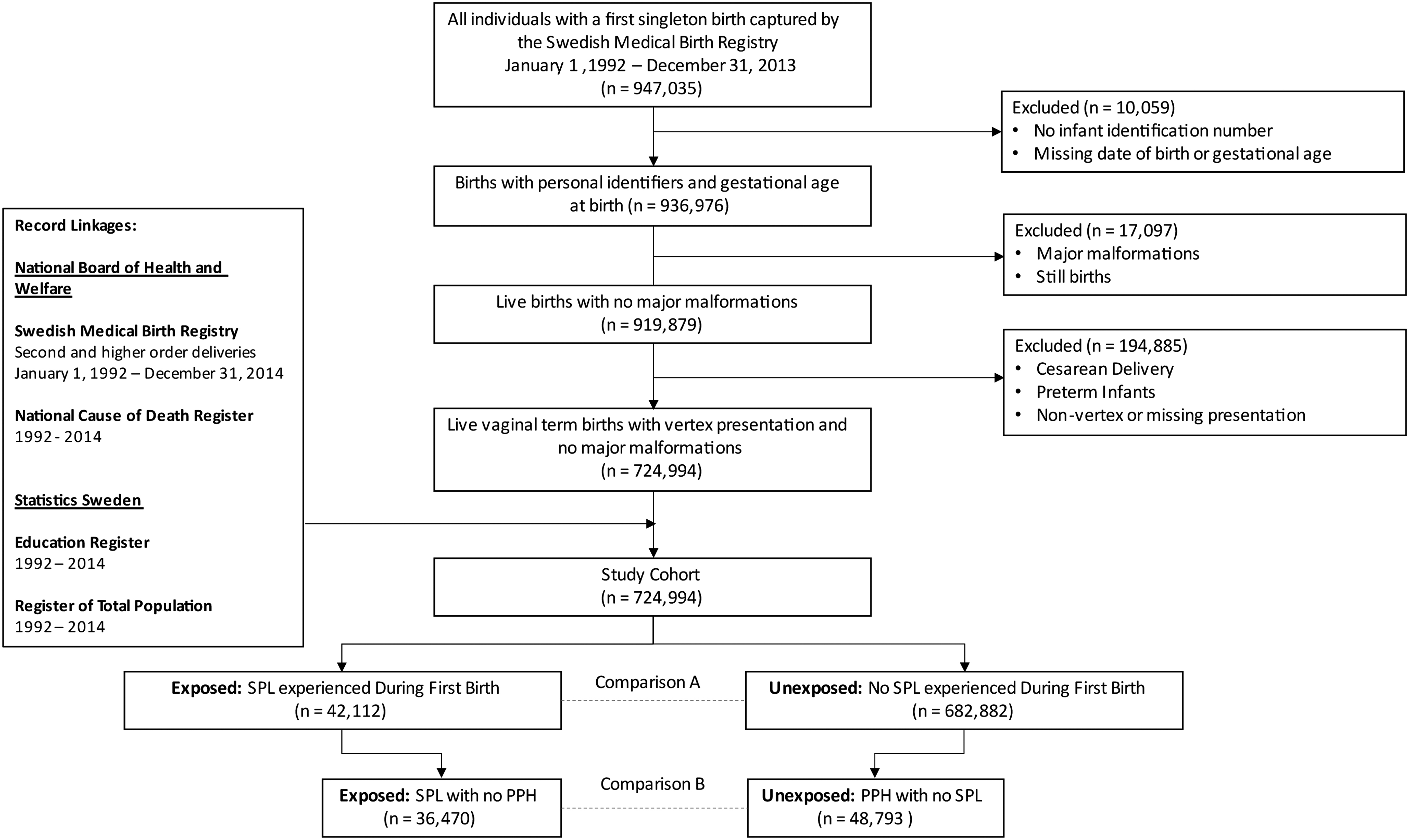
Flowchart of the Study Cohort of 724,994 primiparous women with term, singleton, vaginal births in vertex presentation, 1992–2013. PPH, postpartum hemorrhage; SPL, severe perineal laceration.
