
Abstract
Background:
Intimate partner violence (IPV) has negative health impacts for pregnant people and their infants. Although inpatient postpartum units offer an opportunity to provide support and resources for IPV survivors and their families, to our knowledge, such interventions exist. The goal of this study is to explore (1) how IPV is currently discussed with postpartum people in the postpartum unit; (2) what content should be included and how an IPV intervention should be delivered; (3) how best to support survivors who disclose IPV; and (4) implementation barriers and facilitators.
Materials and Methods:
We used individual, semistructured interviews with postpartum people and health care providers (HCPs). Interview transcripts were coded and analyzed using an inductive-deductive thematic analysis.
Results:
While HCPs reported using a variety of practices to support survivors, postpartum people reported that they did not recall receiving resources or education related to IPV while in the inpatient postpartum unit. While HCPs identified a need for screening and disclosure-driven resource provision, postpartum people identified a need for universal IPV resource provision in the postpartum unit to postpartum people and their partners. Participants identified several barriers (i.e., staff capacity, education already provided in the postpartum unit, and COVID-19 pandemic) and facilitators (i.e., continuity of care, various HCPs) to supporting survivors in the postpartum unit.
Conclusion:
The inpatient postpartum unit is a promising setting to implement an intervention to support IPV survivors and their infants. Future research and intervention development should focus on facilitating universal education and promoting resource provision to IPV survivors.
Introduction
Intimate partner violence (IPV) is a pervasive public health epidemic for pregnant and postpartum people. 1,2 IPV is fundamentally rooted in power and control, with partners using an array of controlling and coercive behaviors and tactics to manipulate, harass, or control an intimate partner. 3,4 Examples of IPV include psychological, physical, financial, sexual, or immigration-related abuse, sexual coercion, stalking, among others. 3,5 The prevalence of IPV for pregnant and postpartum people is high, and varies depending on the group and type of IPV assessed. A systematic review conducted in the United States estimated that 8% of pregnant people experience physical or sexual IPV, with prevalence notably higher among cross-sectional samples of postpartum people who live in rural areas (20%) and use substances (19%). 6 –8
In addition, using data from the violent death reporting system, prior research found that nearly half of suicides and homicides of pregnant people involve IPV. 9 Pediatric, family medicine, and women's health organizations describe the importance of supporting IPV survivors through education and resource provision during the perinatal period. 3,10 One powerful framework for supporting IPV survivors is healing-centered engagement, which is a strengths-based approach where health care providers (HCPs) create safe and nonjudgmental spaces for IPV survivors.
Healing-centered engagement recognizes that IPV survivors are experts in their own experiences, and encourages HCPs to work with survivors on solutions that best reflect their own needs. The American Academy of Pediatrics updated IPV policy statement recommends use of a healing-centered approach in health care settings. 3,11
Although the perinatal period may make people more vulnerable to IPV, it also offers a unique opportunity to support survivors. 12 People are more likely to attend prenatal visits compared with yearly examinations, and prior research has identified perinatal visits as an opportunity to address IPV. 13 –16 The majority of research to date has focused on IPV screening in outpatient settings. 15 –18 However, these studies also identified barriers to addressing IPV in the outpatient setting, including lack of time, provider training, and provider knowledge of available resources. 19
Fewer studies have focused on utilizing the immediate postpartum period as a time to assess for IPV, provide resources, and support survivors. Postpartum people spend 2–4 days in the postpartum unit, where they initiate breastfeeding, begin bonding with their infant, and have access to HCPs. While postpartum people are in the postpartum unit, they may receive education on a variety of topics, including safe sleep practices and postpartum depression. 20,21 The postpartum unit may also be a safe place for survivors to talk about IPV and get needed support. It may also be easier to implement IPV-focused education and connection to resources compared with outpatient visits that are limited by time. However, to our knowledge, no IPV interventions have been developed within the postpartum unit. Further, there may be unique implementation barriers and facilitators in the postpartum unit as compared with other settings.
The goal of this study is to examine the perspectives of postpartum people and HCPs (i.e., postpartum nurses, physicians, lactation consultants, and social workers) in the United States regarding how to address IPV and support survivors in the postpartum unit. Our specific aims examine (1) how IPV is currently discussed in the postpartum unit; (2) what content should be included and how the intervention should be delivered; (3) how best to support survivors who disclose IPV; and (4) implementation barriers and facilitators.
