
Abstract

Case Summary
A
Medications include fluoxetine, buspirone, and Mirena intrauterine device placed 2 years ago. On examination, she has normal visual acuity (VA), but visual field testing shows mild enlargement of the physiological blind spots (Figs. 1 and 2). Dilated fundus examination shows grade 3 disk edema bilaterally (Figs. 3 and 4). Her neurological examination is otherwise normal. MRI of brain with contrast shows normal brain parenchyma and meninges without evidence of hydrocephalus or space-occupying lesion. However, she had a partially empty sella turcica. Magnetic resonance venography (MRV) shows mild transverse sinus narrowing bilaterally but no dural venous sinus thrombosis (DVST).

Right eye automated Humphrey visual field 24-2 test with enlarged blind spot temporally.

Left eye automated Humphrey visual field 24-2 test with enlarged blind spot temporally.

Fundus photograph of the right eye showing grade 3 disk edema, normal macula, and normal vessels.
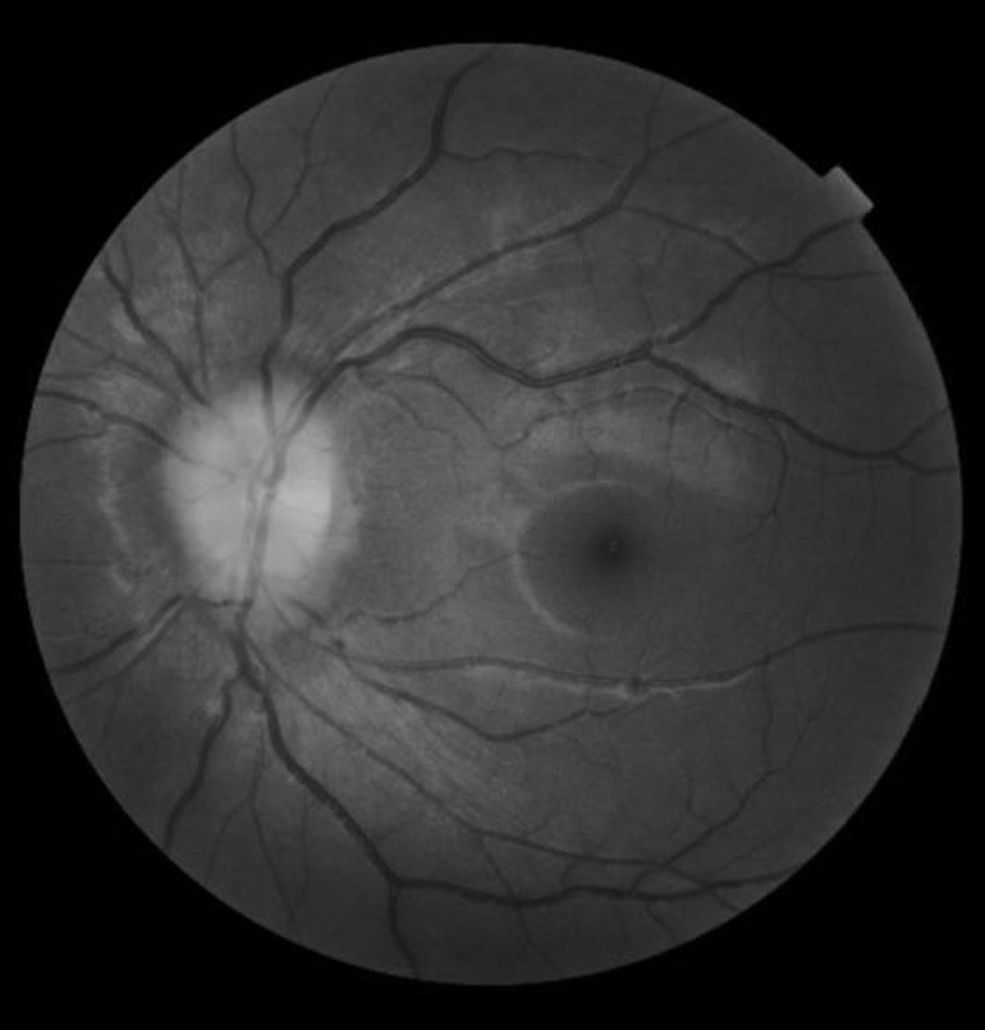
Fundus photograph of the left eye showing grade 3 disk edema, normal macula, and normal vessels.
