
Abstract
Objective:
With a global incidence of more than 10%, preterm birth (PTB) remains a significant concern. The vaginal microbiome strongly influences the well-being of the female reproductive tract. This study examines the correlation between changes in Lactobacillus vaginal microbiota and the PTB risk.
Materials and Methods:
A thorough search of PubMed, Web of Science, Cochrane Library, and EMBASE was conducted to locate studies that examined the association between changes in Lactobacillus vaginal microbiota and the risk of PTB from January 1, 2010, to January 30, 2023. The risk of PTB was determined by calculating odds ratios (ORs) with 95% confidence intervals (CIs).
Results:
In our analysis, there were 11 studies with 1577 pregnant women. The findings revealed a significant negative correlation between higher Lactobacillus abundance and the PTB risk (OR = 0.49, 95% CI: 0.29–0.84, p = 0.009 < 0.05). Similarly, the four individual dominant species, Lactobacillus crispatus (OR = 0.3, 95% CI: 0.14–0.67, p = 0.003 < 0.05), Lactobacillus gasseri (OR = 0.34, 95% CI: 0.17–0.69, p = 0.003 < 0.05), Lactobacillus iners (OR = 0.68, 95% CI: 0.49–0.93, p = 0.016 < 0.05), and Lactobacillus jensenii (OR = 0.43, 95% CI: 0.21–0.89, p = 0.024 < 0.05), were also negatively associated with the PTB risk. The risk of Lactobacillus for PTB was significant in both America (OR = 0.67; 95% CI: 0.50–0.92) and Asia (OR = 0.20; 95% CI: 0.09–0.47), whereas no significant risk was found in Europe (OR = 0.49; 95% CI: 0.11–2.15).
Conclusions:
Our study demonstrated that the abundance of Lactobacillus and the four dominant individual species (L. crispatus, L. jensenii, L. iners, and L. gasseri) were significantly and negatively associated with the PTB risk.
Introduction
The medical field of obstetrics is facing a persistent challenge in addressing preterm birth (PTB), a condition characterized by the delivery of a baby before completing 37 weeks of gestation. It is a significant problem, as it is the primary cause of perinatal incidence rate and mortality, and among children younger than 5 years, it is the direct cause of death that is second in frequency. 1,2 Global PTB rates were estimated at 10.6% in 2014 in 107 countries. 3 Sterile inflammation, infection, and uterine distension are possible causes of spontaneous PTB.
In addition, PTB may be necessary for medical reasons due to fetal distress, preeclampsia, or other causes. 4 Currently, the most accurate way to predict PTB is by examining a woman's history of premature delivery during a previous pregnancy. Other significant risk factors linked to a higher risk of PTB include having a mid-trimester cervical length of 25 mm or less, having low or high maternal weight, being Black, and smoking. 5,6 The incidence of PTB has been linked to differences in the composition of the vaginal microbiome across various populations. 7,8
The creation of lactic acid by bacteria in the human vagina is believed to play a vital role in safeguarding the host from infectious diseases by regulating the growth of harmful pathogens and other opportunistic organisms through pH control. 9,10 Among the bacterial communities in the vagina, Lactobacillus species produce antimicrobial substances known as bacteriocins. The bactericidal properties of these protein substances can prevent the growth of vaginal Lactobacillus gasseri, Gardnerella vaginalis ATCC 14018, Lactobacillus acidophilus, and Pseudomonas aeruginosa ATCC 10145. 11 While bacterial populations in the vagina can differ, lactic acid bacteria are typically the most dominant. 7 Therefore, maintaining a high ratio of lactic acid bacteria is considered an indicator of good health.
Changes in the microbiota during pregnancy may indicate the likelihood of PTB. Stout et al. 12 discovered that women who gave birth prematurely experienced a significant reduction in the diversity, richness, and evenness of their vaginal microbiome between the first and second trimesters, as opposed to those who delivered their babies full-term. However, the vaginal microbiome was not significantly different between women who had preterm deliveries and those who delivered full-term during the third trimester. 12 Fettweis et al. 9 found that bacterial vaginosis-associated taxa declined among women with preterm deliveries, wheras Lactobacillus crispatus increased during pregnancy. In addition, Fettweis et al. observed that alterations in the vaginal microbiome during pregnancy were impacted by race, with Caucasian women having more consistent microbiomes compared with other ethnicities.
However, previous studies have indicated that among Caucasian women who gave birth preterm, there was an increase in G. vaginalis. 9 Based on the current evidence, alterations in the vaginal microbiome specific to gestational age may indicate the likelihood of term delivery. It remains uncertain whether these changes are risk factors for PTB.
