
Abstract
Background:
There is still controversial or limited evidence on whether sex differences exist in clinical characteristics, the risk of contrast-induced nephropathy (CIN), and other clinical outcomes of patients who received coronary angiography (CAG) and/or percutaneous coronary intervention (PCI). The aim of this study was to characterize the effect of sex on clinical characteristics and outcomes of patients undergoing CAG and/or PCI.
Methods:
A total of 3,340 consecutive patients undergoing CAG and/or PCI from May 2017 to December 2022 were assessed in this retrospective study. Subgroup analyses by sex were performed. Clinical characteristics, treatments, the risk of CIN, and other clinical outcomes, including in-hospital and follow-up, were compared between females and males.
Results:
Females undergoing CAG and/or PCI tended to have an advanced age (65.8 versus 63.3 years, p < 0.001), a higher burden of complications, and received PCI less frequently compared with males (43.2% versus 64.2%, p < 0.001). After adjustment, female sex was associated with a higher incidence of CIN [adjusted odds ratio (aOR) 1.47; 95% CI 1.08–2.01; p = 0.015] and a higher all-cause readmission rate (aOR 1.26; 95%CI 1.02–1.56; p = 0.031). Meanwhile, females undergoing CAG alone demonstrated a higher risk of severe arrhythmia compared with males after controlling for potential confounders (aOR 1.52; 95% CI 1.12–2.04; p = 0.006).
Conclusion:
Sex disparities exist in the clinical characteristics, treatments, the risk of CIN, and other clinical outcomes among patients undergoing CAG and/or PCI. Female sex was identified as an independent predictor of risk for CIN, all-cause readmission rate, and severe arrhythmia.
Introduction
Coronary artery disease (CAD) has become a common and frequently occurring disease that endangers human health and remains the leading cause of death and disability in men and women worldwide. 1,2 Coronary angiography (CAG) is one of the most frequently used diagnostic methods in patients with suspected CAD, and percutaneous coronary intervention (PCI) is the preferred nonsurgical revascularization procedure for patients with CAD. Both are associated with an increased risk of contrast-induced nephropathy (CIN). 1,3 CIN is one of the principal complications of procedures that require the use of iodinated contrast media, the third leading cause of iatrogenic acute kidney injury, 4,5 which is associated with prolonged hospitalization, increased mortality, and hospitalization costs. 6,7 It is noteworthy that patients with advanced age, a higher burden of complications, and reperfusion delay are more likely to develop CIN. 5,8 However, there is still a paucity of effective treatment for CIN; 5,9 hence, early identification and prevention for this high-risk population is mandatory.
At present, it is controversial whether there are sex differences in the risk of CIN in patients undergoing CAG and/or PCI, even though these differences are largely influenced by risk profile. 6,8,10 In addition, there is still uncertainty about sex differences in short-term and long-term prognosis after CAG and/or PCI, although a growing awareness that female sex may be related to a worse prognosis. 8,11,12 Even after adjusting for possible confounding factors, inconsistent results were still obtained. 12 –14 Therefore, it is necessary to further explore the effect of sex on the short-term or long-term prognosis of patients undergoing coronary revascularization.
The aim of this study was to compare sex disparities in the risk of CIN and other clinical outcomes among patients undergoing CAG and/or PCI and to systematically evaluate the effects of sex on patient and procedure characteristics, medications, laboratory, and imaging characteristics.
Methods
Data sources and study population
We retrospectively collected data from 16,759 consecutive patients undergoing CAG and/or PCI between May 2017 and December 2022 in Cardiac Medical Center of Fujian Medical University Union Hospital, Fuzhou, China. Given that the primary outcome was the development of CIN, we first excluded patients who had no postoperative serum creatinine or who had postoperative serum creatinine for more than 72 hours. Meanwhile, in order to reduce the renal perfusion injury caused by surgery, we excluded patients who underwent on-pump coronary artery bypass grafting and other urgent surgeries. A total of 3,668 were eligible for analysis. The exclusion criteria included age less than 18, allergic to iodine contrast media, ongoing dialytic treatment, as well as patients with missing data or discharge status. Eventually, 3,340 patients were included (Fig. 1). This study was approved by the Fujian Medical University Union Hospital Ethics Committee and conformed to the ethical guidelines of the Declaration of Helsinki.