Our final study cohort included 724,994 women whose first birth occurred during the study period; these women were followed in the registries described above until December 31, 2014 (a range of 1–21 years).
Exposures and comparison groups
SPL was defined as a third or fourth degree tear, classified by diagnosis at discharge from the delivery hospital according to the Swedish version of the International Classification of Diseases, Ninth and Tenth Revisions (ICD-9 and ICD-10, respectively). SPL was classified by the ICD-10 (ICD-9) codes O70.2, O70.2A/C, O70.2B/D, O70.2E, and O70.2X (664C) for perineal rupture degree 3 and the codes O70.3 (664D) for perineal rupture degree 4. Severe PPH was identified using ICD-10 (ICD-9) code O72 (666), which corresponded to postpartum bleeding of over 1,000 mL throughout the entire study period. 17
SPLs may affect future reproductive outcomes through several heterogeneous mechanisms, including physiologic concerns about integrity of the perineum during future childbearing and psychological trauma due to the experience. We therefore chose two distinct comparator groups for analysis of SPL effects: Comparison A and Comparison B (Fig. 1). The exposed group in Comparison A included all women in the study population who experienced a SPL in their first delivery. The unexposed group included all women in the study population who did not experience a SPL in their first delivery.
While Comparison A assessed potential effects of SPL through all mechanisms, Comparison B was restricted to women with some severe/potentially traumatic childbirth experience during their first birth, focusing specifically on the potential effects of perineal trauma compared to other severe childbirth experiences. The exposed group in Comparison B included all women in the study population who experienced a SPL without a severe PPH in their first delivery (i.e., only SPL). The unexposed group in Comparison B included all women in the study population who experienced severe PPH in the absence of a SPL (i.e., a severe PPH without SPL).
Outcomes
We included four separate subsequent reproductive outcomes in this analysis: (1) total number of subsequent births, (2) proportion of women having a second birth, (3) IPI between first and second birth, and (4) scheduled cesarean section in second birth. All subsequent reproductive outcomes were based on live births recorded in the MBR during 1992–2014.
To assess the impact that experiencing SPL has on overall future reproductive plans, we chose total number of births recorded in the MBR during 1992–2014 as our first outcome, and the number of women who have a second birth as our second. It is possible that experiencing an SPL might delay a woman's subsequent childbearing, so our third outcome was IPI among women who had a second birth during the study period. IPI was quantified as the number of years between first delivery and best estimation of first day of last menstrual period of the second pregnancy that resulted in a birth during the study period. Best estimate was based on (1) first or second trimester ultrasound, (2) first day of last menstrual period, and (3) clinical evaluation. 18
The fourth outcome, scheduled cesarean in the second birth, was chosen as an outcome that we would expect to be strongly associated with SPL a priori, thus providing a logic check for the other associations between SPL and our other three outcomes. Scheduled cesarean was derived from birth register data from the second birth.
Covariates
We considered an array of maternal prepregnancy characteristics, pregnancy- and health-related characteristics, and variables related to labor and delivery in the first pregnancy retrieved from the MBR as tick-boxes, registered variables, or ICD-10 codes. Covariates were chosen a priori based on causal diagrams and on availability in the register data. 16,19 Maternal prepregnancy characteristics included maternal age at first birth (12–24 years, 25–29 years, 30–34 years, and 35–50 years), maternal country of birth (Swedish, African, Asian, other), and body mass index (BMI) at first prenatal visit (underweight, BMI <18.5 kg/m2; normal weight, BMI = 18.5–24.9 kg/m2; overweight, BMI = 25–29.9 kg/m2; and obese, BMI ≥30 kg/m2).
Maternal pregnancy-related health characteristics included smoking level during the first trimester (none, <10 cigarettes/day, ≥10 cigarettes/day), pregestational diabetes (types I and II), gestational diabetes, chronic hypertension, and preeclampsia. Labor and delivery characteristics included birthweight (<4,000 g, ≥4,000 g), infant head circumference (<35 cm, ≥35 cm), mode of delivery (vaginal spontaneous, vacuum extraction/forceps), prolonged duration of labor, and episiotomy (Supplementary Table S1 and Table 1).