Materials and Methods
We conducted individual, semistructured interviews with HCPs (physicians, nurse practitioners, registered nurses, social workers) and postpartum people who recently gave birth to explore their perspectives on how best to address IPV in the postpartum unit. The study took place at a large, academic hospital in a midsize city in the Northeast. The University of Pittsburgh Institutional Review Board approved the study. The virtual interviews took place from November 2021 to August 2022.
Materials
The study team members developed interview questions based on study aims. Interview questions addressed the following: (1) how IPV is currently discussed with postpartum people in the postpartum unit; (2) what content should be included and how education around IPV should be delivered; (3) how best to support postpartum people who disclose IPV; and (4) implementation barriers and facilitators. Separate interview guides were developed for HCPs and postpartum people.
Participants and recruitment
Eligibility criteria for postpartum people included the following: (1) age ≥18; (2) delivered at the participating hospital 0–4 months before the interview; and (3) speaks and understands English. We choose 0–4 months, so that postpartum people could remember and reflect on their birthing experience, but wanted to allow enough time so participants would not have to complete the interview immediately after giving birth. Eligibility criteria for HCPs included (1) age ≥18, (2) HCP at the participating hospital; and (3) speaks and understands English. As we were interested in hearing how IPV should be discussed in the postpartum setting more broadly, experiencing IPV was not part of the inclusion criteria.
Study team members (Erin Mickievicz and M.R.) recruited postpartum people from three locations: (1) at a large pediatric academic clinic during 0- to 4-month well-child visits; (2) immediately postpartum in the postpartum unit; and (3) through Pitt + Me, an online recruitment portal. Using convenience sampling, we recruited HCPs through email, discussing the study at team meetings, and word of mouth. Interested participants were contacted by the study team to provide verbal consent and schedule an interview.
Data analysis
Interviews were conducted via Zoom and lasted 45–60 minutes. Interviews were audio recorded and transcribed. Deidentified transcripts were coded and managed using Dedoose qualitative software. We chose a qualitative descriptive approach to perform thematic analysis. 22,23 We created a preliminary codebook using general topics addressed by our interview guide. Two coders independently coded each transcript using this codebook and adding new codes in an inductive manner. They then met to review their coding and refine the codebook in an iterative fashion.
Once no new codes were added, the final codebook was then reapplied to all transcripts. Transcripts were coded independently, and coders met twice to discuss emerging codes and resolve discrepancies. The full team met twice throughout the data analysis process to consolidate codes into emerging themes and make iterative changes to the interview guide based on inductive guides (e.g., adding a question about how to include partners in IPV education). We continued with interviews until thematic saturation was reached, when we heard no new codes or themes, for both participant groups. 24
Results
Thirty participants completed interviews including 14 HCPs and 16 postpartum people (Table 1). Postpartum participants were predominantly ages 30–34 (31%), and all identified as cis-gender female. Most HCPs identified as cis-gender female (93%) and white (79%). Two domains emerged: (1) need, content, and delivery of IPV resources in the postpartum unit; and (2) barriers and facilitators to implementation. In quotations in the subsequent sections, PP refers to a quotation from a postpartum person and HCP from a HCP.
Demographics
Participants could select more than one option.
HCP, health care provider.
To be inclusive of all birthing experiences, the authors use gender-affirming language throughout this article. The authors specifically refer to birthing people as “postpartum people.” To honor the voices of our participants, the authors did not change any quotes; many participants use gendered language (i.e., “mom” or “mother”) when referring to postpartum people. Table 2 includes additional representative quotations.
Representative Quotes
CPS, Child Protective Services; IPV, intimate partner violence.
