
Abstract
Background:
The levels of oxidative stress and proinflammatory factors in perimenopausal females increased, and they were also deeply troubled by insomnia. The occurrence of insomnia is related to the changes of oxidative stress and inflammation levels in the body. Perimenopausal insomnia may be related to mild systemic inflammation, and oxidative stress can promote chronic inflammation. However, the underlying mechanism behind the phenomenon is still unclear.
Objective:
The aim was to investigate whether the occurrence of perimenopausal insomnia disorder is related to higher levels of oxidative stress and inflammation in the body, and to explore the role of inducible nitric oxide synthase (iNOS) in perimenopausal insomnia.
Methods:
A total of 127 perimenopausal participants were recruited in this study. Participants with global scores of the Pittsburgh sleep quality index (PSQI) >7 were diagnosed with insomnia (n = 54). The patient health questionnaire-9 (PHQ-9) and generalized anxiety disorder-7 (GAD-7) were evaluated, and sociodemographic data were obtained. The serum concentrations of iNOS, interleukin 6 (IL6), and tumor necrosis factor α (TNFα) were measured using commercial assays.
Results:
In the insomnia group, IL6 levels were positively correlated with scores of component 5 and component 7 of PSQI, respectively. PHQ-9 and GAD-7 were positively correlated with the global score of PSQI component 7 and PSQI, respectively; PHQ-9 was positively correlated with the global score of PSQI component 1. Finally, PHQ-9, iNOS, and IL6 were found to be independent predictors of perimenopausal insomnia using logistic regression.
Conclusions:
Moderate oxidative stress caused by a certain concentration of iNOS plays a protective role in perimenopausal insomnia, while proinflammation and depression are potential risk factors.
Introduction
Current evidence suggests that 59% of American perimenopausal females have insomnia, while the incidence is much higher in China (65.86%) and India (67%). 1 The previous study has reported numerous factors associated with insomnia during perimenopause, including hot flashes, anxiety and depression, other medical conditions, behavioral and psychosocial factors, and primitive sleep patterns. 2 Insomnia of perimenopausal females is more severe and lasts longer than that of nonmenopausal females. 3 With females entering the perimenopausal period, the risks of anxiety and depression increase significantly. 4
During perimenopause, females with mood disorders, particularly anxiety and depression, may experience insomnia manifested as difficulty falling asleep and early awakening. 5 The other manifestations of insomnia include increased wakefulness in the night, early waking in the morning and inability to fall asleep again after waking up, shortened total sleep time, and poor sleep efficiency and quality, 6,7 which has been linked to the occurrence and development of many chronic diseases, such as metabolic and neuropsychiatric disorders. 8 Although insomnia during perimenopause has become a research hotspot in recent years, the underlying mechanisms remain largely unclear.
Animal experiments showed that inducible nitric oxide synthase (iNOS) inhibitor injection could suppress rapid-eye-movement sleep (REMS) during the sleep cycle and induce delayed enhancement in slow-wave sleep (SWS) in old rats, 9 suggesting that iNOS may play a key role in maintaining sleep. Nitric oxide (NO) produced by iNOS plays an important role in sleep–wake regulation. 10 A previous study found that decreased NO promotes wakefulness, while increased NO promotes sleep. 11 An increasing body of evidence suggests that perimenopausal estrogen deficiency may induce iNOS expression in the vasculature, which could increase the NO concentrations. 12,13 However, perimenopause is also reported to be a time of significant insomnia.
Other studies have pointed out that excessive NO interacts with superoxide anion to form oxidants and cytotoxic peroxynitrite anion, which causes oxidative stress. 14 An animal study showed that reducing oxidative stress in neurons of wild-type flies reduces their sleep, 15 while other studies have suggested that oxidative stress is a driving factor of sleep shortage. 16 In conclusion, oxidative stress regulates sleep; both high and low levels of oxidative stress are detrimental to sleep. It is obvious that insomnia in the perimenopausal period is related to the increase of iNOS.
