
Abstract
Objective:
To compare gender compositions in the leadership of the top 25 medical schools in North America with the leadership of their affiliated university senior leadership and other faculties.
Materials and Methods:
This retrospective cross-sectional observational study used publicly available gender data from 2018 to 2019 of universities drawn from the U.S. News Best Global Universities for Clinical Medicine Ranking report. Gender compositions in eight leadership tiers from senior leadership to medical school department directors were analyzed. Data analysis included gender compositions by leadership tier and faculty.
Results:
Male representation is greater at higher leadership tiers, with the largest imbalance being at the level of medical school department heads. The faculty of medicine has more men in leadership positions than the average of the other faculties (p = 0.02), though similar to schools of engineering, business, dentistry, and pharmacy. Across the eight leadership tiers, a significant trend exists between tier and proportions, indicating that male representation was greater at higher tiers (p < 0.001). No correlation was found between a university's leadership gender composition and its ranking.
Conclusion:
The under-representation of women is greater in medical school leadership than the leadership of their affiliated universities. The faculty of medicine has greater male over-representation than the average of the other faculties.
Introduction
Women have been historically under-represented in medical school graduating classes, and gender inequality remains intractable in academic medicine. 1 –5 Ongoing efforts have aimed to remedy this disparity with initiatives targeting the reduction of gender-based inequities and bias. 6 –9 In recent years, the U.S. medical school matriculant rates of women have increased with 52% of matriculants from U.S. medical schools in 2019 identifying as women, while the percentage of practicing women physicians was 36%. 10,11
Furthermore, under-representation of women remains endemic in academic and leadership positions in medicine. 4,5,12 –15 Compared with men in similar positions, women generally receive lower compensation, have fewer publications, citations, awards, and receive less funding. 3,7,16 –21 Gender disparity has been documented in various academic disciplines, 13,22 –27 professional society leadership, 28 –30 journal editorial boards, 31 –33 and clinical trials. 34 –36 These factors in conjunction with implicit bias have the potential to keep equity and inclusion in medicine an elusive dream. 37,38
The interactions between university hierarchical (vertical) leadership and departmental (horizontal) leadership influence the performance of organizations and institutions. 39 –41 Studies examining this relationship conclude that the balance between vertical and horizontal leadership determines successful outcomes and warrants further investigation. 42,43 Despite this, the majority of gender leadership research is intradisciplinary, or single leadership tier only. 12 –15,17,44 –52 Our study examines gender trends in medicine at the institutional scale, both vertically within the leadership hierarchy and horizontally by comparing academic disciplines, and includes a focus on deans, associate deans, and assistant deans across various faculties.
Materials and Methods
Data collection
The top 25 medical schools in North America were selected from the U.S. News Best Global Universities for Clinical Medicine Ranking report. 53 U.S. News determined school rankings though considering number of publications, presence of international collaboration, number of citations, as well as the number and percentage of a university's publications within the top 1% of the most cited articles in their respective disciplines. 54
The data from the top 25 medical schools and their affiliated universities were analyzed using R 4.1.0 (R Foundation for Statistical Computing, Vienna, Austria). Eight leadership tiers were created with strict inclusion and exclusion criteria to account for variability in leadership titles between schools. These tiers span a hierarchy that includes senior leadership, faculty leadership, and medical school leadership (Fig. 1).