Domain 1: need, content, and delivery
Theme 1. Postpartum people are often asked about their IPV experiences but are not universally provided education or resources around IPV
HCPs shared a variety of practices around addressing IPV in the postpartum unit, including asking about the patient's home situation and looking at the patient's chart to see if safety concerns arose during prenatal visits. Postpartum people reported that they were asked about IPV during prenatal visits and upon initial intake (usually asked about feeling safe at home), but not provided additional information around IPV while in the postpartum unit: “Basically the standard conversation. Do you feel safe at home? Are you experiencing any domestic violence?” (PP07). Another postpartum person discussed her experience with screening during her prenatal appointment: Even though I was with my husband, they asked him to stay outside… The reason why they did that, I suppose, because they wanted to ask those domestic violence questions, making sure that I felt safe. (PP06)
Both postpartum people and HCPs shared that provision of education or resources around IPV was limited to those who disclosed or who were deemed to be “high risk”: “It's just basically reaching out to social work. I wish it didn't all fall on social work, but we try to reach out to social work and utilize them because they know… the extra resources” (HCP03). Speaking about resource provision after disclosure, one HCP said, “It's been maybe one in the last five years that actually disclosed, like, ‘I am not in a safe relationship’, and we actually got her taken from the hospital away from the dad, but I don't know what happened on follow up” (HCP02). Likewise, patient participants indicated that they did not recall receiving any general IPV information: “nobody talked to me about my relationship” (PP16).
Theme 2. Desire for IPV information and resources that covered a variety of IPV types and manifestations
HCPs and postpartum people identified a need to educate and provide resources on multiple types of IPV. Participants spoke about how postpartum people might not recognize IPV that is not physical or might not feel comfortable seeking help. One HCP said, “But a lot of people, they don't take emotional, mental—you know, the controlling—those type abuse symptoms as serious, and they are” (HCP13). One HCP spoke about the importance of including sexual coercion in education: I have had a few moms reveal to me that, in the postpartum period, that, at the time where their doctors are telling them, “You should not be having sex because you need to heal,” a lot of dads are pushing, pushing, pushing, pushing, and there's a lot of pressure there. (HCP02)
Theme 3. Considerations of partner involvement and presence
Postpartum people identified a need for partners to be involved in IPV prevention and education, but HCPs worried about the safety if the partner is included. An HCP said, It would make me uncomfortable in a situation where I know that the partner was the perpetrator to be able to say, “Here's the resources” and include domestic violence resources. Is he gonna retaliate because she disclosed something that he didn't want her to disclose? (HCP05)
Postpartum people thought the potential benefits of intervention including partners outweighed safety risk. Postpartum people also thought it was necessary to have resources available for partners who use violence. One postpartum person said, …that I'm not also making the assumption that the only options are to leave or not. Maybe part of it is their opportunity for change or to get treatment or for help …If it's at a point where somebody's like, “I've exhibited some of these signs and behaviors and words,”…, maybe it's also like, “Hey, here's some treatment options for you.” (PP11)
Theme 4. Desire for universally distributed IPV education
Most HCPs advocated for screening, as they expressed uncertainty around how to prioritize resource provision with knowing who is at risk: Well, I think screening would be really helpful… just really making sure they're screening to make sure moms feel safe, and that they don't—if they want help, they have it. (HCP14)
HCPs had several hesitations to implement IPV screening in the postpartum unit, including safety and potential lack of comfort with the setting and individual conducting the screen: I noticed in labor and delivery whenever we admit the patients in the admission assessment there's a question of like, “Do you feel safe at home?” … most people don't ask in private. I feel like there isn't really an opportunity for people to safely say no. (HCP08)
Postpartum people identified a need for resources to be provided to all parents, regardless of disclosure or screening results, and that some postpartum people may need resources in the future or to give to someone they know: “Just give the resources. That's the biggest thing. ‘Cause a lot of people, when those things are happening, they don't really have anybody… Just the resources is the biggest thing for me.” (PP02)
HCPs did not bring up universal education or resource distribution, but several answered affirmatively when asked if resources and education should be universally distributed. Several resources were shared to be universally distributed to postpartum people and partners, including food pantries, shelters, housing resources, counseling services, financial resources, IPV hotlines and text lines, and relevant support groups.
When asked about the best method for distributing these resources, participants mentioned the online health portal, videos, and links in discharge instructions. Participants noted that if a disclosure occurs, patients should be referred to the wrap-around services, and HCPs in the postpartum unit should facilitate follow-up with the postpartum provider.
Domain 2: barriers and facilitators
HCPs and postpartum people identified several barriers to addressing IPV in the postpartum unit, including institutional barriers such as understaffing and lack of training, knowledge barriers, and barriers related to the realities of the postpartum unit. Several facilitators were also noted, including staff training, continuity of care during the perinatal period, and opportunities to speak to the patient alone.