It is worth exploring whether the excessive increase of iNOS leads to high oxidative stress levels or insufficient increase leads to low oxidative stress levels, which leads to insomnia. However, no study has hitherto assessed the effects of iNOS on insomnia during perimenopause.
As a key mediator of immune activation and inflammation, iNOS is closely related to the proinflammatory response, 17,18 whereby oxidative stress can lead to the release of inflammatory cytokines. 19 Ample evidence suggests that poor sleep in perimenopausal females is associated with mild systemic inflammation. 20 Important proinflammatory cytokines, including interleukin 6 (IL6) and tumor necrosis factor-alpha (TNFα), play a regulatory role in sleep. IL6 may alter circadian rhythms at the molecular level by activating period gene 1 transcription, while the role of TNFα in regulating sleep may be derived from its direct effect on hypothalamic neurons. 21
A study reported that elevated serum IL6 concentrations were predictive of poor sleep quality and associated with decreased total sleep time. 22,23 Besides, IL6 administration leads to early and transient decreases of SWS followed by increased SWS and decreased REMS. 24 A study found that sleep deficiency was related to higher levels of TNFα in college students. 25 Low doses of TNF promoted nonrapid-eye-movement sleep (NREMS) but did not affect REMS, which was inhibited by higher doses of TNF. 26 Although excessive oxidative stress has been observed in perimenopausal insomnia, 27 the effects of oxidative stress and proinflammatory on insomnia during perimenopause remain unknown.
Accordingly, a hypothesis based on current evidence has been laid out: the elevation of iNOS concentrations affects inflammatory cytokines during perimenopause, resulting in an increase in oxidative stress and proinflammatory levels, consequently leading to insomnia. This case-controlled study investigated the association between oxidation and proinflammatory cytokine concentration in perimenopausal subjects with insomnia and further explored risk factors for perimenopausal insomnia.
Materials and Methods
Study design
This observational study was approved by the Institutional Review Board of Inner Mongolian Medical University (YKD2018039) and was performed in accordance with the Declaration of Helsinki. Written informed consent was directly acquired from the participants. The study recruited 127 perimenopausal females admitted to the gynecological outpatient department and hospitalized department of the Affiliated Hospital of Inner Mongolia Medical University.
Participants
All recruited perimenopausal participants were patients who attended the outpatient, or were inpatients at the gynecological department of the Affiliated Hospital of Inner Mongolia Medical University. Sociodemographic and clinical characteristics were collected, including age, years of education, menstrual history, reproductive history, and age of menarche.
Inclusion criteria were as follows: (1) aged 45–55 years 28 ; (2) dysregulated menstrual cycle, that is, at least two times in the last 10 months of menstrual cycle variation ≥7 days or menopause ≥2 menstrual cycles or 60 days but the menopause time is <1 year 29 ; (3) no infectious diseases, viruses, or microorganisms infected; (4) provided informed consent and willing to cooperate.
Patients were excluded for the following reasons: (1) unexplained irregular vaginal bleeding that has not been cured; (2) premature ovarian failure, organic ovarian disease, bilateral ovariectomy; patients with breast tumors; the presence of any other painful diseases; (3) history of sleeping disorders before perimenopause; (4) suffering from thyroid diseases or other endocrine diseases; (5) used sex hormone drugs or participated in other clinical trials within the last month; (6) obstructive sleep apnea syndrome; (7) drug dependence (alcohol, nicotine, cocaine, etc.); (8) presence of severe comorbidities such as cardiovascular and cerebrovascular diseases, liver, kidney, diabetes and hematopoietic system, and severe neuropsychiatric diseases.
Assessment
The Pittsburgh Sleep Quality Index (PSQI), Patient Health Questionnaire-9 (PHQ-9), and Generalized Anxiety Disorder-7 (GAD-7) were evaluated for all participants.