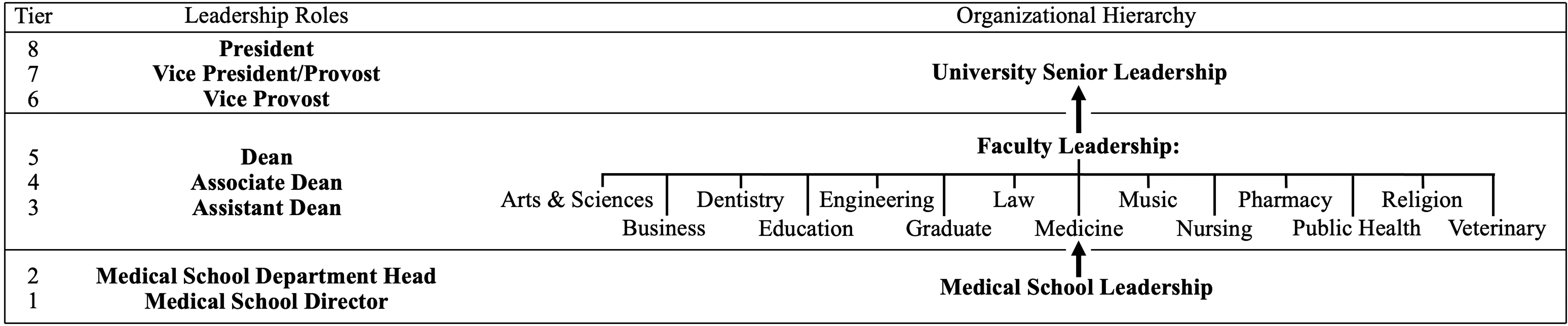
Organizational hierarchy. Vertical analysis comprises eight tiers of leadership roles. Horizontal analysis comprises 14 faculties spanning Tiers 3–5.
The eighth tier included the president or the equivalent highest ranked leadership role of chancellor. The seventh tier included the position of vice president and equivalent roles such as vice chancellor and provost. The sixth and final tier of senior leadership comprised the vice provost. Each university's schools, colleges, and faculties were assigned to 1 of 14 faculties. Tiers 5, 4, and 3 represent leadership roles within the various faculties (arts & sciences, business, medicine, etc.) of a university, and consist of the dean, associate dean, and assistant dean, respectively. The dean, associate dean, and assistant dean tiers are the focus of the horizontal comparison between medical school leadership and other university faculties.
Tiers 2 and 1 represented leadership specifically within the faculty of medicine and consist of the department head and department director roles of medical schools. The study's exclusion criteria eliminated emeritus roles, retired staff, individuals without identifiable leadership position, and individuals without identifiable gender or nonbinary status.
Consistency was maintained by having the same researchers generate the entire data set. All data were obtained from publicly available sources such as university websites. Each role was categorized into one of the eight tiers and gender determined through pronouns in descriptions, references, and profiles such as LinkedIn. Individuals who held more than one leadership position were assigned to the tier corresponding to their highest academic position.
Vertical analysis
The vertical analysis was designed to investigate the gender distribution across different leadership tiers within the medical schools and their affiliated universities. This analysis was conducted using a generalized linear model, where the proportion of females in each tier was regressed against the tiers of leadership, and against the tier groups of senior, faculty, and medical school leadership. The generalized linear model was chosen as it allows for the modeling of relationships between variables that may not be normally distributed.
By regressing the proportion of females against the tiers of leadership, this approach helps in understanding how gender representation changes across different levels of hierarchy. The adjustment for the cluster effect in the standard errors for each estimated slope ensures that the unknown effect of tier groups is accounted for. The t-test of the slope was then conducted to determine whether the observed trend was statistically significant.
Horizontal analysis
The horizontal analysis focuses on comparing gender representation across different faculties. The chi-square goodness-of-fit test was used to determine whether the observed gender proportions across different faculties were consistent with expected proportions. This test is appropriate for categorical data and helps in identifying whether there are significant differences in gender representation across faculties. The post hoc z-score tests with the Holm procedure were then used to identify specific pairs of faculties where the gender proportions were significantly different. The Holm procedure was applied to control the family-wise error rate, reducing the likelihood of Type I errors that can occur when performing multiple comparisons.
Results
From 22 U.S. and 3 Canadian medical schools, a total of 4008 university and medical school faculty in leadership positions were included in our study.