Theme 1. Need for standardized HCP training and care procedures
HCPs noted variation in provider practice and not understanding how to best support postpartum people experiencing IPV. HCPs suggested that having a standardized resource pamphlet to give to patients or instruction in EHR may help standardize care. HCPs also noted that staff may forget to discuss IPV or provide resources or may not know what to do if someone discloses IPV: Then, sort of lack of knowledge of what to do if they told us something's going wrong. … I do know that [community resource] is another resource too… but what to do after that, other than get social work involved, I don't have a great wheelhouse. (HCP02)
HCPs expressed uncertainty around best practices when documenting IPV in the postpartum person's and baby's charts. They identified possible improved coordination of care between HCPs in obstetrics, the postpartum unit, and pediatrics if IPV was documented in the EHR. However, HCPs noted safety concerns of documenting IPV in charts if they did not document in a secure note.
Theme 2. Limited staff capacity
HCPs spoke about the institutional barriers to supporting postpartum people experiencing IPV, including lack of time per patient and understaffing: “Again, it's the time situation and the ratios for postpartum care that just makes it impossible” (HCP13). Postpartum people and HCPs spoke about certain HCPs like lactation consultants who may have additional time with each patient, and it may be more feasible for them to deliver interventions.
Theme 3. Information exchange throughout the perinatal period
HCPs discussed the overwhelming amount of information shared, including feeling like there are too many papers and information shared with new parents: “I think that's a hard question because, even if they would get like more paperwork—because they get a lot of papers while they're there in the hospital.” (HCP03)
HCPs and postpartum people spoke about the importance of multiple points of resource delivery including on bulletin boards, television screens, and discharge paperwork: “I think posters and bulletin boards in common spaces is probably a good touch point …I think in the common points, and probably part of the discharge packet, some sort of paper, flyer.” (HCP04)
Both postpartum people and HCPs also spoke about the importance of continuity of care in providing support for postpartum people experiencing IPV. HCPs noted that if done with attention to confidentiality, the EHR has potential to improve coordination of care between providers in obstetrics, social work, pediatrics, and on the postpartum unit: If they're already hooked up, pre-delivery, through the OB offices… then if they are coming back to us, specifically, I guess just ensuring that they are connected and getting the necessary follow-through …Occasionally, they [social work] will maybe call us, but they'll typically just put their note in the chart that there is something more significant as far as the conversation that we need to help follow-through for the baby. (HCP04)
Postpartum people shared that this continuity of care aided in building trust and safety with HCPs: “I just wish that there would've been more time to talk to her [postpartum unit HCP], because I started building—when we were talking, I felt safe talking to her.” (PP02)
Theme 4. Logistical challenges speaking to the postpartum person
HCPs also spoke about a variety of barriers related to the realities of the postpartum unit, particularly speaking to patients alone without their partners, family members, or children. As an example, an HCP spoke about the lack of a safe space for older children to go to during private conversations with the postpartum person, which inhibits HCPs from discussing IPV confidentially: If they're infants, you can have a conversation ‘cause they may hear it, but they're not really discerning anything, but even a three-year-old hears something that can be challenging because how they understand what you might have talked about… The space and time is a little bit challenging sometimes. (HCP04)
HCPs spoke about social workers as a facilitator to speaking to postpartum people alone by giving the partner or other family members a task that required them to leave the room.