Pittsburgh Sleep Quality Index
It is well established that PSQI is a sensitive, reliable, and effective outcome assessment tool for community-based primary insomnia research, and is simple and easy to implement, 30,31 with Cronbach's α coefficient of 0.702. 32 Nineteen individual items covering seven components were assessed: subjective sleep quality (PSQI component 1, PSQIC1), sleep latency (PSQI component 2, PSQIC2), sleep time (PSQI component 3, PSQIC3), sleep efficiency (PSQI component 4, PSQIC4), sleep disorders (PSQI component 5, PSQIC5), use of hypnotics (PSQI component 6, PSQIC6), and daytime dysfunction (PSQI component 7, PSQIC7). 33,34
Each component was assigned a score between 0 and 3. The sum of these domains provided the global PSQI score, which ranged from 0 to 21, with higher scores indicating poorer sleep quality 35 ; a PSQI global score of >7 confirms the presence of insomnia. 36 Accordingly, all participants were divided into two groups: the insomnia group (PSQI >7) (n = 54) and the normal group (PSQI ≤7) (n = 73).
Patient Health Questionnaire-9
The PHQ-9 is a self-completed questionnaire developed to screen depressive status and assess its severity in nonpsychotic medical patients. 37 PHQ-9 has been identified as the most reliable screening tool for depression. 38 The PHQ-9 demonstrates high internal consistency, and good sensitivity and specificity, 39 with Cronbach's α coefficient of 0.892. 40
PHQ-9 consists of nine items, rated on a 4-point ordinal scale for none at all, a few days, more than half of the days, and almost every day. The responses are summed to provide a total score ranging from 0 to 27, with higher scores indicating a greater frequency of symptoms. 37,41
Generalized Anxiety Disorder-7
The GAD-7 is a self-completed questionnaire used to screen for anxiety status in nonpsychotic patients, 42 and as an effective screening tool for generalized anxiety disorder and assessment of its severity in clinical practice and research. 43 GAD-7 has shown good reliability and criterion, construct and factorial validity. 44 Cronbach's α coefficient was 0.84. 45 GAD-7 consists of seven items, rated on a 4-point ordinal scale for none at all, a few days, more than half of the days, and almost every day. The total number of points is 21 (higher scores indicate more severe symptoms). 46
Blood sample collection and laboratory tests
Five milliliters of venous blood was collected from fasting participants before 10:00 am in a vacuum blood collection tube with gel promotion. After the venous blood collection was completed, a low-speed centrifuge was used to centrifuge at 4000 r/min for 10 minutes. Serum concentrations of sex hormone indexes estradiol2 (E2), follicle-stimulating hormone (FSH), and luteinizing hormone (LH) were assayed by electrochemiluminescence (Cobas8000 automatic biochemical analyzer). The remaining serum was separated and stored in a −80°C freezer. Analyses were performed to measure serum concentrations of IL6 and TNFα using enzyme-linked immunosorbent assay kits (Cloud-clone Corp., Katy, TX, respectively), iNOS using NO synthase typed assay kit (Nanjing Jiancheng Bioengineering Institute, China).
Statistical analysis
All data were expressed as the mean ± standard deviation. In combination with the clinical characteristics of women in the 45–55 age group, iNOS and TNFα levels were compared between the two groups using Student's t-test. Given that IL6 did not conform to a normal distribution, logarithmic transformation was first conducted and then compared by Student's t-test. The nonparametric Mann–Whitney rank-sum test was used to compare the age, years of education, menstrual cycle, fertility history, age of menarche, and the levels of sex hormones between groups. Since the scales PHQ-9, GAD-7, and PSQI had no normal distribution, but were continuous variables, a parametric test was used to analyze them.
Pearson's correlation and partial correlation analyses were performed to analyze continuous variables and PSQI scores in the insomnia group after adjusting for age, educational levels, anxiety and depression, respectively. Multivariate analysis was performed using binary logistic regression; the existence of sleep disorders was taken as the dependent variable, and indicators with statistically significant differences between groups were taken as the independent variable to determine potential influencing factors of sleep disorders.
All statistical analyses were performed using IBM SPSS Statistics for Windows, Version 20.0 (IBM Corp., Armonk, NY). Figures were generated using GraphPad Prism version 8 (GraphPad Software, Inc.). All tests were two sided, and the significance threshold was set at p < 0.05.