Conflicting results have emerged from studies exploring the vaginal microbiome and PTB connection. No correlation was found between PTB risk and diverse vaginal communities in a study involving primarily Asian and White women with a history of spontaneous PTB. However, the study did identify that a decreased abundance of L. crispatus and an increased abundance of Lactobacillus iners were associated with higher subsequent PTB risk. 13 Another study, which utilized an improved bioinformatics approach, demonstrated no relationship between L. iners and birth results in White or African American (AA) cohorts. Despite this, the research revealed that L. crispatus had a protective impact on both cohorts and a connection was observed between lower levels of Lactobacillus jensenii and L. gasseri and PTB in the AA cohort. 7 This study aimed to perform a systematic review and meta-analysis to evaluate the statistical relationship between alterations in Lactobacillus vaginal microbiota and the probability of PTB.
Materials and Methods
Literature search
The study aimed to systematically examine the link between variations in Lactobacillus vaginal microbiota and the possibility of giving birth preterm through an extensive literature search. The databases PubMed, Cochrane Controlled Register of Trials (CENTAL), EMBASE, and Web of Science were used to perform the search. To enhance the quality of reporting, the systematic review and meta-analysis adhered to the PRISMA checklist. 14 The search included articles released between January 1, 2010, and January 30, 2023, without any language or release status restrictions. Refer to Supplementary Table S1 for the comprehensive search approach.
Inclusion criteria
The following criteria determined inclusion of studies: (1) A clear evaluation of the Lactobacillus vaginal microbiota before the commencement of labor, covering complications such as premature rupture of membranes and other issues associated with labor; (2) Until delivery, all participants were tracked; (3) Studies that reported changes in Lactobacillus vaginal microbiota and their relationship to the risk of PTB were deemed eligible; (4) To avoid culturing, 16S analysis was used to identify species from samples. Studies published since 2010 were the only ones included, as this was when 16S sequencing techniques became available; (5) There were no limitations imposed on the age of the participants, study environment, or language used.
Exclusion criteria
The exclusion criteria were as follows: (1) Only studies involving high-risk pregnancies, such as prior PTB or cervical weakness, were excluded; (2) Excluded from the analysis were studies that involved interventions, cross-sectional studies that collected samples after labor onset, and studies that focused exclusively on specific pathogens or used culture-dependent or microscopic diagnostic methods; (3) Studies that were excluded also included reviews, book chapters, editorial letters, books, conference abstracts, case reports, and commentaries; (4) Studies with the same cohort or overlapping cohorts were either merged into a single study or the most recent study was included.
Data extraction
Two independent reviewers performed data extraction, and a third reviewer verified the data for accuracy. Any discrepancies were resolved through group consensus. The extracted information included the first author's last name, publication year, region, ethnicity, mean age, study design, sequencing methods, hypervariable region, and sample size. Patients were defined as having high Lactobacillus abundance if the vaginal community status was dominated by L. crispatus, L. gasseri, L. iners, L. jensenii, or other lactobacilli via 16S rRNA sequencing. Otherwise, cases were regarded as low Lactobacillus abundance.
Quality assessment
Using the Newcastle–Ottawa Assessment Scale, 15 the quality of cohort studies or nonrandomized case–control studies was evaluated, and each study was rated in three primary domains: selection, comparability, and outcome.
Data analysis and meta-synthesis
Data analysis was conducted using STATA software (version 14.0; Stata Corp, College Station, TX). For dichotomous outcomes, the odds ratio (OR) with 95% confidence intervals (CIs) was calculated based on the combined number of outcomes. The I 2 statistic and p-value were used to assess statistical heterogeneity. Heterogeneity was considered unimportant if I 2 was between 0% and 40%, moderate if I 2 was between 30% and 60%, substantial if I 2 was between 50% and 90%, and considerable if I 2 was between 75% and 100%. If I 2 was ≤50% or the p-value was >0.1, the study was classified as mildly statistically heterogeneous, and a fixed-effect model was used. Otherwise, a random-effects model was used to pool the effect size.
A sensitivity analysis, specifically the leave-one-out approach, was conducted to determine the impact of each study on the overall effect estimate. Results that were susceptible to significant changes after removing studies were considered to be less robust. When more than 10 articles were included, publication bias in the meta-analysis was assessed using funnel plots, Egger's regression test, and Begg's rank correlation test. 16 Nonparametric trim-and-fill analysis was performed in case of evidence of publication bias. 17
Results
Study selection
Figure 1 presents the PRISMA diagram outlining the database search process and final selection of articles. A total of 7539 records were identified, with 4561 unique records among them. Seventy records were initially considered relevant based on the title and abstract screening. After a thorough analysis, a final selection of 11 studies 9,18 –27 meeting all relevant criteria were used for the meta-analysis, including 5 case–control studies and 6 cohort studies.
