
Abstract
Objective:
To examine how (1) partnered sexual activity, and (2) sexual functioning, contribute to global quality of life (QOL) and health-related quality of life (HRQL) among midlife and older women, and whether importance of sex modifies these associations.
Materials and Methods:
Women in the Study of Women's Health Across the Nation (SWAN), a multiethnic/racial cohort study, aged 42–52 at recruitment, were followed for ∼20 years. The Ladder of Life and Short Form-36 physical component summary (PCS) and mental component summary (MCS) assessed Global QOL (N = 3,263) and HRQL (N = 2,576), respectively. Primary predictors were (1) having partnered sexual activity (yes/no), and (2) sexual functioning among those with partnered sexual activity. Sociodemographic, health, lifestyle, and psychosocial covariates were included.
Results:
Importance of sex modified covariate-adjusted association of having partnered sexual activity with global QOL. Adjusted associations of partnered sexual activity with PCS and MCS were not statistically significant. Sexual functioning, among women with partnered sexual activity, was positively associated with global QOL (adjusted p = 0.03), regardless of importance of sex; unrelated to PCS; but positively associated with MCS (adjusted p = 0.03), particularly when sex was “very/quite important.”
Conclusions:
Partnered sexual activity and better sexual functioning are related to QOL for mid-aged and older women, and are stronger when sex is considered important. Partnered sexual activity and sexual functioning are less consistently related to HRQL when adjusted for covariates, and importance modifies only the association between sexual functioning and MCS. Understanding the importance of sex to midlife and older women contextualizes the impact of sex on QOL.
Introduction
Sexual activity and functioning in women is generally considered important to quality of life (QOL). 1,2 Sexual activity includes being sexually engaged with a partner or participation in types of sexual behaviors, while sexual functioning includes multiple domains such as desire, arousal, satisfaction, and presence/absence of sexual pain. 3,4 Given the physiologic and psychosocial changes that occur across the menopausal transition, sexual function among midlife women has received a good deal of attention. 3,5 –9
Despite considerable literature on factors related to QOL, 10 –14 empirical evidence for a role of sexual activity and functioning in overall QOL is sparse. Furthermore, many factors related to global QOL and health-related quality of life (HRQL) are also related to sexual functioning, including age, education, health status, lifestyle factors, psychological function, and relationship quality. 4,9,11 –13,15 –17 It is thus important to adjust for these covariates when evaluating the impact of sexual function on QOL/HRQL.
Several large cross-sectional surveys have examined sexual dysfunction and QOL-related outcomes, including overall QOL 18,19 and HRQL. 20,21 A large study of sexual behavior of men and women in the United States reported that sexual dysfunction (defined as low desire, arousal disorder, and sexual pain) was highly associated with low feelings of happiness, even adjusting for age, marital status, education, race and ethnicity, religion, and place of residence. 18 A Danish study found that women reporting sexual problems had lower QOL, but analyses did not adjust for confounders. 19
Two cross-sectional studies of hypoactive sexual desire disorder (HSDD; i.e., being distressed by low sexual desire) and HRQL in women found that HSDD was related to lower scores on the Short Form-12 (SF-12) 20 and lower scores on several domains of the SF-12 and the EuroQol-5D (EQ-5D). 21 After controlling for depressive symptoms, body mass index (BMI), smoking, and comorbidities, HSDD was no longer significantly related to SF-12 domains, but remained significantly related to the EQ-5D. 21
Given that both sexual functioning and the degree to which sex is important decline with age, 6,15,18,22 –24 the role of sexual functioning in QOL/HRQL should be considered within the context of the importance of sex. In addition, most research examines sexual function and dysfunction in people who are sexually active with partners. However, being sexually active in itself may be relevant to QOL, especially if sex is considered important. We could not identify any studies that examined whether just being sexually active with a partner (compared to being inactive) regardless of level of function was related to QOL or HRQL.