Maternal, Infant, and Delivery Characteristics of the Study Cohort of 724,994 Primiparous Women with Term Vaginal Births in Vertex Presentation, by Severe Perineal Laceration Exposure Status, 1992–2013
164,184 (22.7%) of women were missing data on one or more maternal, infant, or delivery characteristics.
SPLs, severe perineal lacerations.
Analysis
We characterized the cohort by cross tabulating each potential confounder by each comparison group. For all analyses, we conducted separate analysis for Comparison A (SPL vs. no SPL) and Comparison B (SPL without PPH vs. PPH without SPL). For unadjusted analysis of first three outcomes, total number of live births, total number of second births, and IPI among women who had second births, we compared unadjusted means and standard deviations (SDs) using Student's t-test for each comparison. For our fourth outcome, scheduled CS in the second pregnancy, we estimated unadjusted risk ratios (RRs) and 95% confidence intervals (CIs) for each comparison using logistic regression. In this analysis, we excluded women with no information on onset of second delivery (n = 2,304).
We then used linear and multinomial logistic regression analyses to estimate the adjusted association between SPL and each of our four outcomes. We constructed three iterative multivariable models for each outcome, progressively adjusting for additional confounders in each subsequent model: (1) maternal prepregnancy characteristics (age, country of birth, and BMI), (2) maternal prepregnancy characteristics and maternal pregnancy-related health characteristics (smoking, pregestational and gestational diabetes, chronic hypertension, and preeclampsia), and (3) maternal prepregnancy characteristics, maternal pregnancy-related health characteristics, and delivery characteristics (birthweight, infant head circumference, mode of delivery, prolonged duration of labor, and episiotomy). Missing covariate data were imputed using fully conditional single-chained imputation with mean values: the logistic function was used for binary covariates, the discriminate function for ordinal covariates, and the linear model for continuous covariates. Analyses were conducted in SAS version 9.4 (SAS Institute, Carey, NC).
Results
This cohort comprised 724,994 primiparous women with term, singleton, vaginal births with no major malformations, and vertex presentation during 1992–2013 (Fig. 1). In the cohort, a total of 42,112 (5.8%) women experienced a SPL during the index birth, 54,435 (7.5%) experienced severe PPH, 36,470 (5.0%) experienced SPL and no PPH, and 48,793 (6.7%) experienced PPH and no SPL. A second birth was recorded in the MBR during 1992–2014 for 529,553 (73.0%) of the cohort. This included 381,579 (52.6%) who only had a second birth recorded, and 147,971 (20.4%) with a second birth and higher order births included (range = 3–14).
Comparison group A
Compared to women who did not experience SPL, a higher proportion of women who experienced SPL were 35–50 years old at delivery (9.9% vs. 7.9%), born outside of Sweden, and did not smoke during early pregnancy (Table 1). Women who experienced SPL were more likely to have diabetes (types I and II, or gestational), and less likely to be diagnosed with preeclampsia. Infants whose delivery resulted in SPL were more likely to weigh ≥4,000 g (27.2% vs. 13.5%) and have a head circumference ≥35 cm (69.3% vs. 55.9%). Compared to women who did not experience SPL, women who experienced SPL were more likely to have an instrumental vaginal delivery, prolonged labor, or an episiotomy.
Women who experienced SPL in their first delivery had an average of 1.93 (SD = 0.76) births during the study period, compared to 1.99 (SD = 0.83) among women who did not (p < 0.001; Table 2). Compared with women who did not experience SPL, women who experienced SPL had fewer overall births (β = −0.061, p < 0.001). This association was attenuated in the full adjusted model, but remained significant (aβ = −0.020, p < 0.001; Table 3). A smaller proportion of women who experienced SPL had a second delivery (72.2%), compared to women who did not experience SPL (73.1%) (RR = 0.99, p < 0.001). The fully adjusted model indicated no association (adjusted risk ratio [aRR] = 1.00, p = 0.71).