Gender proportion by leadership rank
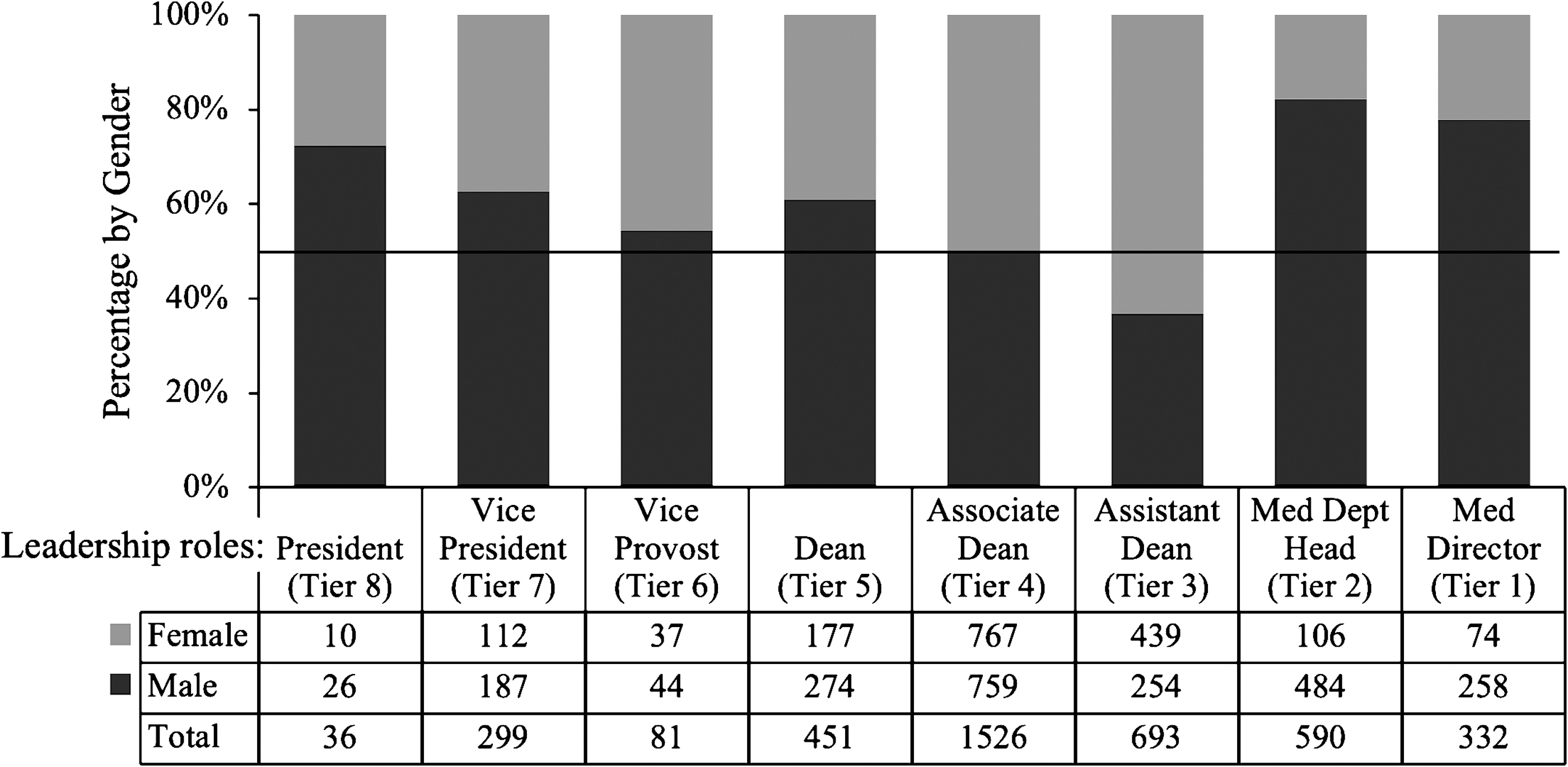
There was under-representation of women in medical school leadership compared with the leadership of affiliated universities (p < 0.001, Fig. 2a). Male representation was greatest in medical school department heads (Fig. 3). Men outnumbered women with a majority of 60% or greater in the leadership hierarchy of president, vice president, dean, medical school department head, and medical school department director positions.