Results
Demographic and clinical characteristics
The mean age of all participants was 48.82 ± 2.58 years, and 42.5% (n = 54/127) had insomnia (PSQI >7).
A significant difference in years of education was found between the two groups (p < 0.05), while no differences were found in age, menstrual cycle, fertility history, age of menarche, and sex hormone (E2, FSH, and LH) (all p > 0.05) (Table 1).
Demographic and Clinical Characteristics of the Insomnia group and the Normal Group
All data are expressed as mean ± SD, * p < 0.05. The nonparametric Mann–Whitney U test was used to compare age, the menstrual cycle, fertility history, educational levels, age of menarche, and sex hormones.
C1–C7, component 1–component 7; E2, estradiol2; FSH, follicle-stimulating hormone; LH, luteinizing hormone; PSQI, Pittsburgh Sleep Quality Index; SD, standard deviation.
Differences in scales and biomarkers
The PHQ-9 and GAD-7 scores of the insomnia group were significantly higher than those of the normal group (7.98 ± 5.72 vs. 2.07 ± 2.03, p < 0.001; 5.54 ± 4.88 vs. 2.01 ± 1.98, p < 0.001) (Table 2) (Fig. 1a, b). In addition, the insomnia group had significantly higher IL-6 concentrations compared with the normal group (7.34 ± 7.71 vs. 4.93 ± 2.70, p = 0.012), while iNOS concentrations in the insomnia group were lower than those in the normal group (15.12 ± 4.07 vs. 17.08 ± 3.91, p = 0.007) (Fig. 2a, b), but the TNFα concentration was comparable between both groups (p > 0.05).

The differences of scales between the insomnia and the normal group;

The differences of biomarkers between the insomnia and the normal group;
Scale and Serum Biomarkers of the Insomnia and the Normal Group
All data are reported as mean ± SD, * p < 0.05. Scale and serum biomarkers were compared by Student's t-test.
GAD-7, generalized anxiety disorder-7; IL6, interleukin 6; iNOS, inducible nitric oxide synthase; PHQ-9, patient health questionnaire-9; TNFα, tumor necrosis factor-α.
Correlations and regression analysis
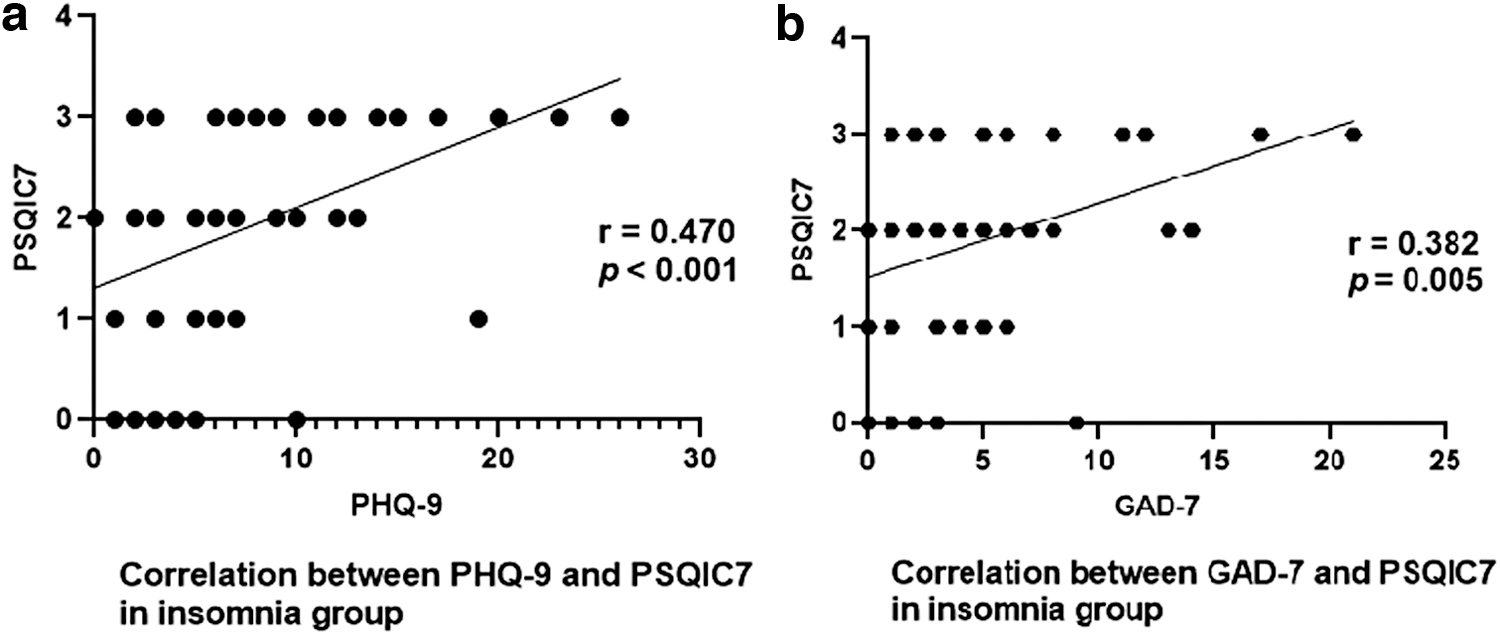