Flow diagram of the screening and enrollment of study patients.
Baseline data collection
Baseline data were collected from the Electronic Medical Records System of the Fujian Medical University Union Hospital. The data mainly included sociodemographic data, admission and discharge diagnosis, laboratory and imaging examinations, medications, procedural characteristics, and discharge status. The baseline value was defined as the most recent preoperative serum creatinine level and other laboratory indices. The surgical information included the type of stents and the number of stents.
Clinical definition and covariates
The ejection fraction (EF), pulmonary artery diameter (PA), and pulmonary artery systolic pressure (PASP) were measured by echocardiography. CAD was defined according to current guidelines 15 combined with the discharge diagnosis. Heart failure was confirmed by the discharge diagnosis and New York Heart Association class >2. Hypertension, diabetes mellitus (DM), and stroke were defined using the 10th Revision Codes of the International Classification of Diseases. The diagnostic criteria of chronic kidney disease (CKD) were based on Guidelines for the Screening, Diagnosis and Prevention of Chronic kidney Disease in China (2017), 16 estimated glomerular filtration rate (eGFR) <60 mL/min/1.73m2, and calculated with MDRD formula. Liver dysfunction was defined as the discharge diagnosis and serum aspartate aminotransferase level >100U/L. The guidelines for the prevention and treatment of dyslipidemia in Chinese adults (2016) 17 were used to define the diagnosis of hyperlipidemia. Hyperuricemia, pulmonary arterial hypertension (PAH), pulmonary infection, anemia, malignancy, and myocardial infarction (MI) were defined by the discharge diagnosis. A history of MI, cerebrovascular accident (CVA), pneumonia, PCI, and coronary artery bypass graft (CABG) was confirmed by past medical history. CIN was defined as an absolute increase of 44.2 μmol/L (0.5 mg/dL) or a relative increase of 25% in serum creatinine from baseline within 48 to 72 hours after intravascular use of iodinated contrast agents.
The covariates included demographic characteristics [age, smokers, and body mass index (BMI)], comorbidities [CAD, MI, unstable angina, heart failure, hypertension, DM, stroke, hyperlipidemia, hyperuricemia, anemia, PAH, pulmonary infection, malignancy, CKD, liver dysfunction, prior MI, prior CVA, prior pneumonia, prior PCI, and prior CABG], imaging characteristics (EF, PA, and PASP), laboratory tests [albumin, fasting blood glucose (FBG), blood urea nitrogen (BUN), serum creatinine (Scr), eGFR, total cholesterol (TC), high density lipoprotein cholesterol (HDL-C), low density lipoprotein cholesterol (LDL-C), and apolipoprotein A (APOA)], medications [diuretics, angiotensin-converting enzyme inhibitor or angiotensin receptor blocker or angiotensin receptor–neprilysin inhibitor (ACEI/ARB/ARNI), β blockers, statins, and dual antiplatelet therapy (DAPT)], and procedural characteristics (number of infarcted arteries, repeated angiography in <7 days, hydration therapy, contrast volume, stent number).
Outcomes measured
The primary outcomes were the risk of CIN, all-cause in-hospital mortality, major bleeding, repeated revascularization, and all-cause readmission rate. Major bleeding included intracranial bleeding and upper and lower gastrointestinal bleedings. Repeated revascularization was defined as secondary stent placement in addition to the first stent during hospitalization and excluded patients who underwent CABG surgery instead. The all-cause readmission rate was defined as the first admission for any cause within 1 year of discharge. The situation of readmission was obtained by reviewing medical records or contacting the patient or physician in charge. The mean follow‐up duration was 11 months in this study. Patients who were missing discharge data or died while in the hospital were excluded from the readmission analysis.
The secondary outcomes included major adverse cardiovascular events (MACE). MACE was defined as acute myocardial infarction (AMI), acute heart failure (AHF), and severe arrhythmia from any cause, which was obtained from the discharge summary and the postoperative course records.
Statistical analyses
Subgroup analyses were performed for female and male patients. Baseline data were presented as frequencies and percentages for categorical data, and the comparison between groups was analyzed with the χ2 test. When continuous variables conformed to a normal distribution, results were expressed as mean ± standard deviation, and the t test was performed. Otherwise, a descriptive statistic was calculated using median and interquartile range, and the differences between groups were analyzed by the Mann–Whitney U test. Statistical significance was defined as a p value <0.05.