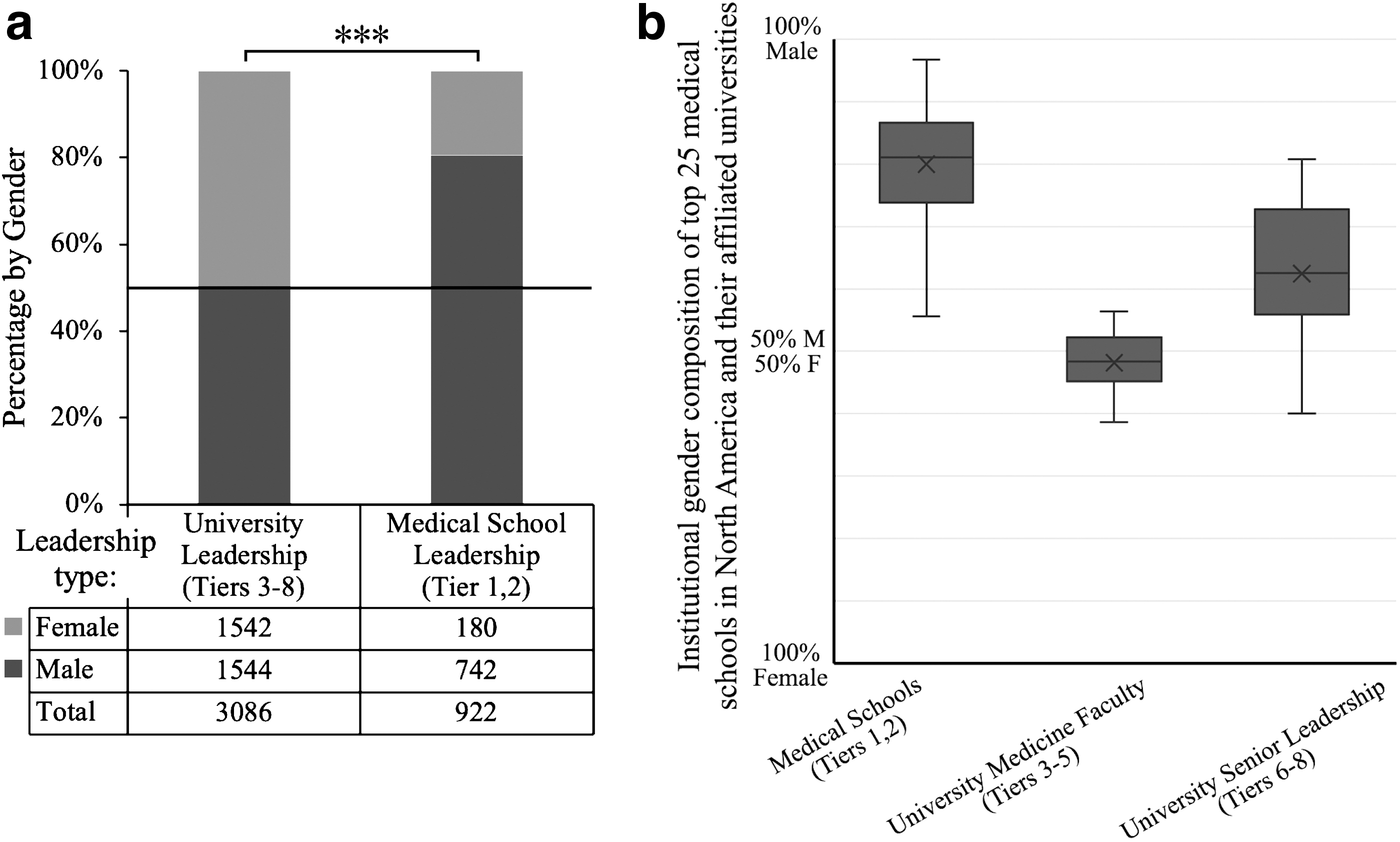
Gender disparity in medical school leadership (Tiers 1 and 2) compared with the leadership of their affiliated universities (Tiers 3–8) organized by tiers.