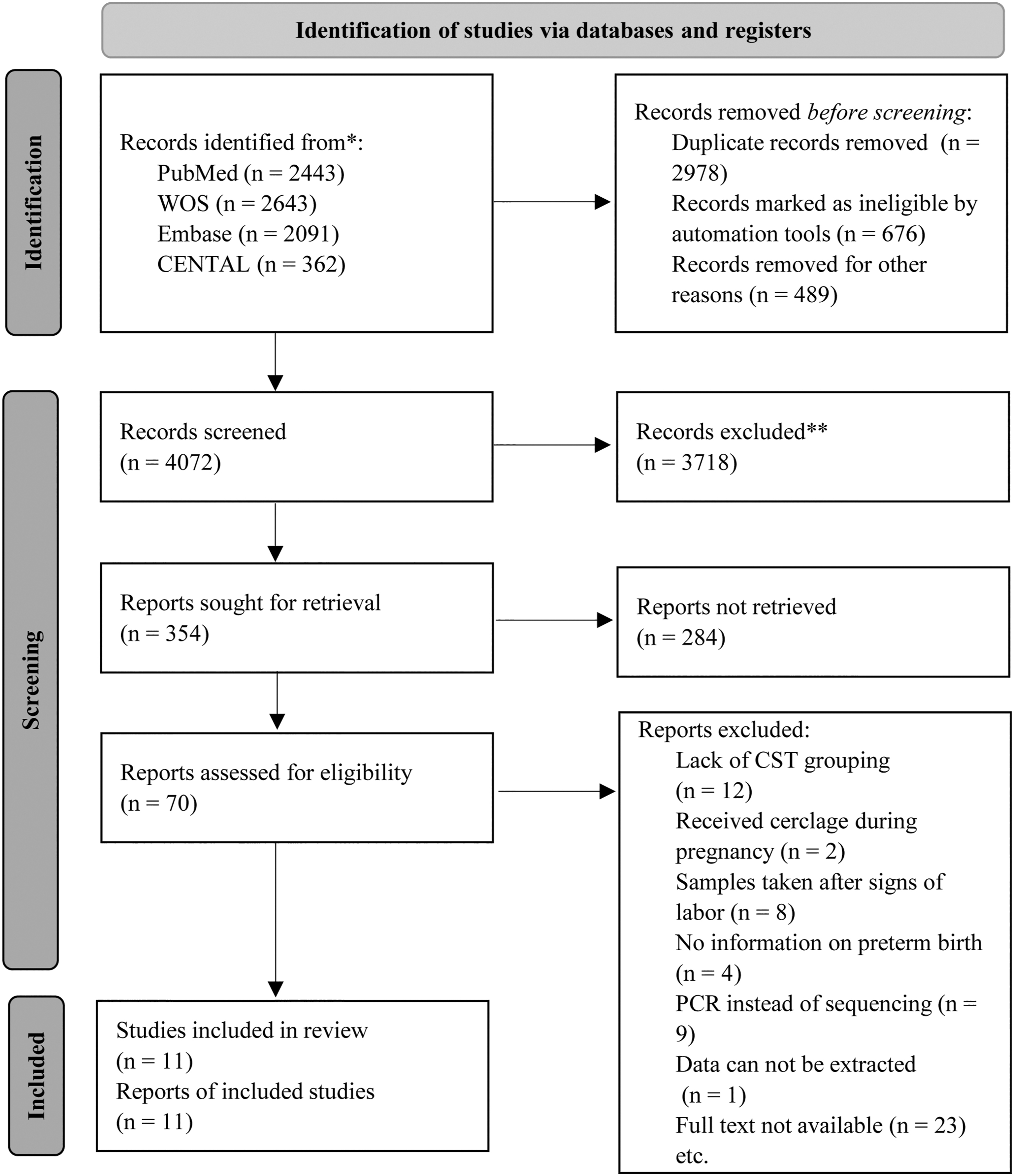
Flow diagram of the study selection process.
Characteristics of the included studies
Table 1 provides specific information regarding the included articles published between 2014 and 2022. The studies were conducted in various countries, including the United States, Korea, the United Kingdom, Canada, Pakistan, Nigeria, and Brazil. The sample sizes of the included articles ranged from 38 to 449, with a total of 1577 participants, consisting of 1212 term births and 365 PTB. The average Newcastle-Ottawa Scale score for the included studies was 7.4 points, with all selected studies receiving a score between 6 and 8 points, indicating a relatively high level of quality (Table 2).