Study outcomes were compared between the two sexes in the study population using binary logistic regression. The relationship between female sex and study outcomes was determined using multivariable logistic regression analyses, after correction for potential baseline confounders. A multivariable cox proportional hazards regression model was used to assess potential sex differences in all-cause readmission rate and to control the potential baseline confounders. All statistical analyses were performed using SPSS version 29.0 software.
Results
Characteristics of patients undergoing CAG and/or PCI
Among the 3,340 patients undergoing CAG and/or PCI enrolled, the mean age was 65 years, 922 (27.6%) patients were female (mean age: 65.8 versus 63.3 years, p < 0.001), and a total of 1,961 (58.7%) patients were undergoing CAG with PCI treatment (404 [20.6%] females, mean age: 68.1 versus 63.1 years, p < 0.001). The study population consisted primarily of patients who were first-time hospitalizations. Among the patients, 73.4% of patients (n = 2453) suffered from CAD, 31.7% (n = 1059) presented with MI, and 29.5% (n = 984) exhibited a combination of unstable angina. In addition, 56.1% of the patients (n = 1,874) were complicated with hypertension, whereas hyperlipidemia was present in 27.2% of the patients (n = 908). Furthermore, hyperuricemia was observed in 16.3% of the patients (n = 545), and CKD affected 10.3% of the patients (n = 343).
Compared with males, females undergoing CAG and/or PCI had a higher prevalence of chronic comorbidities, including PAH (17.9% versus 8.4%, p < 0.001), pulmonary infection (49.2% versus 33.8%, p < 0.001), and anemia (11.9% versus 9.2%, p = 0.020), which was coupled with lower odds of acute comorbidities, including AMI (17.1% versus 28.9%, p < 0.001) and unstable angina (24.8% versus 31.2%, p < 0.001). It was worth noting that the proportion of females with a history of MI (3.0% versus 7.5%, p < 0.001), PCI (9.3% versus 17.6%, p < 0.001), and CABG (1.1% versus 2.2%, p < 0.05) was significantly lower compared with males. In addition, females were more likely to have higher levels of EF (61.1% versus 59.2%, p < 0.001) and PASP (35.3 versus 33.3, p < 0.001) than males. Simultaneously, females exhibited higher levels of albumin (39.6 versus 39.2, p = 0.016) and serum lipids (all p values <0.001), but showed significantly lower levels of urea nitrogen (6.0 versus 6.5, p < 0.001) and serum creatinine (74.9 versus 97.5, p < 0.001), as well as eGFR (70.3 versus 76.4, p < 0.001). Regarding medications, compared with other medications, the proportion of females using diuretics was significantly higher than that of males (45.9% versus 31.4%, p < 0.001). Among patients undergoing CAG and/or PCI, females received fewer repeated angiography in <7 days (48.0% versus 68.7%, p < 0.001) and hydration therapy (88.7% versus 92.1%, p = 0.002), accompanied by a lower number of arterial infarcts (1.7 versus 2.3, p < 0.001) and use of contrast agents (190.6 versus 232.2, p < 0.001), than males. More details on baseline characteristics of patients are listed in Table 1.
Sex Differences in Baseline Characteristics of the Study Patients
BMI, body mass index; CAD, coronary artery disease; MI, myocardial infarction; DM, diabetes mellitus; CVA, cerebrovascular accident; PAH, pulmonary arterial hypertension; CKD, chronic kidney disease; PCI, percutaneous coronary intervention; EF, ejection fraction; CABG, coronary artery bypass graft; PA, pulmonary artery diameter; PASP, pulmonary artery systolic pressure; FBG, fasting blood glucose; BUN, blood urea nitrogen; Scr, serum creatinine; eGFR; estimated glomerular filtration rate; TC, total cholesterol; HDL-C, high density lipoprotein cholesterol; LDL-C, low density lipoprotein cholesterol; APOA, apolipoprotein A; ACEI or ARB or ARNI, angiotensin-converting enzyme inhibitor or angiotensin receptor blocker or angiotensin receptor–neprilysin inhibitor; DAPT, dual antiplatelet therapy.