The primary objective of these analyses was to examine the roles of: (1) having partnered sexual activity, and (2) sexual functioning (defined as sexual desire, arousal, ability to climax, pain with intercourse, and emotional satisfaction) among those with partnered sexual activity in women's QOL/HRQL, adjusting for related variables, and to consider how the importance of sex modifies these associations. We hypothesized: (1) partnered sexual activity and higher sexual functioning would be related to better QOL/HRQL in multivariable models adjusting for relevant covariates; and (2) importance of sex would moderate relationships of partnered sexual activity and sexual functioning with QOL/HRQL.
Materials and Methods
Sample and procedures
The Study of Women's Health Across the Nation (SWAN) is a multiracial/ethnic cohort study characterizing biological and psychosocial changes occurring during the menopausal transition 25 and beyond. From 1995 to 1997, seven clinical sites recruited from the community non-Hispanic White women and women belonging to a predetermined racial/ethnic minority (Black women in Pittsburgh, Boston, Michigan, Chicago; Japanese women in Los Angeles; Hispanic women in Newark; Chinese women in Oakland, California). The protocol was approved by Institutional Review Boards at each site. All participants provided written informed consent.
A brief 15-minute telephone or in-home screening interview was conducted to determine eligibility for SWAN's longitudinal cohort. Baseline eligibility included age 42–52 years; an intact uterus and at least one ovary; not pregnant, lactating, using oral contraceptives, or hormone therapy (HT); and having a menstrual cycle in the prior 3 months. Among cohort-eligible women, 50.7% (N = 3,302) entered the longitudinal study. 25 Participants were assessed in-person at baseline and approximately annually through follow-up visit 15 from 1997 to 2017 using a standardized protocol assessing medical, reproductive, and menstrual history; lifestyle and psychosocial factors; physical and psychological symptoms; and anthropometric measurements. All instruments were provided in English, Spanish, Japanese, and Cantonese.
Measures
Outcomes
Global QOL
Global QOL was measured at screening and all follow-up visits using the Ladder of Life developed by Cantril 26 and modified by Andrews and Withey, 27 a widely used scale with variations. 28 –32 Respondents were asked: “Think about the quality of your life at the present time. I'd like you to give it a rating where 0 represents the worst possible quality for you and 10 represents the best possible quality for you.” The scale is self-anchoring because ratings are made relative to each person's conception of her own maximum and minimum QOL. Based on previous analyses, 11 original responses were recoded as 0–4 (poor), 5–7 moderate, 8 (good), and 9–10 (excellent); current analyses collapsed poor and moderate to avoid small cell counts.
Health related quality of life
We used the SF-36 to assess HRQL with the original coding algorithm where raw scores are transformed to a 0–100 range. 33 The SF-36 is a generic HRQL measure yielding eight subscales and two summary scores: the physical component summary (PCS) and the mental component summary (MCS). 34 The PCS includes domains of physical functioning, role limitations caused by physical health problems, bodily pain, and general health perceptions. The MCS includes domains of vitality, social functioning, role limitations due to emotional problems, and mental health. Because the SF-36 was not administered until visit 06, the sample for these analyses is smaller than that for global QOL. The SF-36 was subsequently administered at visits 08, 10, 12, 13, and 15.
Sexual activity/functioning predictors
SWAN measured sexual activity and functioning at each study visit from baseline to visit 6 and subsequently at follow-up visits 08, 10, 12, 13, and 15. Women with and without sexual partners completed a 20-item, self-administered questionnaire (returned to staff in a sealed envelope), inquiring about sexual activity and function during the prior 6 months. The questionnaire was derived from several sources 5,35,36 and designed to cover important domains of sexual functioning. We analyzed (1) partnered sexual activity, and (2) sexual function among those with partnered sexual activity.
Partnered sexual activity (asked of all). Women were classified as having partnered sexual activity if they responded “yes” to: “During the past 6 months, have you engaged in sexual activities with a partner?” where “sexual activities” was not specified.
Sexual Functioning Score. A sexual functioning score that was based on the Female Sexual Functioning Index (FSFI) 37 was subsequently developed from the SWAN items. The sexual functioning score is highly correlated with the total FSFI score (rho = 0.84) and its development is described in detail. 6 The sexual functioning score consists of 5 items measuring important domains of sexual function: sexual desire, emotional satisfaction, ability to climax, arousal, and pain. Scores range from 5 to 25 with higher scores indicating better functioning. The sexual functioning score was calculated only at visits where women responded “yes” to having sexual activities with a partner.