Characteristics of the Studies Included in This Meta-Analysis
NA, not available.
Quality Assessment of the Included Studies by Newcastle-Ottawa Scale
NOS assesses studies on 3 dimensions with a maximum score of 9 and each star representing one point. The quality of each study was assessed using the following scoring algorithm: ≥ 7 as “good,” 2–6 as “fair,” and ≤ 1 as “poor.”
There were up to 4 stars for quality in representing patient selection, up to 2 stars for comparability between cases and controls, and up to 3 stars for adequately determining exposure.
NOS, Newcastle-Ottawa Scale.
Meta-analysis results
Vaginal microbiota and the risk of PTB
A total of 11 studies were included in the meta-analysis of the relationship between Lactobacillus abundance and the risk of PTB. The clinical heterogeneity test showed moderate heterogeneity among the studies (I 2 = 58.6%, p = 0.007). Therefore, a random-effects model was used to combine the effect sizes. The results showed a statistically significant negative correlation between higher Lactobacillus abundance and the risk of PTB (p = 0.009 < 0.05), with an OR of 0.49 and a 95% CI of [0.29–0.84], as shown in Figure 2.
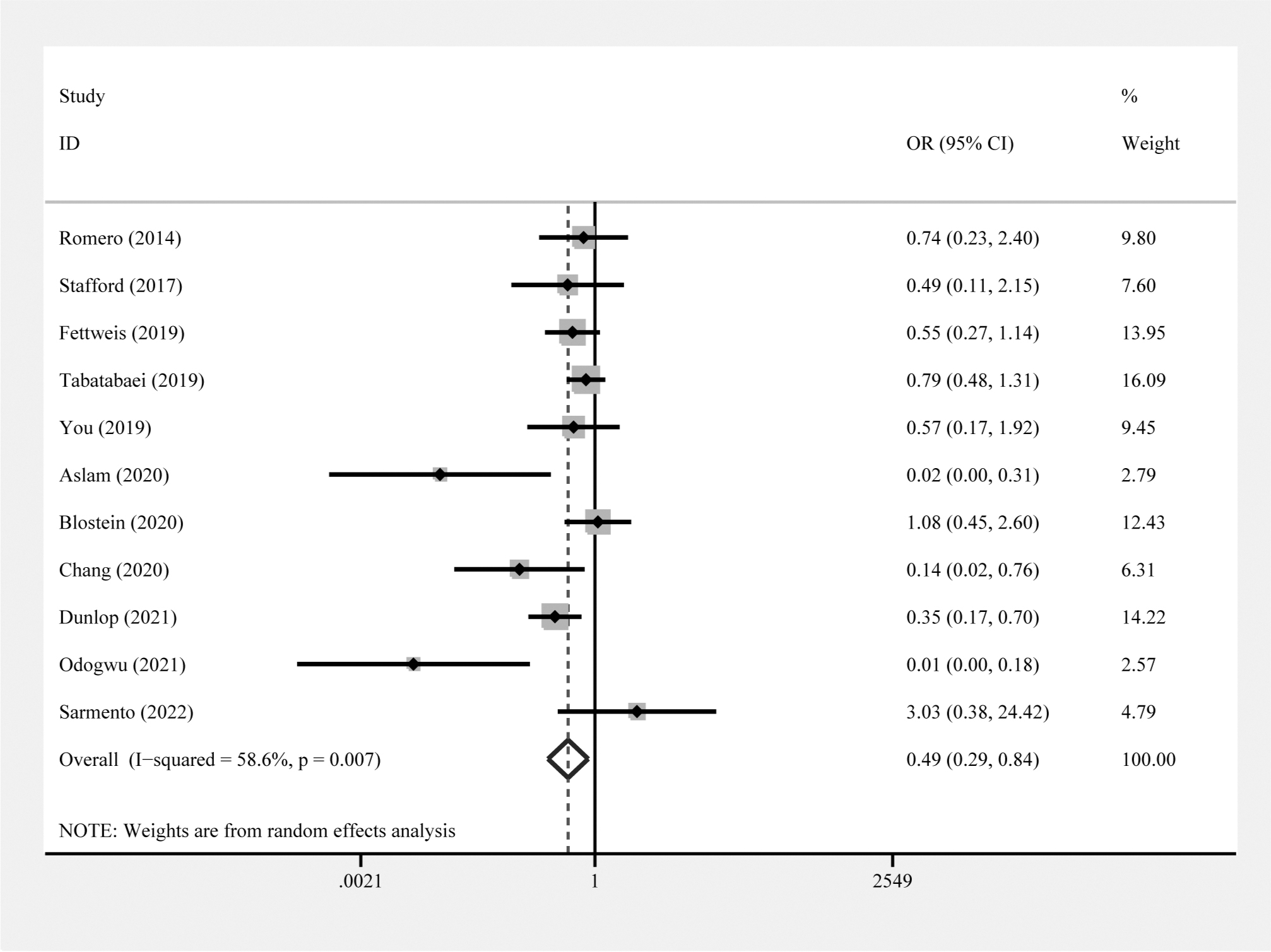
Forest plots of the risk of higher Lactobacillus abundance for preterm birth.