Characteristics of patients undergoing CAG and PCI
There was a predominance of individuals who received PCI procedures mainly for the treatment of CAD. Similar to patients undergoing CAG and/or PCI, females undergoing PCI exhibited a higher prevalence of chronic comorbidities, including hypertension (71.5% versus 62.8%, p = 0.001), DM (44.1% versus 37.5%, p = 0.016), anemia (13.6% versus 8.0%, p = 0.001), and PAH (2.0% versus 0.8%, p < 0.05). Conversely, acute comorbidities such as AMI were less frequent in females compared with males (32.9% versus 39.2%, p = 0.020). In addition, the lower odds of females with a history of MI (5.9% versus 9.8%, p = 0.015), pneumonia (10.9% versus 15.0%, p < 0.05), and PCI (18.1% versus 22.7%, p < 0.05) was observed than males. Furthermore, females had higher levels of EF (61.2% versus 59.8%, p = 0.019) and serum lipids (all p values <0.01), but lower levels of serum creatinine (75.0 versus 92.0, p < 0.001) and eGFR (72.1 versus 79.8, p < 0.001). On average, females were more commonly treated with ACEI/ARB/ARNI than males (38.6% versus 32.6%, p < 0.05). Alternatively, the majority of patients underwent repeated angiography in <7 days, whereas no significant differences were observed in terms of hydration therapy and stent number. The details on baseline characteristics of patients are shown in Table 1.
Characteristics of patients undergoing CAG alone
Compared with patients undergoing CAG and PCI, the majority of patients undergoing CAG alone had generally lower rates of comorbidities and preexisting conditions, as well as procedural characteristics. However, it is remarkable that the incidence of PAH and pulmonary infection was significantly higher in patients undergoing CAG alone compared to those undergoing PCI, and the incidence was also significantly higher among females than males. In addition, females undergoing CAG alone exhibited higher levels of EF (61.1% versus 58.3%, p < 0.001), albumin (39.6 versus 38.0, p < 0.001), and serum lipids (all p-values < 0.001), but showed significantly lower levels of urea nitrogen (6.2 versus 7.3, p < 0.001) and serum creatinine (65.0 versus 87.0, p < 0.001). Different from patients undergoing CAG and PCI, the use of diuretics was significantly higher in females than in males (68.9% versus 59.3%, p < 0.001) compared with other medications. The detailed characteristics are displayed in Table 2.
Sex Differences in Baseline Characteristics of the Study Patients
BMI, body mass index; CAD, coronary artery disease; MI, myocardial infarction; DM, diabetes mellitus; CVA, cerebrovascular accident; PAH, pulmonary arterial hypertension; CKD, chronic kidney disease; PCI, percutaneous coronary intervention; EF, ejection fraction; CABG, coronary artery bypass graft; PA, pulmonary artery diameter; PASP, pulmonary artery systolic pressure; FBG, fasting blood glucose; BUN, blood urea nitrogen; Scr, serum creatinine; eGFR; estimated glomerular filtration rate; TC, total cholesterol; HDL-C, high density lipoprotein cholesterol; LDL-C, low density lipoprotein cholesterol; APOA, apolipoprotein A; ACEI or ARB or ARNI, angiotensin-converting enzyme inhibitor or angiotensin receptor blocker or angiotensin receptor–neprilysin inhibitor; DAPT, dual antiplatelet therapy.
Multivariable analysis of sex differences in study outcomes
We conducted a multivariate regression analysis to systematically assess sex differences of the three groups. The variables in Table 1 or Table 2 that conformed to colinear diagnosis and statistically significant (p < 0.05) were included in the multivariable regression model, and the assignment of categorical variables is shown in Supplementary Table S1. Of these, TC was not included in the model due to collinearity (variance inflation factor >5).