In the insomnia group, after adjusting for age, years of education, GAD-7, and PHQ-9, IL6 concentrations were positively correlated with PSQIC5 and PSQIC7 scores, respectively (r = 0.341, p = 0.018; r = 0.320, p = 0.026). After adjusting for age and years of education, PHQ-9 scores were positively correlated with the PSQI global scores, PSQIC1 and PSQIC7 scores, respectively (r = 0.410, p = 0.003; r = 0.309, p = 0.026; r = 0.470, p < 0.001); GAD-7 scores were positively correlated with the PSQI global scores (r = 0.435, p = 0.001) and PSQIC7 scores (r = 0.382, p = 0.005) (Fig. 3a, b). No significant correlation was found between INOS and IL6 and TNFα (all p > 0.05).
Correlation between anxiety, depression, and sleep subscale;
In the normal group, after adjusting for the covariates of age, years of education, anxiety and depression, iNOS, IL6, and TNFα exhibited no significant correlation with PSQI, and PHQ-9 and GAD-7 had no significant correlation with biomarkers in the noninsomnia group (all p > 0.05). Moreover, INOS exhibited no significant correlation with IL6 and TNFα, respectively (all p > 0.05).
Subsequently, binary logistic regression was conducted to explore the risk factors for insomnia in the perimenopausal period. The existence of insomnia was taken as the dependent variable, and the variables with significant results in univariate analysis of the two groups were taken as the independent variables, namely years of education, iNOS, IL6, PHQ-9, and GAD-7. Among them, “years of education” was assigned and analyzed as a dummy variable. We found that PHQ-9 (odds ratio [OR] = 1.588, 95% confidence interval [CI] [1.306–1.931], p < 0.001) and IL6 (OR = 2.360, 95% CI [1.074–5.184], p = 0.032) were risk factors, while iNOS (OR = 0.821, 95% CI [0.710–0.949], p = 0.008) was a protective factor (Table 3).
Binary Logistic Regression of Factors Affecting Insomnia in Perimenopause
Cox&Snellr 2 and Nagelkerker2 of the logistic regression equation were 0.463 and 0.624, respectively. The Hosmer–Lemeshow test statistic was 4.839 (p = 0.775), and the prediction accuracy of the Logistic regression fitting equation was 81.6%, * p < 0.05.
CI, confidence interval; OR, odds ratio; SE, standard error.