Reproductive Outcome Distributions During Follow-Up (1992–2014) Among Women Who Had First Births Captured by the Swedish Medical Birth Register During 1992–2013, by Severe Perineal Laceration and Postpartum Hemorrhage Exposure Status
IPI (years).
Proportion among women who go on to multiparous.
IPI, interpregnancy interval; PPH, postpartum hemorrhage; SD, standard deviation.
Reproductive Outcomes (Comparison A) Among Women Who Experienced Severe Perineal Lacerations During Their First Birth, Compared with Women Who Did Not Experience Severe Perineal Laceration in the Study Cohort of 724,994 Women, 1992–2014
Labor Onset analysis only completed for records that included delivery mode for second birth.
Adjusted for maternal age, maternal country of birth, BMI at first prenatal visit.
Adjusted for Model 1 covariates+smoking during the first trimester, diabetes (gestational+pregestational), chronic hypertension, preeclampsia.
Adjusted for Model 1+Model 2 covariates+birthweight, head circumference, prolonged delivery, episiotomy, mode of delivery.
BMI, body mass index; CI, confidence interval; RR, risk ratio.
Among women who had a second delivery, the average IPI between birth and second conception was 2.29 (SD = 1.66) years for women who experienced SPL during their first delivery, compared to 2.37 (SD = 1.90) years for women who did not (p < 0.001; Table 2). Compared with women who did not experience SPL, women who experienced SPL had a shorter IPI (β = −0.085, p < 0.001; Table 3). This association did not achieve statistical significance in the final adjusted model (aβ = 0.016, p = 0.14).
Among the second births in Comparison A, 20,853 (2.88%) women delivered by a scheduled cesarean (Table 2). Compared with women who did not experience SPL, women who experienced SPL during their first delivery had 5.59 (95% CI: 5.43 to 5.75) times the risk of delivering their second child via scheduled cesarean (Table 3). This association was attenuated in the fully adjusted model but remained strong (aRR = 4.57; 95% CI: 4.42 to 4.73; Table 3).
Comparison group B
Compared to women who experienced PPH without SPL, a higher proportion of women who experienced SPL without PPH were <35 years old at delivery, had more than 12 years of education, and were born outside of Sweden (Supplementary Table S2). Infants whose delivery resulted in severe tearing were more likely to have a head circumference ≥35 cm. Compared to women who experienced PPH without SPL, women who experienced SPL without PPH were more likely to have an instrumental vaginal delivery, prolonged labor, or an episiotomy (Table 4).
Reproductive Outcomes (Comparison B) Among Women Who Experienced Severe Perineal Lacerations Without Postpartum Hemorrhage During Their First Birth, Compared with Women Who Experienced Postpartum Hemorrhage Without Severe Perineal Laceration, in the Study Cohort of 724,994 Women, 1992–2014
Labor Onset analysis only completed for records that included delivery mode for second birth.
Adjusted for maternal age, maternal country of birth, BMI at first prenatal visit.
Adjusted for Model 1 covariates+smoking during the first trimester, diabetes (gestational+pregestational), chronic hypertension, preeclampsia.
Adjusted for Model 1+Model 2 covariates+birthweight, head circumference, prolonged delivery, episiotomy, mode of delivery.
Results between Comparison A and Comparison B were broadly similar, although the magnitude of the differences between the SPL and referent group did vary slightly. Women who experienced SPL without PPH in their first delivery had an average of 1.93 (SD = 0.76) births during the study period, compared to 1.96 (SD = 0.81) births among women who experienced PPH without SPL (p < 0.001; Table 2). A similar proportion of women who experienced SPL without PPH (72.5%) and women who experienced PPH without SPL (72.2%) had a second delivery in the study period (RR = 1.00, p = 0.33; aRR = 1.00, p = 0.11).
For women in Comparison B who had a second birth, the average IPI between first birth and second conception was 2.29 (SD = 1.66) years among women who experienced SPL without PPH during their first delivery, compared to 2.37 (SD = 1.89) years among women who experienced PPH exclusively (p < 0.001; Table 2). Compared with women who experienced PPH without SPL, women who experienced SPL without PPH had a shorter IPI (β = −0.085, p < 0.001; Table 4). This association was attenuated in the full adjusted model (aβ = −0.033, p = 0.03).