What is the next best step in her diagnosis and management?
Place referral to weight management clinic.
Reassurance.
Lumbar puncture with opening pressure measurement.
Prescribe sumatriptan and follow-up in 1 month.
Discussion
Epidemiology
Idiopathic intracranial hypertension (IIH), also known as primary pseudotumor cerebri (PTC), is characterized by elevated intracranial pressure (ICP) in the absence of a secondary cause. 1 IIH often occurs in the setting of weight gain. The annual age-adjusted incidence rate is 3.3/100,000 persons in women of ages 15–44 years and 0.3/100,000 in men of the same age group (p < 0.001). 1 Incidence rates increase up to 22/100,000 in obese females of ages 15–44 years. 1 In prepubescent patients there is no association with gender or weight gain. 1
Patients typically present with frequent positional headaches, transient visual obscurations, pulsatile tinnitus, retrobulbar pain, neck and shoulder pain, dizziness, depression, cognitive impairment, and diplopia secondary to cranial nerve 6 palsy. 2 Visual field deficits are usually present and can indicate severity of disease.
There are numerous proposed mechanisms for IIH. Studies evaluating the role of estrogens have been inconclusive. 3 Other proposed mechanisms include impaired cerebrospinal fluid (CSF) reabsorption due to excessive vitamin A-derived proteins and impaired cerebral venous drainage through venous stenosis, microthrombi, increased cardiac filling pressure, and central obesity. 4 Westgate et al. found that women with IIH had higher rates of central truncal obesity and were phenotypically more insulin and leptin resistant. 5
Risk factors
The greatest risk factors for IIH are BMI ≥30 kg/m2 with recent weight gain and female gender of childbearing age. Polycystic ovarian syndrome (PCOS) is associated with IIH. Avisar et al. found that the prevalence of PCOS among patients with IIH to be 15.5%, compared with 8.7% in the general population (p = 0.0001). 6 Secondary PTC can be caused by systemic diseases such as hypothyroidism, severe anemia, Addison disease, systemic lupus erythematosus, end-stage renal disease, pulmonary hypertension, and obstructive sleep apnea. 4 Medications associated with secondary PTC include tetracyclines, second- and third-generation fluoroquinolones, cyclosporine, danazol, vitamin A, lithium, long-term steroid use, growth hormone, nalidixic acid, and others. 4,7
The risk of hormonal birth control, including combination and progestin only medications causing increased ICP, has been controversial for several years. Most case-controlled studies and a recent population-based study found no association between oral contraceptives and increased ICP. However, studies on hormonal contraceptive implants have included a smaller number of patients; a few case reports have suggested an association. Although there is unlikely a connection between IIH and hormonal implants, removal of the implant can be considered, especially if the patient does not respond to weight loss and medical therapy. 3
Diagnostics
The definition of papilledema is optic disk swelling in the setting of elevated ICP. Evaluation of bilateral disk edema needs to be performed in a stepwise approach to localize the lesion to the optic nerve head, the intracranial optic nerve, or the brain. The differential for bilateral disk edema with intact VA and minimal visual field loss is suggestive of increased ICP, vitreopapillary traction, mild-to-moderate diabetic papillopathy, impending central retinal vein occlusion, and hypertensive retinopathy, among other diagnoses. The differential for optic disk swelling with vision loss or visual field loss is vision threatening or severe IIH, anterior ischemic optic neuropathy, optic neuritis, compressive optic neuropathy, and neoplastic optic neuropathy, among others.