Female predominance was at the assistant dean rank at 63%. The remaining ranks included the vice provost with a male majority at 54% and the assistant dean that had parity between male and female gender. For tiers 1–8, a t-test of the slope of the regression line determined a significant trend between tier and proportions, indicating that male representation was greater at higher tiers (p < 0.001).
Gender proportion by faculty
The faculty of medicine had the fourth largest percentage of male leaders (Fig. 4a) and a z-test of proportions showed that medical faculty had greater male representation than the average of the other faculties for the dean, associate dean, and assistant dean tiers (p = 0.02 for dean, p = 0.004 for associate dean, and p = 0.003 for assistant dean, see Supplementary Fig. S1, which compares the faculty of medicine with other faculties). For most faculties, the dean tier had the greatest male representation, whereas the assistant dean tier had the greatest female representation (Fig. 4b).
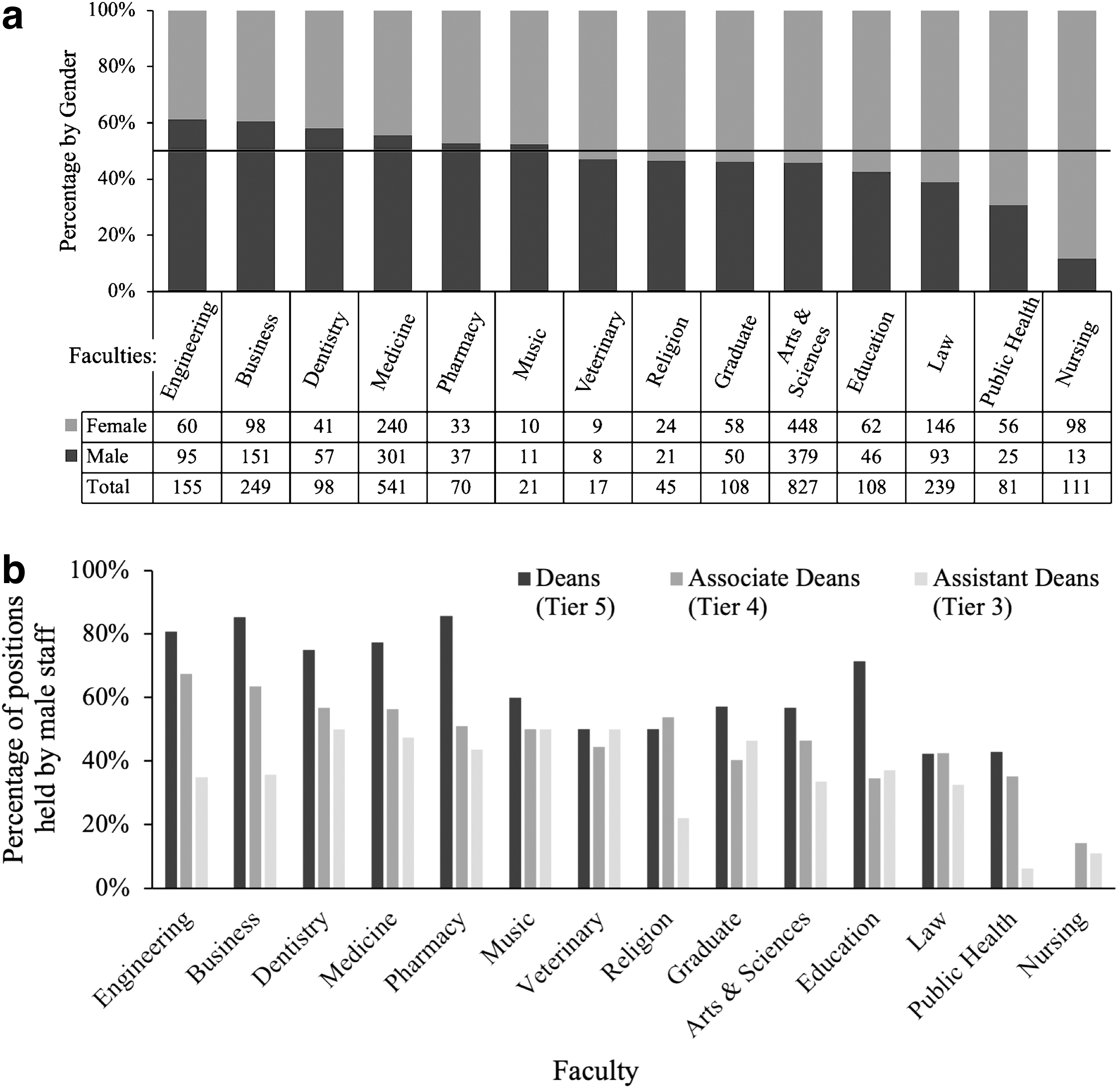
Gender disparity within faculty-level leadership (Tiers 3–5),
The chi-square goodness-of-fit test indicated significant differences in proportions between the faculties (p ≤ 0.001). The p-value matrix for the post hoc z-score test details faculty pairs with gender proportions that are significantly different (Fig. 5). The gender proportion of the nursing faculty was found to have significantly greater women representation than all other faculties except for the veterinary and public health faculties.