Postpartum people identified several barriers to disclosure, including shame, fear of Child Protective Services involvement, safety concerns for themselves or their children, and pervasiveness of trauma: “I think a lot of times people, either individuals who have dealt with them [social workers] in the past for negative reasons or people who, like me, I'm just educated, and I'm—I overthink things.” I'm like, “If I say the wrong thing, they're gonna take my kid away” (PP06). Another postpartum person spoke about shame and embarrassment as barriers to disclosure: I would say probably go to every room because if there's—if it's a thing where somebody might be maybe scared to speak up or embarrassed. Plus now, there's a baby. They might have a lot of fears about if somehow it could maybe make them look bad as a mother. (PP01)
Another postpartum person spoke about how a survivor might not disclose because they would be afraid that their only option would be to leave their partner: Just one more thought too which is, that I'm not also making the assumption that the only options are to leave or not. Maybe part of it is their opportunity for change or to get treatment or for help … Maybe the answer is not just automatically somebody leaves or not. I think having all of those options available and certain resources just depending on what is being shared. (PP11)
Theme 5. COVID-19 pandemic
HCPs also noted several barriers related to the COVID-19 pandemic, including decreased time from delivery to discharge, difficulty speaking with patients alone, and increased staff turnover. HCPs explained that with the COVID-19 pandemic time to discharge is often 24 hours, and expressed concern that there would be enough time to “fit another thing in.” One HCP explained, I think that it should be targeted more towards when you go home just because with COVID as well. We used to keep our vaginal deliveries for two days and our c-section deliveries for three days, but with COVID they've been letting people go home. Sometimes after 24 hours of delivery they're going home already. I feel like we're not having them in the hospital that long anymore. (HCP08)
Discussion
To our knowledge, this is the first study to explore the perspectives of postpartum people and HCPs on how IPV should be addressed in the postpartum unit. The perinatal period is a particularly important time for IPV-related interventions as prenatal and postpartum people are at increased risk of violence and are often in more frequent contact with health care. 25,26 Although interventions exist to support IPV survivors during the prenatal and postpartum period, 27,28 including at prenatal appointments, no interventions exist within postpartum units. Results from our study demonstrate a need to address IPV within postpartum units, and provide guidance on intervention content and delivery.
While HCPs noted the importance of screening, postpartum people reported that resource provision should be universal as survivors may not disclose IPV due to sigma, fear of Child Protective Services (CPS) involvement, or safety concerns. This finding is aligned with previous qualitative work from postpartum units of two delivery hospitals, which showed that survivors may not disclose to HCPs due to fear of violence escalation or criminalization of their partner. 25 It also reflects studies noting that positive IPV screening rates in health care settings are often <10%, in contrast to nationally representative data showing that ∼50% of women have experienced IPV. 29
Our study extends this work to note unique concerns in the pediatric health care settings, particularly around CPS involvement. Among IPV survivors using the National Domestic Violence hotline, one in three survivors did not report their experiences due to fear of mandated reporting, and 50% noted that mandated reporter involvement made their situation much worse. 30 Fear of CPS involvement may be compounded during the perinatal period, during which people are often surveilled for risk factors, interact frequently with health care, and may be more likely to have a report filed against them. 31
Postpartum people also highlighted a desire to include partners in IPV-related education and interventions. Standard of care as dictated by multiple professional organizations is to provide any IPV screening or intervention to women alone, without the partner, verbal children, or other family members. Such practices are necessary to ensure survivors can comfortably and confidentially talk about their experiences.
Compared with adult health care settings, the issue of partner presence may be more commonly encountered in pediatric health care settings because other caregivers may be involved and present during their child's hospitalizations and outpatient visits. Use of universal resource provision, rather than screening, may be a strategy to provide support and services to more families in pediatric care settings, and offer opportunity to focus on relational health and bolster survivor's social supports. Future work is needed to determine how to safely provide partners education around IPV.
The impact of COVID-19 on health care delivery systems was discussed as a potential barrier to supporting survivors. COVID-19 rapidly shifted health care delivery, catalyzed a move to virtual service provision, decreased in-person interactions with health care systems, and created staffing shortages. 32,33 Past work demonstrated how COVID-19 served as a mechanism for abusive partners to control survivors (e.g., limiting access to nonhousehold supports under the guise of mitigating COVID-19 risk). 34,35 COVID-19 also radically shifted victim service agency service delivery to provide more virtual and flexible services. 36 As systems re-equilibrate during the current stage of the pandemic, there may be opportunity to reimage healthcare delivery especially by making institutional-level changes to better prepare for emergencies.
Both HCPs and postpartum people identified several institutional- or hospital-level changes that will be required to effectively support patients experiencing IPV. These findings extend previous qualitative work examining barriers to disclosure among postpartum survivors, which found that participants recommended creating a shift in the health care system's approach toward IPV (i.e., building continuity of care during perinatal period, eliminating time constraints and understaffing), and providing support for survivors and care providers (i.e., providing HCPs training on IPV). 37
Previous work in a pediatric hospital also identified several institutional barriers such as increasing emphasis on clinical efficiency (as opposed to the time required to address IPV), lack of staff training, insufficient attention to staff vicarious trauma, and lack of social work capacity. 38 Taken together, these findings show that multilevel strategies are needed and provider education without systems-level change is not sufficient to support survivors.