L. crispatus and the risk of PTB
A total of 10 studies reported the relationship between L. crispatus abundance and PTB risk, with moderate heterogeneity among the studies (I 2 = 54.2%, p = 0.02). The random-effects model was used, and the results showed a statistically significant negative correlation (p = 0.003 < 0.05), with an OR of 0.3 and a 95% CI of [0.14–0.67], as shown in Figure 3A.
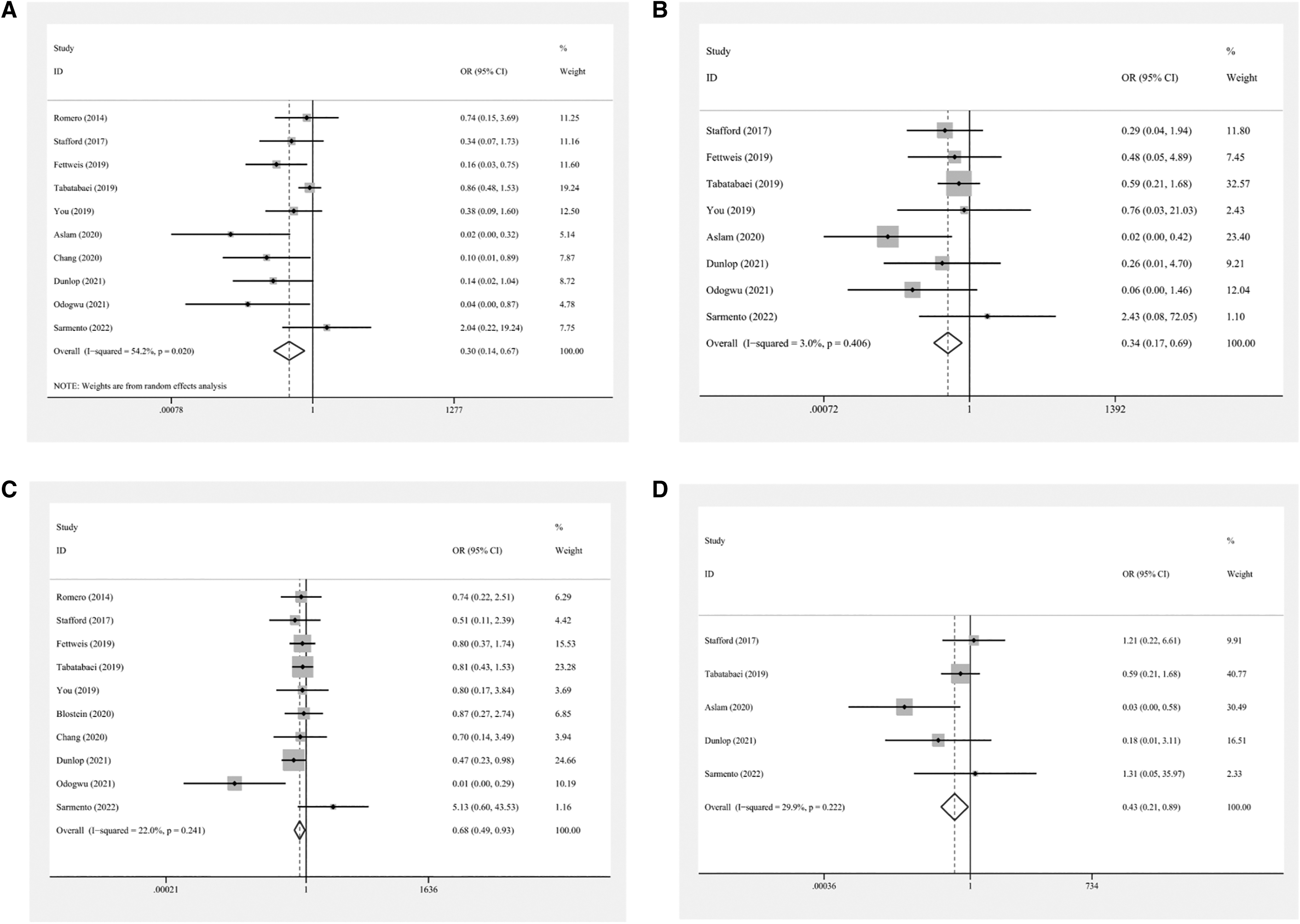
Subanalysis of the risk of Lactobacillus crispatus
L. gasseri and the risk of PTB
Eight studies reported the relationship between L. gasseri abundance and PTB risk, with no significant heterogeneity among the studies (I 2 = 3%, p = 0.406). Therefore, a fixed-effects model was used, and the results showed a statistically significant negative correlation (p = 0.003 < 0.05), with an OR of 0.34 and a 95% CI of [0.17–0.69], as shown in Figure 3B.