In the multivariable regression analysis, we found that the unadjusted incidence of CIN in patients undergoing CAG and/or PCI was 13.1%, and it occurred more frequently in females (20.8% versus 10.2%, p < 0.001). After controlling for all possible confounders (age, smokers, BMI, CAD, MI, unstable angina, hypertension, hyperlipidemia, hyperuricemia, anemia, PAH, pulmonary infection, prior MI, prior PCI, prior CABG, diuretics, ACEI/ARB/ARNI, β blockers, statins, DAPT, number of infarcted arteries, repeated angiography in <7 days, hydration therapy, contrast volume, EF, PASP, albumin, BUN, Scr, eGFR, HDL-C, LDL-C, APOA), the result validated that female sex was associated with an increased risk of CIN (aOR 1.47; 95% CI 1.08–2.01; p = 0.015) (Table 3). We further performed a subgroup analysis of major high-risk patients and found that pulmonary infection and the use of preoperative diuretics were independent positive predictors for CIN, whereas BMI (≥23.98) and the use of preoperative DAPT were protective factors (Fig. 2). Interestingly, the unadjusted all-cause readmission rate was lower for females than for males (20.2% versus 27.0%, p < 0.001). However, after adjusting for confounding factors, females demonstrated a higher readmission rate (aOR 1.26; 95% CI 1.02–1.56; p = 0.031) (Table 3). Through our subgroup analysis of major high-risk patients, we also further found hypertension, PAH, repeated angiography in <7 days, and the use of preoperative DAPT as independent positive predictors for the all-cause readmission rate, while prior PCI and HDL-C (≥1.02) were protective factors (Fig. 3). However, other results were not further confirmed after controlling for all possible confounders (Table 3).

Predictors of CIN in patients undergoing CAG and/ or PCI. Forest plot for the effect sizes of individual predictors of CIN in patients undergoing CAG and/ or PCI. CIN, contrast-induced nephropathy; CAG, coronary angiography; PCI, percutaneous coronary intervention.

Predictors of all-cause readmission in patients undergoing CAG and/ or PCI. Forest plot for the effect sizes of individual predictors of all-cause readmission in patients undergoing CAG and/ or PCI. CAG, coronary angiography; PCI, percutaneous coronary intervention.
Table 3. The Risk of CIN and Clinical Outcomes in Female Patients Undergoing CAG and/or PCI
Multivariate model adjusted for all possible confounders listed in Table 1.
CIN, contrast-induced nephropathy; MACE, major adverse cardiovascular events; AMI, acute myocardial infarction; AHF, acute heart failure.
Table 4. The Risk of CIN and Clinical Outcomes in Female Patients Undergoing CAG with PCI
Multivariate model adjusted for all possible confounders listed in Table 1.
CIN, contrast-induced nephropathy; MACE, major adverse cardiovascular events; AMI, acute myocardial infarction; AHF, acute heart failure.
The Risk of CIN and Clinical Outcomes in Female Patients Undergoing CAG Alone
Multivariate model adjusted for all possible confounders listed in Table 2.
CIN, contrast-induced nephropathy; MACE, major adverse cardiovascular events; AMI, acute myocardial infarction; AHF, acute heart failure.
Among patients undergoing CAG with PCI, the unadjusted incidence of CIN was higher in females (6.4% versus 3.7%, p = 0.017), whereas the incidence of AMI was slightly lower (32.9% versus 39.2%, p = 0.020), compared with males (Table 4). However, after adjusting for baseline confounding factors, there were no statistically significant differences observed in the multivariable analysis (Table 4). Notably, in contrast to patients undergoing CAG with PCI, females undergoing CAG alone demonstrated a higher incidence of severe arrhythmia compared with males (47.3% versus 40.4%, p = 0.012) in the unadjusted analysis. The result remains even after controlling for a variety of potential confounders (aOR 1.52; 95% CI 1.12–2.04; p = 0.006) (Table 5). Through our subgroup analysis, we further identified CKD, PAH, hyperuricemia, repeated angiography in < 7 days, PA (≥21.90), and the use of preoperative statins as independent positive predictors for severe arrhythmia, whereas EF (≥61.90) was found to be a protective factor (Fig. 4).