This study has several limitations. HCPs were recruited from one academic medical center, and postpartum people from a single hospital and university-run recruitment repository in the Northeast. This study was conducted in the United States; due to differing clinical practices in countries outside the United States, these findings may not reflect the experiences of HCPs and postpartum people. The perspectives of these participants may not be generalizable to other clinical settings. This study did not include perspectives from transgender and nonbinary birthing people, adolescent parents, partners, or non-English–speaking communities.
Future work should include their voices in research on IPV interventions. Particularly, transgender and nonbinary people may be more likely to experience IPV, and may have different experiences than cisgender women in the postpartum unit. 39 It is critical that their voices are included in future studies concerning supporting IPV survivors in the postpartum unit. This study did not include the perspectives of obstetricians; future studies should explore their current practices and desired resources. Finally, postpartum people were not required to have experienced IPV to participate. While important to explore the perspectives of all postpartum people, there may be safety concerns related to some of the recommendations proposed by participants, including proving universal education to partners.
This study has several implications for further research and clinical innovation. Larger survey-based and longitudinal studies should explore these findings to generalize to other settings and HCPs. Given the conflicting opinions on screening, future work should elucidate the opinions of perinatal people and HCPs of screening during the perinatal period. In addition, more research is needed to triangulate these findings with postpartum people who identify as IPV survivors, particularly around inclusion of partners in IPV-focused education.
Results also have practice and policy implications. Healing-centered engagement is a powerful framework for health care systems to provide strength-based, survivor-centered care. 11,40 A potential healing-centered approach is confidentiality, universal education, and resource provision (CUES), which advocates for provision of education and resources to all patients rather than just to those who disclose IPV. 41,42 CUES also recognizes that some patients may disclose IPV, and recommends connecting them with hospital and community-based resources. This approach, which is an alternative to IPV screening and is recommended by the AAP, is aligned with participants' interest in giving resources universally. 3 Further work is needed to develop and test a CUES process that can be safely implemented and sustained in the postpartum unit.
Given considerable implementation barriers, healing-centered engagement must extend beyond the provider level to also involve a systems-level approach. Health care systems can advocate for colocated IPV advocates in postpartum units (e.g., the AWAKE program), system-wide processes to connect survivors to local resources, flyers and posters with IPV helpline numbers in the postpartum unit, training for all members of the health care team on supporting survivors, and formation of IPV workgroups to guide postpartum unit protocols around supporting IPV survivors.
Vital to creating a survivor-centered health care response to IPV is ensuring that while standard procedures for supporting IPV survivors exist within the postpartum unit, there is enough flexibility in protocols to tailor to the unique needs of each survivor. Finally, health care systems must provide financial resources to ensure sustainability of systems-level approaches. As part of this, payors must reimburse supporting survivors rather than just identifying IPV. Figure 1 shows changes that can be implemented to promote healing-centered care within the postpartum unit.