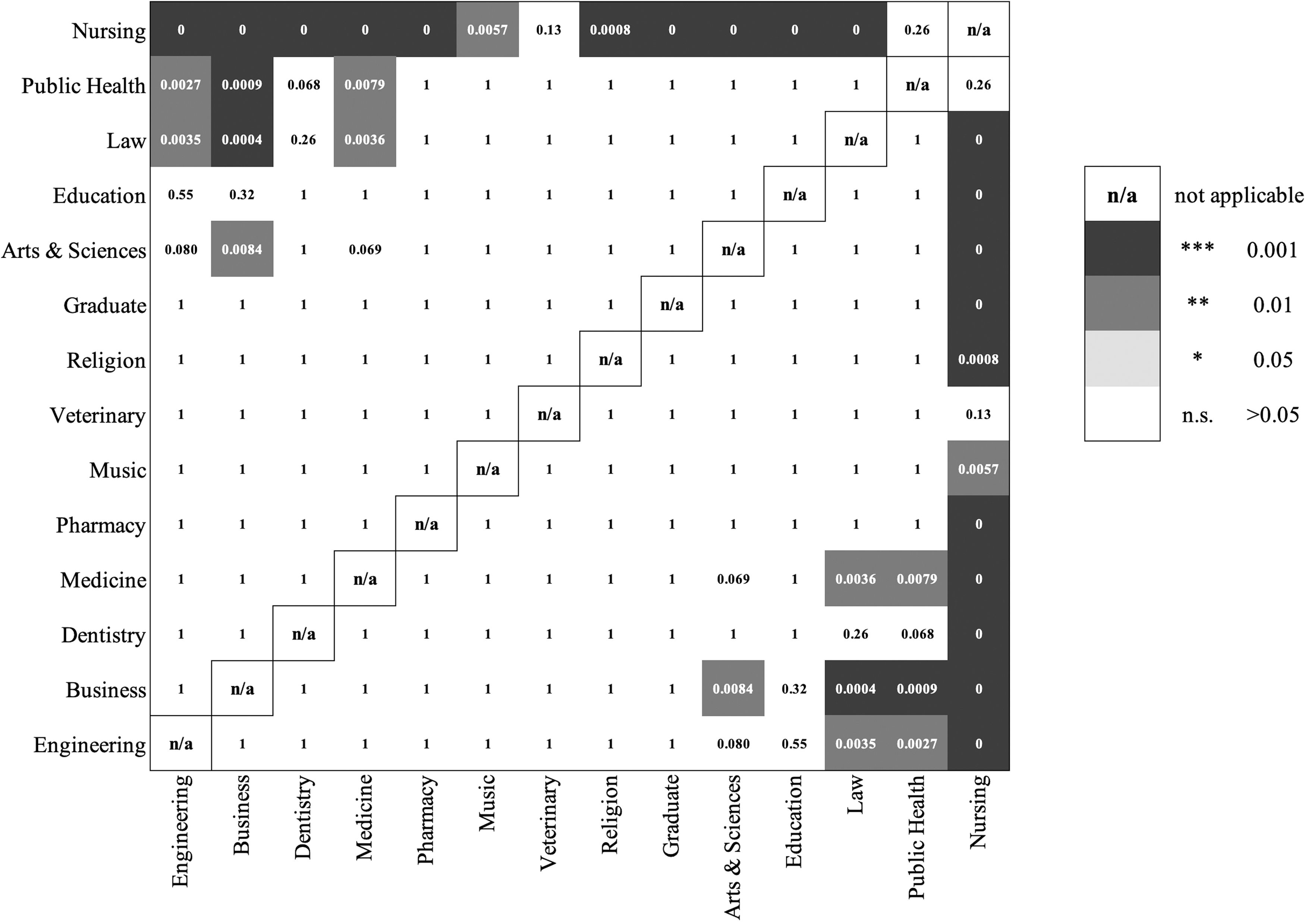
Matrix of p-values for the post hoc z-score test on gender disparity by faculty.