Among the second births in Comparison B, 6,131 (10.0%) women delivered by a scheduled cesarean. Compared with women who experienced PPH without SPL, women who experienced SPL without PPH during their first delivery had 3.26 (95% CI: 3.09 to 3.43) times the risk of delivering their second child via scheduled cesarean (aRR = 2.97; 95% CI: 2.80 to 3.15).
Discussion
In this large Swedish population-based cohort study, women who experienced SPL at the time of their first birth had slightly fewer overall births. Notably, the difference in the total number of births was evident when comparing women with SPL to all women without (Comparison A), but no difference was detected when comparing these women to those who sustained another severe birth outcome (severe PPH, Comparison B). Our results provided some moderate support for our hypothesis that experiencing SPL would be associated with fewer overall births, although we can and should consider these results in light of the modest effect size.
The difference in total number of births between women who experienced an SPL and those who did not was very small in absolute terms (−0.020 births) as well as relative terms (a decrease in ∼1%, as a fraction of the average number of later births in our study population). While this difference of ∼470 births per year may not be notable at the population level, even a small significant difference can be of clinical importance for individuals—especially when considered alongside other factors that drive reproductive decisions and outcomes.
In contrast to our hypothesis that second pregnancies would be less frequent after SPL, we found no association between SPL and probability of having a second birth during the study period. While prior research found that women who experienced SPL had a significantly decreased likelihood of delivering a second birth, these studies did not adjust for maternal or delivery characteristics. 12,13 Our findings instead support results by a smaller study that found that even though women who experienced SPL indicated that they were unlikely to have a second child—their postbirth preferences were not reflected in actual reproductive outcomes. 6 We also expected a longer IPI among women who experienced SPL (compared to women without SPL) who go on to be multiparous, but our findings do not support this hypothesis.
The crude association between SPL and a shorter IPI disappeared when adjusting for confounders when comparing to all women without SPL, but a shorter IPI remained significant after adjustment when comparing to women with severe PPH. This could partially be explained by the fact that women in the SPL group were older than those in either comparison group and therefore more likely to have a shorter IPI. 20
There are multiple mechanisms through which SPL may affect a woman's future reproductive intentions and outcomes. These include concerns specifically about the pelvic floor and anogenital region, as well as the psychological impact of trauma. 4,6,7,9,12,21 The fear of new tears and ending up in a similar situation could possibly be addressed by a scheduled cesarean in second birth. As expected, scheduled cesarean in second birth was increased fivefold in women who experience SPL during their first delivery. This corresponds to clinical practice in Sweden, where women who have experienced a SPL and have persistent pelvic floor dysfunction are generally recommended a scheduled cesarean (although all women with a previous SPL without dysfunction also have the right to discuss planned mode of delivery with a midwife or obstetrician before and during subsequent pregnancy).
When considering how results changed when utilizing a different comparison group experiencing a different severe birth outcome (PPH, one without perineal etiology), there is evidence that some of the differences observed in our main findings may be related to both experience of a severe outcome and experience of an outcome that specifically relates to disruption of the perineum. For example, our finding of a moderately decreased total number of births between women with SPL and women without (1.93 vs. 1.99) was not evident when comparing women with SPL to women with PPH.
Similarly, the magnitude of increase in scheduled cesarean was diminished when PPH was the comparison group (suggesting that some of the SPL-related increase was related to more generalized negative outcomes in the first birth), but a large and significant SPL-related increase remained even when comparing to first births with PPH. This is logical in that a scheduled cesarean avoids the risk of repeat SPL but not of PPH in the same way, and this finding suggests that some of the increase in scheduled cesarean relates specifically to the outcome of SPL and not to the general experience of sustaining a severe birth outcome.