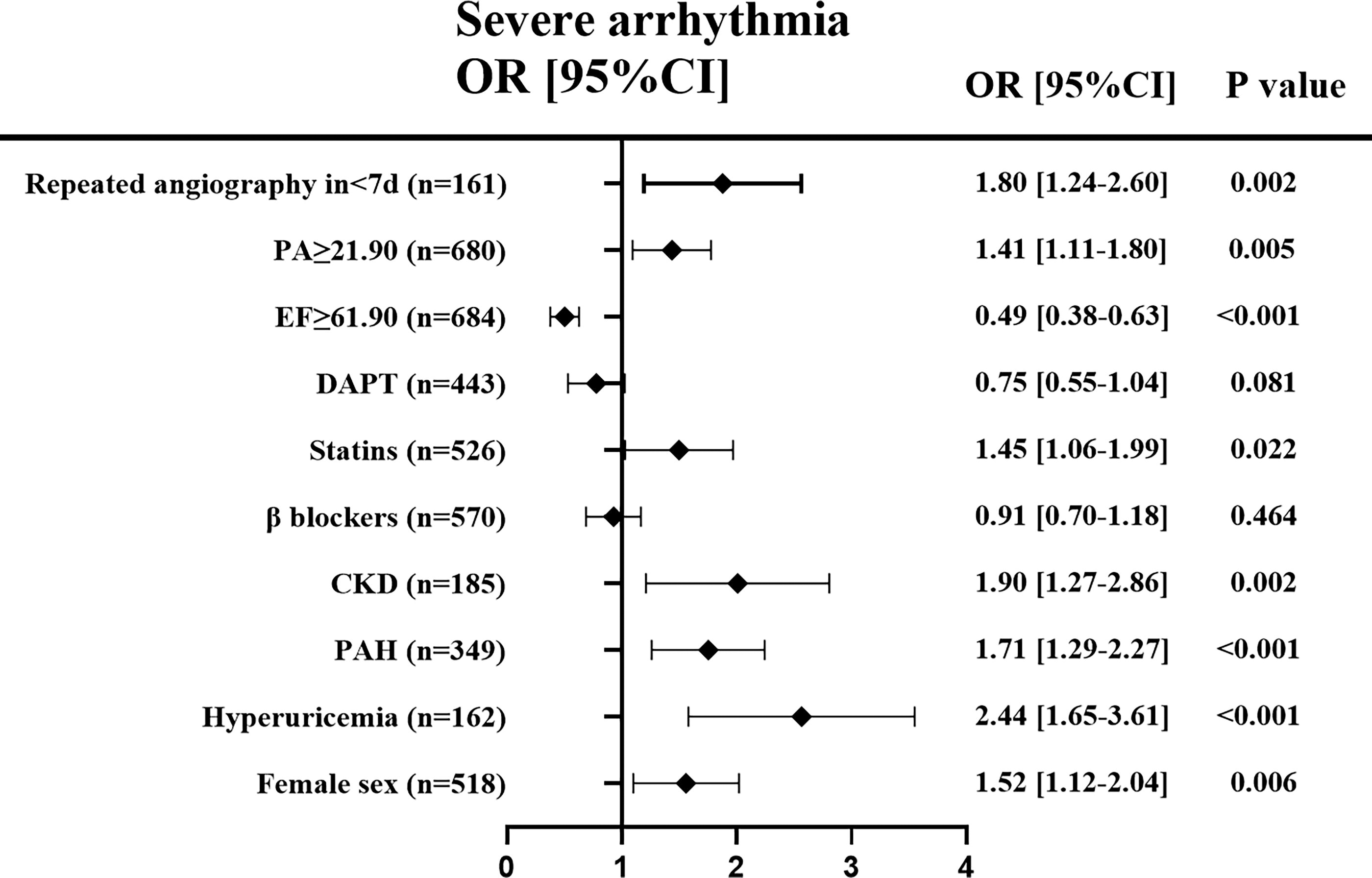
Predictors of severe arrhythmia in patients undergoing CAG alone. Forest plot for the effect sizes of individual predictors of severe arrhythmia in patients undergoing CAG. Note: color should not be used when printing. CAG, coronary angiography.
Discussion
Our study systematically evaluated sex differences in clinical characteristics, treatments, the risk of CIN, and clinical outcomes among patients undergoing CAG and/or PCI. To the best of our knowledge, this study is the largest study to evaluate sex differences in the risk of CIN among patients undergoing CAG and/or PCI in China. Previous studies have indicated that females tend to exhibit a higher age and burden of complications, while experiencing limited access to PCI compared with males. 11,18 –20 However, the current body of evidence regarding the existence of sex differences in clinical characteristics, treatments, risk of CIN, and clinical outcomes among patients undergoing CAG and/or PCI remains controversial or limited, necessitating further confirmation.