L. iners and the risk of PTB
Ten studies reported the relationship between L. iners abundance and PTB risk, with unimportant heterogeneity among the studies (I 2 = 22%, p = 0.241). A fixed-effects model was used, and the results showed a statistically significant negative correlation (p = 0.016 < 0.05), with an OR of 0.68 and a 95% CI of [0.49–0.93], as shown in Figure 3C. In addition, the risk of L. iners for PTB was significant among AA (OR = 0.47; 95% CI: 0.23–0.98), whereas no significant risk was found among Asians (OR = 0.75; 95% CI: 0.24–2.29) (Fig. 4A).

Sensitivity analysis in the risk of Lactobacillus
L. jensenii and the risk of PTB
Five studies reported the relationship between L. jensenii abundance and PTB risk, with unimportant heterogeneity among the studies (I 2 = 29.9%, p = 0.222). A fixed-effects model was used, and the results showed a statistically significant negative correlation (p = 0.024 < 0.05), with an OR of 0.43 and a 95% CI of [0.21–0.89], as shown in Figure 3D.
Geographic location
The risk of Lactobacillus for PTB was significant in both America (OR = 0.67; 95% CI: 0.50–0.92) and Asia (OR = 0.20; 95% CI: 0.09–0.47), whereas no significant risk was found in Europe (OR = 0.49; 95% CI: 0.11–2.15) (Fig. 4B).
Sensitivity analysis
The sensitivity analysis found that the overall estimate was not dependent on a single study (Fig. 5).

Sub-analysis of the risk of L. iners for preterm birth among African American and European
Publication bias
All the studies included in the analysis were assessed for publication bias using Begg's rank correlation and Egger's weighted regression tests. The results of Begg's and Egger's tests did not show any publication bias for Lactobacillus (Begg's p = 0.119, Egger's p = 0.106) (Fig. 6A) and L. iners (Begg's p = 0.474, Egger's p = 0.657) (Fig. 6B). However, publication bias was found for L. crispatus based on Begg's and Egger's regression tests (Begg's p = 0.074, Egger's p = 0.013) (Fig. 6C). Therefore, trim-and-fill analysis was performed for L. crispatus, but it was found that there was no need for additional literature (Fig. 6D).
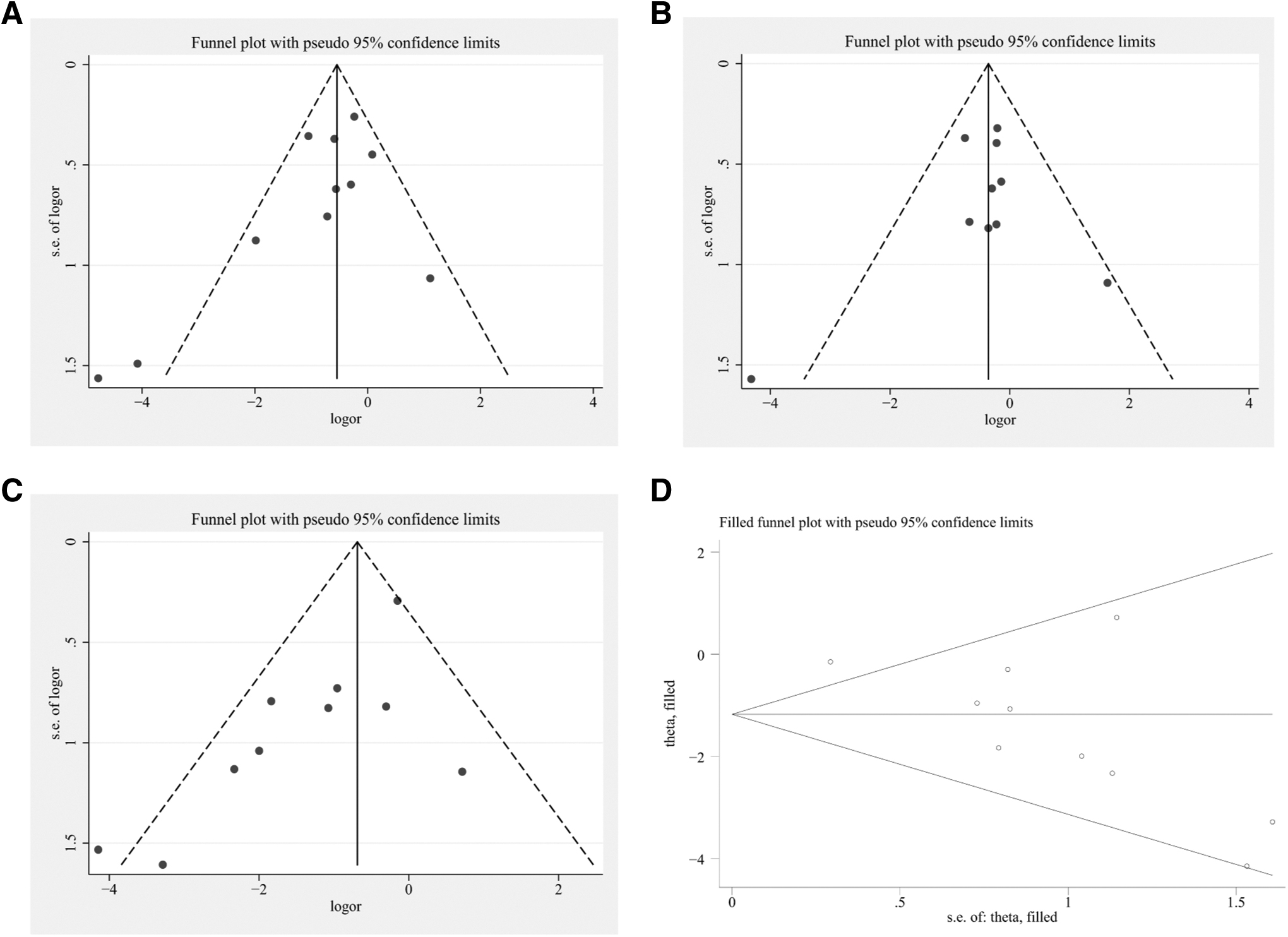
Funnel plot in the risk of Lactobacillus
Discussion
The health of the female reproductive tract is heavily influenced by the composition of the vaginal microbiome, with a microbiome dominated by Lactobacillus species playing a crucial role in maintaining a healthy state. This is due to the production of lactic acid, which lowers the vaginal pH. On the contrary, an increase in bacterial diversity, particularly non-Lactobacillus species, as seen in bacterial vaginosis, is considered an independent risk factor for sexually transmitted infections, pelvic inflammatory disease, and PTB. 28,29 However, the vaginal microbiome contains a variety of Lactobacillus species, which can produce varying levels of lactic acid and exhibit differing levels of tolerance toward anaerobic microbial species. 30