Engineering, business, and medicine had significantly greater male representation than the faculties of law and public health. Business and medicine also had greater male representation than the faculty of arts and sciences. However, the greater male representation of medicine compared with arts and sciences was not statistically significant (p = 0.07).
Leadership composition by school
The top 25 medical schools in North America had an average institutional leadership gender composition that was 80% ± 9% male (mean ± standard deviation, Fig. 2b). Average leadership gender composition of the affiliated universities' faculties of medicine was 52% ± 5% women. The gender composition of medicine faculty leadership was marked by male representation in the dean tier and women representation in the assistant dean tier (Fig. 4b). The senior leadership of the affiliated universities had an average gender composition that was 62% ± 11% male.
Plotting each institution's gender composition of its medical school leadership against its senior and faculty leadership showed no correlations in gender disparity between medical school and affiliated university leadership (see Supplementary Fig. S2, which compares medical school and university leadership). Furthermore, no correlations were found between gender composition and university ranking.
Discussion
This retrospective cross-sectional study analyzed vertical and horizontal leadership gender differences in medical school and their affiliated universities, although previous publications have examined gender differences in specific departments or leadership tiers. 4,5,17,27,51,55,56 Our results are consistent with prior research on women under-representation in academic leadership. Furthermore, we found that the under-representation of women in medical school leadership was greater than of affiliated universities at every leadership tier.
The faculty of medicine had greater representation of male leaders than the average of other faculties and had the fourth largest percentage of male leaders, comparable with other male-dominated faculties such as engineering, business, and dentistry. Our data highlight the need for additional research on the potential factors contributing to these observed gender differences in leadership roles within medicine.
This under-representation has been referred to as sticky floor, broken ladder, and glass ceiling and has been proposed as obstacles preventing women from advancing in academic medicine hierarchies. 57 Leadership positions in disciplines that have historically been male dominated have lower percentages of women in their senior leadership. 1,8,58 This gender disparity results in fewer women role models and mentors, potentially limiting the motivation of aspiring women leaders and perpetuating bias in the leadership environment. 59
Compared with men, more women remain in interim and mid-level administrative positions for longer periods of time before pursuing senior positions. 60,61 This is consistent with our results that determined a correlation between leadership tier and gender disparity, with higher tiers being predominantly male and lower tiers mostly female.