In the present study, we found that females undergoing CAG and/or PCI tended to be older, have a higher prevalence of chronic comorbidities, including PAH, pulmonary infection, and anemia, which was accompanied with lower odds of acute comorbidities such as AMI and unstable angina. In addition, females were less likely to undergo revascularization or timely reperfusion compared with males. These results are comparable to several prior studies. 11,13,21,22 Indeed, females are more prone to pulmonary infections compared with males, which may be attributed to the fact that females tend to be older than males. Our study revealed that a lower proportion of females presented with chronic conditions such as hypertension, DM, and CKD, which is distinguished from other studies. 13,23 This may be partly due to selection bias or regional disparity. Notably, BMI was similar for males and females, the levels of EF, PASP, and serum lipids were higher in females, whereas eGFR was lower than males. These findings of our study are in agreement with prior studies. 13,20 We further found that compared with males, females with CAD undergoing CAG and/or PCI had similar procedural characteristics and they less often received guideline-directed medications, which is consistent with other studies. 18,24 The reason may be related to the low usage of medications that lower compliance to secondary prevention measures in females with advanced age, resulting in fewer females adhering to drug therapies. 11
Similar to patients undergoing CAG and/or PCI, chronic comorbidities such as PAH and anemia were common problems in patients undergoing CAG with PCI. Nevertheless, the difference was that females undergoing PCI showed a significantly higher prevalence of chronic comorbidities, including hypertension and DM, which is in line with Kosmidou et al. 23 Moreover, our study indicated that the rates of prior CAD (MI, PCI) and pneumonia were lower in females with CAD than in males. It is presumable that the former may suggest the underestimation of CAD severity in females, 13 whereas the latter is predominantly related to age and disease conditions in females rather than smoking. Interestingly, females undergoing PCI were more frequently treated with ACEI/ARB/ARNI compared with males; similar findings were reported in previous studies, 20,25 which is inconsistent with other findings. 26,27 The difference may be explained by the diverse study population and differing study designs.
In our study, we found that patients undergoing CAG alone exhibited a comparatively milder disease profile in contrast to those undergoing CAG with PCI. However, notable disparities were evident in the outcomes related to pulmonary infection and PAH. The reason may be related to the abnormality of pulmonary artery, such as pulmonary artery dilation and increased pulmonary artery systolic pressure. It is worth noting that the proportion of females utilizing diuretics was significantly higher than that of males compared with patients undergoing CAG with PCI, which is consistent with other studies. 6,10 The utilization of preoperative diuretics has been observed to augment the nephrotoxicity associated with renal tubular injury, thereby elevating the prevalence of CIN. 28
It is worthy of special attention for the risk of CIN and clinical outcomes in patients undergoing CAG and/or PCI. Notably, the occurrence and progression of CIN are associated with numerous factors, 5 –7,9 among them, the interpretation of CIN by sex-based differences is still controversial. Our findings revealed that the unadjusted incidence of CIN in females undergoing CAG and/or PCI was preeminently higher than in males (20.8% versus 10.2%, p < 0.001), in addition to female sex itself, which may be partly related to the worse clinical profile such as advanced age, a high burden of complications, and low rates of treatments in females. Prior research also found that female sex is an independent predictor of a higher risk of CIN, however, it has demonstrated conflicting findings after controlling for all possible confounders. 6,8,10 Contrary to prior findings, a meaningful result was obtained after controlling for all possible confounders in this study, which also further confirms the significant association between female sex and an increased risk of CIN.
Interestingly, we further found that pulmonary infection and the use of diuretics were independent positive predictors of CIN compared with other studies. 5,7 One possible explanation is that when patients are complicated with pulmonary infection during hospitalization, renal ischemia and hypoxia are likely to be aggravated, leading to renal hypoperfusion; meanwhile, the use of diuretics can affect the extracellular fluid balance in renal tubules and further impair renal function, increasing the risk of CIN. 5,29 In parallel, the findings of our subgroup analysis demonstrated that BMI (≥23.98) and the use of preoperative DAPT were protective factors for CIN, which is similar to other studies. 30,31 On the one hand, an increase in eGFR with increasing BMI, which can improve renal reabsorption of sodium, and have a protective effect on the kidneys, may reduce the occurrence of CIN. However, excessive obesity (BMI ≥ 30) may exacerbate the development of CIN. 32 On the other hand, the utilization of preoperative DAPT may have a protective effect on the occurrence of CIN; however, the result is likely to be influenced by drug–drug interactions.