There is disagreement regarding the link between the maternal vaginal microbiome and the risk of PTB. A case–control study conducted in the United States showed that patients with low levels of Lactobacillus in their community state type (CST) but high levels of Gardnerella or Ureaplasma were at a higher risk of PTB. 31 On the contrary, a U.S. cohort study found no correlation between low levels of Lactobacillus and the risk of PTB. 32 In the United Kingdom, a study revealed that a dominance of L. crispatus in the vaginal microbiota at 16 weeks of gestation could protect against PTB before 34 weeks, whereas L. iners is a risk factor for PTB in women at high risk. 13 The above evidence highlights the importance of identifying Lactobacillus at the species level. Although two related meta-analyses 33,34 have been published, the relationship between specific Lactobacillus species and the risk of PTB has not been conclusively established.
Our findings indicated that the presence of Lactobacillus, along with its four individual dominant species (L. crispatus, L. gasseri, L. iners, and L. jensenii), was negatively correlated with the risk of premature delivery. Among these Lactobacillus species, L. iners and L. gasseri have more distinctable characteristics. 35 L. iners, in comparison to other Lactobacillus species, may potentially represent a stronger root origin and present in human vaginal microbiomes at an earlier stage. 10 Striker divergence is also higher in L. gasseri instead of various Lactobacillus species; however, significant divisions between subgroups might be the reason, and this may have originated before the establishment of the human vaginal microbiome. 35
L. jensenii exhibits low diversity and a notebly positive Tajima's D, which is suggestive of the presence of an excess of medium frequency alleles, and this may be an indication of a bottleneck or balancing selection, and it is possible to have a relation with the colonization of the vaginal niche. 35 L. iners are more prevalent among African women, whereas an abundance of L. crispatus is commonly observed among European women. 10,36,37 Future work should focus more on what kind of ecological factors affect the intra-community and inter-community variations, especially at the strain level. The reason for the existing population structure caused by the evolution of genomic and the functional differentiation also requires more research to fill the gap.