Social barriers such as implicit bias make it more difficult for women to advocate for their values and highlight their accomplishments compared with men. 37,62 –65 Fewer women apply to clinical excellence awards, and achieve lower success rates for senior awards than for lower-tier awards. 66,67 Women in academic medicine find fewer opportunities to increase the visibility of their work through assuming peer reviewer and editorial writer positions. 68 Traditional news media, modern journalism, and social media platforms contribute to gender bias through amplifying and promoting male perspectives. 69
These factors may result in discouragement and prevent women from putting themselves forward and seeking leadership opportunities, further perpetuating these biases. 67 Implicit gender bias and social barriers can render leadership an uncomfortable experience for women, especially when lacking support and resources. 37,70
Gender role stigma pertaining to household and workplace norms may set gender-based societal expectations for women leaders. 71 Although home duties and caretaking responsibilities may divert attention from academic pursuits, gender differences in career trajectories cannot be explained solely by differing priorities and aspirations. 72 Nevertheless, women continue to face structural challenges such as imbalanced divisions of domestic labor and having tenure-track years coinciding with their prime reproductive years. 9,17
Preventable gender-based barriers associated with childbearing responsibilities hinder women's ability to seek leadership. 73 Women in medicine often assume the majority of domestic responsibilities and disproportionately experience burdens of family. 74 Although improvements in gender stereotypes have been observed in recent decades, the COVID-19 pandemic has resulted in widening gender disparities. 75 –80
Women in medicine face discrimination both in the clinic and in academia, which negatively impacts motivation and career advancement. 59,81 Sexual harassment persists within medicine owing to gender and power imbalances, amplifying the struggles of aspiring women leaders. 59,82,83 Eliminating gender-based harassment and discrimination requires integrating women into positions of authority, thereby decreasing women's barriers to voicing concerns. 17,64,75,84
Although gender disparities in some specialties of medicine have seen recent corrections, substantial disparities in senior academic ranks and leadership persist and further improvement efforts are needed. 10,11,76 –78,85 Factors contributing to observed gender differences in leadership roles can be addressed by implementing change. Peer mentoring programs can augment the support networks of women faculty, as well as foster academic productivity and advancement. 60,86,87
Strategies to reduce implicit biases can be promoted through physician education. 88 Eliminating such biases is critical in furthering institutional change and the promotion of women to higher ranks. 64,89 Furthermore, it is worth noting that gender disparity is inextricably linked with the intersections of class, ethnicity, geography, sexuality, and many other socioeconomic factors. 90 –94 These relationships as well as numerous other interventions for improving gender disparity warrant further evaluation. 7 –9,37,75,85,93,95
Our study has limitations. First, gender identity is a multifaceted individual and social construct. Although most subjects in this study were identified in binary terms based on their pronouns, a certain portion of subjects may self-identify as gender neutral or as transgender. Second, data collection depended on institutional websites, which all may not have been updated. Third, the choice of only the top 25 medical schools from North America based on U.S. News Ranking methodology limits the generalizability and external validity of the study.
Fourth, the study focused on analyzing gender patterns of leadership in Tiers 1 and 2 specifically within the faculty of medicine. The absence of a similar evaluation for other faculties represents a limitation, as it restricts the comparative understanding of gender trends across different academic disciplines. Future research could address these limitations by expanding the scope of the study, incorporating more diverse methods of gender identification, and including a broader range of institutions and faculties.
Conclusions
The results of this study suggest that the under-representation of women is greater in medical school leadership than in the leadership of their affiliated universities. The faculty of medicine has greater male over-representation than the average of the other faculties, as well as the specific faculties of law, public health, and nursing. Our study lays out benchmark data and motivation for further investigation into potential causes and influencing factors for gender differences in leadership within medicine.
Footnotes
Acknowledgments
F.K. is the recipient of the Michael Smith Health Research BC Award (2023–2028); University of British Columbia Radiology—Excellence in Equity, Diversity & Inclusion Award (2023); Don Rix Physician Leadership Lifetime Achievement Award (2022); BC Achievement Foundation—Mitchell Award of Distinction (2022); University of British Columbia—Distinguished Achievement Award for Equity, Diversity & Inclusion (2022) and Vancouver Medical Dental & Allied Staff Association—Equity, Diversity & Inclusion Award (2022).
Authors' Contributions
W.W. processed the data and wrote the article. Z.C. performed the statistical analyses and contributed to writing the article. S.F. reviewed versions of the article and provided detailed input. J.D. and F.K. contributed to the design and implementation of the research as well as reviewing the article. A.P. reviewed versions of the article and provided detailed edits.
Availability of Data and Materials
Author Disclosure Statement
No competing financial interests exist. The authors report no proprietary or commercial interest in any product mentioned or concept discussed in this article.
Funding Information
No funding was received for this article.
Supplementary Material
Supplementary Figure S1
Supplementary Figure S2
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.