Readmission rate is considered an important indicator of the quality of medical care, and the higher the readmission rate, the higher the morbidity and hospitalization costs. 14,33 The results of our study demonstrated that the all-cause readmission rate for females was higher than that for males after controlling for all possible confounders. Indeed, through our subgroup analysis, we further uncovered hypertension, PAH, repeated angiography in <7 days, and the use of preoperative DAPT as independent positive predictors for the all-cause readmission rate, whereas prior PCI and HDL-C (≥1.02) were identified as protective factors, which is in line with other studies. 34,35 Similar to our findings, Lam et al. evaluated gender differences in the 30-day readmission rate and found a crude 30-day readmission rate of 13.9% in women and 9.6% in men among 583 acute coronary syndrome (ACS) patients undergoing PCI. 14 Another study also showed that females with ACS who underwent PCI were more likely to experience higher rates of 2-year rehospitalization. 26 In contrast, Worrall-Carter et al. demonstrated that a lower odds of 2-year rehospitalization was observed in females with ACS who received PCI compared with males. 36 Therefore, further confirmation is needed to determine whether female sex has a different effect on short- and long-term readmission rates.
We further found that female sex was an independent risk factor for severe arrhythmia in patients undergoing CAG alone. Females exhibited a higher prevalence of severe arrhythmia compared with males, with an increasing incidence observed in correlation with advancing age, in agreement with other studies. 37,38 The results of our subgroup analysis on high-risk populations revealed PAH, CKD, hyperuricemia, repeated angiography in < 7 days, PA (≥21.90), and the use of preoperative statins as independent positive predictors for severe arrhythmia, whereas EF (≥61.90) was identified as a protective factor. Similar results were found in other studies. 39,40 The reasons are that long-term PAH, persistent elevation of blood uric acid levels, and accumulation of renal toxins will result in increased ventricular volume and pressure load, thereby inducing heart failure and consequently increasing the incidence of arrhythmia. In contrast to previous studies, 41 our study identified the preoperative utilization of statins as a significant risk factor for arrhythmia, potentially attributed to variations in drug dosage and drug–drug interactions. Therefore, the role of lipid-lowering therapy in the prevention of arrhythmia necessitates further discussion.
Limitations
Several limitations should be noted in our study. First, our study included only patients who underwent CAG and/or PCI, so it may not represent the whole CAD population. In addition, the study was conducted as a single-center study, which could hamper the generalizability of the findings. Despite these limitations, our study is the largest study on the risk of CIN between the two sexes among patients undergoing CAG and/or PCI in China. It systematically assesses sex differences in clinical characteristics, treatments, the risk of CIN, and clinical outcomes among patients undergoing CAG and/or PCI, providing important reference evidence for future work.
Conclusion
Female sex is an independent predictor that can influence clinical characteristics, treatments, the risk of CIN, and other clinical outcomes to varying degrees in patients undergoing CAG and/or PCI. In summary, females exhibit advanced age, a higher burden of complications, an increased risk of CIN, and generally poorer prognosis compared with males, along with limited treatment opportunities. Therefore, it is of great necessity to highlight early risk assessment and prevention for females who received CAG and/or PCI, so as to improve their prognosis.
Footnotes
Acknowledgements
Ethics Approval
Ethics Approval was obtained from the Fujian Medical University Union Hospital Ethics Committee (2023KY032) prior to data collection, and informed consent was obtained from either the patients’ guardians or the patients themselves.
Authors’ Contributions
X.H., B.L., S.L., F.L., Q.L., Q.Y., L.C., Y.L.: Study design and data acquisition. X.H., B.L., Y.P., F.Y.: Analysis and interpretation of data. X.H. and B.L.: Writing original draft. X.H., B.L., Y.P., F.Y., L.C., Y.L.: Critically revising the article for important intellectual content. X.H., B.L., Y.P., F.Y., S.L., F.L., Q.L., Q.Y., L.C., Y.L.: Final approval of the version to be published.
Author Disclosure Statement
The authors declare no conflict of interest.
Funding Information
This study was supported by the fund of
Supplementary Material
Supplementary Table S1
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.