The study involving diverse ethnicities, such as AA, European, and Asian. Studies have highlighted that according to the self-reported ancestry, different population have different predominant taxa. 10,36,37 For instance, L. crispatus is more commonly found in European women, whereas L. iners prevalence is higher in African women. 10,36 Studies have found that European women had lower incidence of adverse reproductive disorders because of the heritability of L. crispatus. 38 Our subanalysis results further indicated that L. iners was more likely to reduce the risk of PTB among AA than Asians.
This study provides additional evidence that the composition of the vaginal microbiome tends to be associated with the risk of PTB. Our findings are consistent with previous studies 33,34 showing that changes in the vaginal microbiome during pregnancy may indicate the likelihood of PTB. Specifically, our study suggests that maintaining a high proportion of lactic acid bacteria, particularly the four dominant individual species, is a sign of good health and may protect against PTB. The findings of this meta-analysis have significant clinical implications. Understanding the role of the vaginal microbiota in pregnancy and its association with PTB could lead to developing interventions to lower the risk of PTB by maintaining a healthy vaginal microbiome. For instance, probiotics that contain Lactobacillus species could be used to prevent PTB in high-risk women. However, more studies are needed to determine the optimal intervention strategies to improve vaginal health during pregnancy and prevent PTB.
The microbial composition of the vagina may offer valuable information for the precise and prompt diagnosis or prediction of pregnancy-related conditions. In clinical settings, assessing the risk of PTB could be aided by the vaginal microbiota's ability to predict preterm delivery outcomes early and with high precision, according to Haque et al. 39 Despite recent progress, conflicting information and limited understanding of the connection between the vaginal microbiota and high-risk pregnancy persist. In the study by Hyman et al., 32 PTB was associated with increased diversity within the vaginal microbial community.
DiGiulio et al. reported an inverse correlation between gestational age at delivery and the prevalence of a Lactobacillus-poor vaginal CST IV. 31 On the contrary, the relative abundance of microbial phylotypes or any specific CST did not show a significant correlation with PTB, as reported by Romero et al. 18 Furthermore, the vaginal microbiota may vary based on ethnicity and race, as suggested by several reports, 7,40 underscoring the importance of individual studies to assess the vaginal microbiota properly across diverse ethnic groups. In this study, we observed that not only the abundance of Lactobacillus but also the four individual dominant species (L. crispatus, L. iners, L. gasseri, and L. jensenii) were negatively correlated with the risk of PTB.
Our study has several strengths. First, it included a large sample size of 1577 pregnant women, which provides more statistical power and generalizability. Second, we thoroughly searched multiple databases to identify all relevant studies. Third, we used a meta-analysis to combine the results of multiple studies, increasing our estimates' precision. Some limitations need to be acknowledged in this meta-analysis. Although all the studies included in this analysis were of high quality, significant heterogeneity was observed. The first limitation is that all the studies were observational, which makes it difficult to avoid selection and observer bias.
In addition, publication bias was detected in some indexes, although it did not alter the result. Second, only relevant studies in English were included, which means that some relevant published data may have been missed. Third, it is well-known that microbiome studies are influenced by various factors, such as extraction methods, sample collection, and the hypervariable region utilized during sequencing. Any differences in these factors could impact the outcomes.
Conclusions
In summary, this meta-analysis demonstrated that not only the abundance of Lactobacillus but also the four dominant individual species (L. crispatus, L. gasseri, L. iners, and L. jensenii) were negatively associated with the risk of PTB. However, the current evidence was derived from observational studies, and it is suggested that high-quality studies with larger sample sizes be conducted for validation.
Footnotes
Authors' Contributions
Conception and design: J.L. and J.G. Administrative support: J.L. and J.G. Provision of study materials or patients: J.L. and J.G. Collection and assembly of data: Q.Z., Y.Y., and J.Z. Data analysis and interpretation: Q.Z., Y.Y., and J.Z. Article writing: All authors. Final approval of the article: All authors.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This study was supported by the National High Level Hospital Clinical Research Funding (2022-PUMCH-A-233).
Supplementary Material
PRISMA_2020_checklist
Supplementary Table S1
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.