Discussion
To our knowledge, this is the first study to explore the effects of oxidative stress and proinflammation levels on insomnia during perimenopause simultaneously. We provide hitherto undocumented evidence that iNOS might be a protective factor for perimenopausal insomnia, with higher concentrations of IL6 and lower concentrations of iNOS in participants with insomnia than in participants with normal sleep. Second, perimenopausal mood disorders do have a certain role in promoting insomnia, mainly depressed mood plays a role; anxiety mood performance is not obvious.
iNOS synthesizes the production of NO. 47 NO is an endogenous sleep-promoting factor widely involved in regulating the sleep–wake state involved in mediating sleep homeostasis by affecting the activity of the ascending reticular activation system. 48 Current evidence suggests that iNOS is not expressed in a healthy state but after immune or microbial stimulation, and continues to produce NO until the enzyme is degraded. 47 It has been established that perimenopausal estrogen deficiency can induce the expression of iNOS in blood vessels. 12
NO produced by iNOS plays an important role in the body's defense ability, while under long-term pathological conditions, the high level of NO produced by iNOS can lead to the formation of peroxynitrite and DNA damage. 49 It is widely thought that iNOS is permanently expressed with aging, and the production of corresponding NO/iNOS is important to ensure the full maintenance of REMS and SWS, while the impaired expression of iNOS negatively affects SWS and REMS. 9 Moreover, iNOS plays a major role during recovery of NREMS. An animal experiment demonstrated that the knockdown of the iNOS gene in mice reduced NREMS. 10
Many studies on the relationship between diseases and iNOS have highlighted that iNOS may act as a protective molecule in the disease process. 50,51 The above findings suggest that insomnia during the perimenopausal period may be related to decreased serum iNOS and protective ability. In other words, iNOS has a protective effect on sleep within a certain concentration range, which means that high or low concentrations of iNOS might not play its protective effect on insomnia due to inability or oxidative stress.
Current evidence suggests that iNOS concentrations increase in perimenopausal women due to a lack of estrogen. 12 We speculate that subjects whose iNOS concentration has not increased to a predetermined range suffer from insomnia due to a lack of protection in their sleep. As for the specific scope, we need to explore further. However, the relationship between iNOS and perimenopausal insomnia has been largely underestimated, highlighting the importance of future studies with larger sample sizes.
Moreover, we demonstrated that IL-6 might be a risk factor for perimenopausal insomnia. Under normal circumstances, the serum concentrations of IL6 in the sleep cycle stages 1 and 2 and the REM phase are higher but lower in SWS; the overall performance is high at night and low during the day. High levels of IL6 stimulate the hypothalamic pituitary adrenal (HPA) axis and cause hyperactivity of the HPA axis, which is closely associated with the development of sleep disorders. It has been shown that IL6 may also affect sleep–wake regulation by affecting neurotransmitters and their receptors. For example, IL6 can weaken 5-hydroxytryptamine2A (5-HT2A) receptor signaling, 52 and mice with 5-HT2A receptor knockout exhibit significantly increased wakefulness and decreased SWS. 53
There is a rich literature available substantiating that higher levels of IL6 are correlated with short sleep duration and a delayed circadian rhythm. 23,54 A study on subjective sleep quality in older adults found that poor sleep quality was associated with long-term high levels of IL6. 55 Besides, in a study on the relationship between inflammatory cytokines and sleep disorders in patients with liver cirrhosis, researchers found that a high concentration of IL6 predicted poor sleep quality, and IL6 was an independent predictor of sleep disorders. 22
A clinical trial based on 519 participants confirmed that insomnia was significantly associated with higher blood IL6. 56 With aging, circulating proinflammatory cytokine levels increase, and females become vulnerable to inflammation. 57 At the same time, compared with males, females may be more susceptible to insomnia. Another study found that increased IL6 levels are linked to poor sleep quality and efficiency in perimenopausal females, 58 which confirms the reliability of our study. This study also found that serum IL6 was positively correlated with PSQIC5 (sleep disorders) and PSQIC7 (daytime dysfunction) in the insomnia group.
A French study found that a high concentration of IL6 in middle age was predictive of cognitive decline and led to a decrease in mental status scores. Increased IL6 may cause a decline in cognitive function, affecting daytime function in perimenopausal females. In addition, our study did not find an association between insomnia and TNFα, although some studies suggested that sleep deprivation can lead to elevated levels of TNFα. 59 However, a meta-analysis showed that high levels of TNFα were not associated with insomnia. 58 In a nutshell, the proinflammatory factor IL6 plays an important role in the occurrence of perimenopausal insomnia, unlike TNFα.