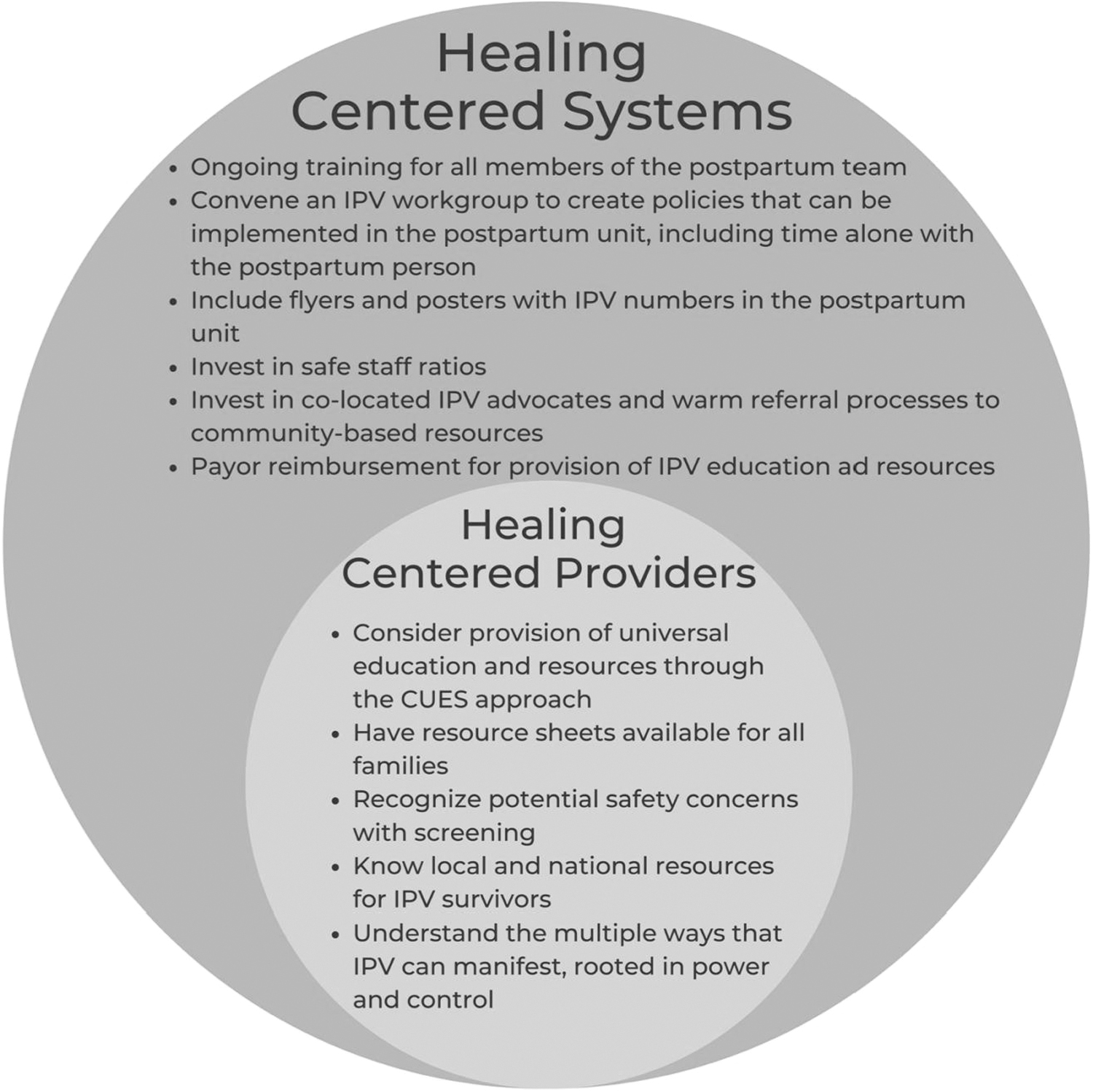
Recommendations for supporting healing-centered systems and providers. CUES, confidentiality, universal education, empowerment, and support intervention; IPV, intimate partner violence.
Conclusions
This study is one of the first, to our knowledge, to examine the perspective of postpartum people and HCPs on IPV interventions in the postpartum unit. We found that while participants identified a need for IPV intervention in the postpartum unit, HCPs require additional training and institutional support to better connect survivors with resources. IPV has lifelong health impacts for postpartum people and their infants; developing interventions for the postpartum unit will help provide the support needed to promote the well-being of postpartum people and infants.
Footnotes
Authors' Contributions
S.S. contributed to writing—original draft; writing—review and editing. G.J. assisted with writing—review and editing. Er.M. performed analysis; writing—review and editing. J.S., A.-M.R., R.L., J.C., and K.R. designed conceptualization; methodology; writing—review and editing. M.R. contributed to conceptualization; methodology; writing—original draft; writing—review and editing.
Author Disclosure Statement
El.M. receives royalties for writing content for UptoDate, Wolter Kluwers, Inc. The other authors have no conflicts of interest relevant to this article to disclose.
Funding Information
This work was supported by Amy Roberts Health Promotion Research Award. Maya Ragavan is supported by a K23 (HD104925) from the National Institute on Child Health and Human Development. Dr. Kimberly A. Randell is supported by the Eunice Kennedy Shriver National Institute of Child Health & Human Development of the National Institutes of Health under award number K23HD098299. The findings and conclusions in this report are those of the authors and do not necessarily represent the official position of the National Institutes of Health.