Our findings add to the small but growing body of literature on how serious maternal complications affect future reproductive intentions and impacts. Prior research has documented that women who experience a blood transfusion, cesarean section, or severe maternal morbidity (SMM) are less likely to have a second birth. 8,10,11,22 Our prospective cohort study, which is based on a large, national, population-based sample, has some contributions that make it novel compared to other work. This includes an extended follow-up time, multiple comparison groups, and adjustment for relevant maternal and delivery characteristics. Notably, much current research on maternal health focuses on SMM, a composite metric with some notable strengths from a research and quality improvement perspective. 23
However, SMM does not include all complications that pregnant women experience as being serious (being restricted to life-threatening events on par with organ failure). As such, there is a need for research on specific complications—both SMM-defining conditions and other maternal complications—and their impact on long-term maternal health.
The large size of the study over a time-period of 22 years enabled us to follow-up the reproductive course of primiparous women with and without SPL, thus attempting to parse out potential impact of a specific serious outcome (i.e., SPL) compared to more general impacts of experiencing any serious maternal outcome. Although a focus on SMM enables population-wide comparisons of maternal outcomes that are more common than maternal death, its heterogeneity means that specific downstream causal impacts of SMM are difficult to parse out by definition. The effect of a stroke during labor is different from the impact of a blood transfusion or a hysterectomy. By focusing on one outcome, we sought to narrow down the etiological heterogeneity and provide more evidence on this under-studied outcome.
Finally, due to the fine-grained data in the MBR and linkage to other national registers, we were able to adjust for several important confounders that other studies which examined subsequent birth outcomes following SPL did not account for. 12,13
However, our study is not without limitations. While we had access to comprehensive records of the pregnancy, delivery, and neonatal period for each birth included in the study, we did not have access to information on long-term pelvic floor dysfunction or medical interventions after the experience of SPL, both of which could act as potential mediators on the study outcomes. In addition, different clinical practices regarding scheduled cesarean section after a previous SPL, either over the course of the study period or between facilities, could have influenced the effect estimates for the cesarean outcome.
Further, severity of perineal lacerations can be difficult to classify, leading to a potential misclassification of the exposure, specifically between second- and third-degree perineal lacerations. While a quality assessment of the MBR found that the validity of the diagnoses of the most common maternal complications during pregnancy is good, there has been no specific assessment of SPL diagnoses, and underreporting or misclassification may exist. 14 In addition, the external validity of these results could be hampered when generalizing to settings where childbirth care is not delivered free of charge within national health care coverage, for example by introducing financial incentives for obstetric procedures. 24
Maternal health is a national and global priority, and experiences during childbirth can profoundly affect maternal psychological and physical short- and long-term wellbeing. The awareness of perineal injuries has risen the last decades, but research is still broadly lacking. In Sweden, the Swedish Agency for Health Technology assessment and assessment of social services emphasizes a focus on this outcome and especially on prevention, detection, and treatment of different symptoms related to perineal injuries. 25 However, with some notable exceptions (e.g., incontinence), the long-term sequelae of SPL remain understudied, despite the fact that this is among the most common complications sustained during childbirth.
A more nuanced and precise understanding of any long-term impacts of SPL is required to continue to achieve improvement in maternal health around the globe. SPL has been shown to negatively affect maternal, mental, and physical health shortly after birth, our study adds evidence that the long-term impacts may be limited in this setting. A deeper understanding of how SPL affects a woman's future childbearing may be useful in informing best practices for maternity care. Enhanced efforts should be made in the clinical setting to support women who have experienced SPL and engage them to discuss their sexual/reproductive health, including future reproductive plans.
Footnotes
Authors' Contributions
A.N-.K.: Conceptualization, Software, Formal Analysis, Writing—Original Draft, and Visualization. A.S.: Conceptualization, Methodology, Software, Formal Analysis, Data Curation, and Writing—Original Draft. A-.K.W.: Writing—Review and Editing. O.S.: Writing—Review and Editing. J.M.S.: Conceptualization, Methodology, Writing—Original Draft, Writing—Review and Editing, and Supervision.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.
Supplementary Material
Supplementary Table S1
Supplementary Table S2
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.