In this study, regression analysis found that depression was a risk factor for the development of insomnia during the perimenopausal period after controlling for other factors, and higher levels of depression were associated with worse subjective sleep quality, consistent with findings reported by Peters et al. 60 The perimenopausal period is considered a vulnerable window for developing depressive mood and depressive episodes. 61 Previous exposures to stress combined with the effects of aging and a changing pattern of estradiol secretion could dysregulate the function of the HPA axis, increasing possibilities of perimenopausal women developing depression. 62,63 Hyperactivity of the HPA axis is the most common neuroendocrine abnormality in perimenopausal depression. 64
Furthermore, the Chinese Sleep Research Society proposed that HPA axis overactivity may play an important role in the occurrence and maintenance of insomnia, leading to the individual's sleep becoming lighter and increasing night wakefulness. 65 Taken together, these findings suggest that the development of perimenopausal depression may be related to changes in the HPA axis, and depression causes insomnia through these common mechanisms. The prevalence of comorbid depression and insomnia in perimenopause is 31.5%. 66
What's more, both PHQ-9 and GAD-7 were positively correlated with PSQIC7. Using two r-value comparisons, we found that the effect of PHQ-9 on PSQIC7 was significantly greater than that of GAD-7 reported in this study. It has been established that the core symptoms of depression affect adults' daily lives through unstable mood, daytime fatigue, nonrestorative sleep, reduced motor activity, somatic symptoms, and appetite and weight change. 67 A high degree of depression significantly affects daytime function and activities in perimenopausal females. Similarly, previous studies have shown that lower daily activity level is the core feature of mood disorders. 68 Importantly, less emphasis has been placed on anxiety. However, our results showed similar effects on depression.
There were some limitations in our study. First, the sample size analyzed in this study was relatively small but was selected based on strict criteria to reduce potential confounding factors. Moreover, the self-rating questionnaire PSQI was used to evaluate sleep. It is well established that compared with polysomnography (PSG) test results, there may be some differences between the subjective and objective evaluation results. Although subjective scales may affect the results, they are convenient and easy to operate.
In contrast, PSG may yield more reliable data, but requires more cooperation from the subjects. Finally, perimenopause is a special transitional period whereby many factors affect women's sleep. Some problems, such as sexual life, family income, weight, and other factors that affect sleep, were not discussed, and should be explored in future studies with larger sample sizes. In the future, a large sample size will be collected, and further divided into urban and rural subgroups, or 45–50 and 51–55-year-old groups to explore the effects of zone or age on REM and NREM1, 2 (light sleep) and NREM3, 4 (deep sleep).
Conclusion
This study provided preliminary evidence that moderate oxidative stress plays a protective role in the development of perimenopausal insomnia, while proinflammatory and depression were risk factors, based on lower concentrations of iNOS and higher levels of IL6 and depression found in females with insomnia during perimenopause. Overall, the above findings broaden our understanding of the pathophysiology of perimenopausal insomnia.
Footnotes
Acknowledgments
We thank all the participants for their willingness to participate in the study and the time that they devoted to the study.
Authors' Contributions
F.W., Y.K., and J.Z. designed the study. F.W., Y.K., and Y.Y. secured funding for the study. J.Z., Y.J., and Y.Z. led the drafting of the article. J.Z. led the statistical analyses. J.Z. and L.Z. collected the clinical samples. J.Z. and P.W. finished the laboratory tests. J.Z. and C.K. input the data. Y.Y. and W.W. directed the clinical and experimental guide. All authors approved the final article for submission.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This work was supported by the following grants: The Technology Support Project of Xinjiang (2017E0267), The 10th Inner Mongolia Autonomous Region’ Prairie excellence’ Project, Natural Science Foundation of Inner Mongolia (2022MS08068), Natural Science Foundation of Xinjiang Province (2018D01C228 and 2020D01A23), Outstanding Youth Science and Technology Talents of Xinjiang (2017Q007), Natural Science Foundation of China (81560229), and Beijing Natural Science Foundation (7152074).