Patient evaluation should begin with a thorough history, neurological examination, and complete ophthalmic examination including dilated fundoscopic examination and visual field testing performed by an ophthalmologist. Examination should be followed by neuroimaging, preferably MRI of the brain and orbits with and without contrast and MRV to rule out DVST. If neuroimaging is normal, a lumbar puncture should follow to measure CSF opening pressure and assess for central nervous system (CNS) infection or inflammation.
The modified Dandy criteria for the diagnosis of IIH listed below can be useful in interpreting diagnostic testing and arriving at a final diagnosis. 8 All of the following criteria should be met to diagnose IIH.
Signs and symptoms of increased ICP such as headaches, nausea, vomiting, transient visual changes, pulsatile tinnitus, and papilledema.
No localizing neurological signs except for unilateral or bilateral sixth nerve palsy.
CSF opening pressure >25 cm H2O with normal CSF composition.
No evidence of hydrocephalus, mass, structural, or vascular lesion (including venous thrombosis) on MRI with MRV. Signs of ICP may be seen on imaging such as flattening of posterior pole, empty/partially empty sella turcica due to pituitary gland compression, enhancement of the prelaminar optic nerve, distension of perioptic subarachnoid space, vertical tortuosity of the orbital optic nerve, or stenosis of one or both transverse cerebral venous sinuses.
No other cause of increased ICP identified.
Treatment
The first-line treatment for IIH is weight loss. A 6%–10% reduction in body weight can lead to resolution of disk edema, but additional weight loss may be needed in some patients to reduce headache and ICP. 4 In addition to weight loss management, referral to an ophthalmologist for assessment of VA, visual fields, and optic nerves is required.
First-line medical therapy in patients with mild-to-moderate disk swelling and mild visual loss is acetazolamide. The dose can be advanced up to 4 g/day until symptoms are relieved and optic nerve swelling has resolved. Alternative treatments include topiramate and loop diuretics. Patients with severe disk edema and rapidly progressing vision loss should be emergently evaluated by an ophthalmologist. Brady et al. published an interdisciplinary protocol for management of vision-threatening papilledema patients. 9
These patients require emergent workup to determine the cause of elevated ICP, and they need rapid reduction in ICP by CSF lumbar drain, high dose acetazolamide, and possible optic nerve fenestration or CSF diverting shunt. Given the complex and progressive nature of vision-threatening papilledema, a multidisciplinary approach with ophthalmology, neurology, and neurosurgery has been shown improve patient outcomes and preserve vision. 9
Case Answer
The correct answer is option C. Lumbar puncture showed opening pressure of 29 cm H2O and normal CSF constituents. She meets the diagnostic criteria for IIH. Treatment includes setting weight loss goal, dietician referral, and acetazolamide 500 mg twice a day with 1 month follow-up.
Once a diagnosis of IIH has been made, weight loss is first-line therapy. However, a diagnosis of IIH cannot yet be made based on the information provided in the case. Our patient should also have a lumbar puncture to confirm elevated ICP and to rule out CNS infection and inflammation.
If left untreated, optic disk edema can lead to optic atrophy and possibly permanent vision loss. Patients with optic nerve swelling should be followed regularly by an ophthalmologist and treated appropriately. Patients who have IIH without papilledema do not necessarily need to be followed by an ophthalmologist, as they do not have a threat to their vision or optic nerve health.
Sumatriptan is a treatment for migraine headache. Migraine is unlikely the primary diagnosis in this patient given her disk edema, positional headache, and lack of associated photophobia and nausea. However, over 60% of IIH patients also have migraines. 10 They may need chronic migraine management even after treatment of their elevated ICP. In addition, a diagnosis of increased ICP should be considered in chronic migraine patients who have weight gain, changes in headache characteristics, or if headaches become refractory to migraine therapies.
Footnotes
Authors' Contributions
S.V. contributed to conceptualization, methodology, supervision, project administration, and writing—review and editing; and M.J. was involved in investigation, resources, and writing—original draft.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This study was supported in part by an Unrestricted Grant from Research to Prevent Blindness, Inc., New York, NY, USA, to the Department of Ophthalmology & Visual Sciences, University of Utah.