Effect modifier
Importance of Sex (asked of all) was considered a modifying variable, as we hypothesized that the associations of global QOL and HRQL with partnered sexual activity and with sexual functioning would differ by concurrent importance of sex. This was a single 5-point item asking how important sex was to a woman. Responses included: not at all important, not very important, moderately important, very important, and quite important; the latter two categories were combined in analyses to avoid small cell counts.
Covariates
Covariates for each outcome were based on variables previously found related to QOL 11 or HRQL. 12,13 Sociodemographic variables included age, marital status (married or living as married, separated/divorced, widowed, never married), race/ethnicity, educational attainment (<high school, high school, some college, college, more than college), and difficulty paying for basics (very hard to pay for basics, somewhat hard, not at all hard). Race and ethnicity were self-defined in response to the open-ended question: “How would you describe your primary racial or ethnic group?” Responses were categorized as White (non-Hispanic), Black, Chinese, Hispanic, or Japanese.
Health-related variables included self-assessed health (excellent, very good, good, fair/poor); number of medical conditions (none, 1, 2, or more). Menopause status was categorized as premenopausal (bleeding in the previous 3 months with no change in menstrual regularity in the past year), early perimenopausal (bleeding in the previous 3 months and changes in menstrual regularity in the past year), late perimenopausal (amenorrhea in previous 3 months but bleeding in past year), nonsurgically postmenopausal (>12 months of amenorrhea), bilateral oophorectomy, unknown due to hysterectomy, or unknown due to premenopausal HT use. Symptoms included sleep problems (any of the following: difficulty falling asleep, staying asleep, and/or early morning awakening ≥3–4 times/week in past 2 weeks) and frequency of vaginal dryness (past 2 weeks: none, 1–5 days, 6–14 days) and urinary leakage (never, <1 day/week in past month, 1+days/week in past month).
Lifestyle and anthropometric variables included cigarette smoking (never, past, current), physical activity, 38,39 and BMI (weight [kg]/height [m2]). Psychosocial factors included perceived stress (summed score of 4 items, total score ranging from 5 [never] to 25 [fairly often]), 40 stressful life events (none, 1, 2, or more), attitudes toward aging and menopause, 41 trait anxiety, emotional and instrumental social support (4-item summed scale), 42 and depressive symptoms (score ≥16 on Center for Epidemiologic Studies Depression [CES-D] scale). 43
Race/ethnicity, education, and site were time invariant. All other variables were time varying starting at baseline (screening) for global QOL and visit 06 for HRQL. Missing time-varying covariates were interpolated based on prior/subsequent visits for categorical covariates and random effects modeling for continuous covariates. 44
Statistical analyses
Separately for global QOL and SF-36 outcomes, we summarized participant characteristics at the first visit included in analyses using frequencies and percentages for categorical variables and means and standard deviations for continuous variables. To address the first objective of being sexually active with a partner, we compared global QOL by partnered sexual activity status using random effects ordinal logistic regression 45 before and after adjusting for covariates, first in the full sample and then including effect modification by importance of sex. Parallel analyses were conducted for the continuous PCS and MCS outcomes (HRQL) versus partnered sexual activity status using linear mixed models. 44 The second objective on sexual functioning (among those having partnered sexual activity), analyses were run including only observations with partnered sexual activity and substituting continuous sexual functioning score for partnered sexual activity as the primary predictor of global QOL and HRQL. Sensitivity analyses omitted visits baseline through 05 in analyses of global QOL to correspond with the timeframe used for the HRQL analyses (data not shown).
Results
Of 3,302 women enrolled in SWAN, the number of women in each of our four analytic samples was different due to our two predictors and the timing of our two outcomes (Supplementary Figs. S1 and S2). Because the global QOL measure was initiated earlier in SWAN, the participants in the two global QOL analyses were younger, at an earlier menopause stage, and had less difficulty paying for basics (Table 1) compared to the participants in the two HRQL analyses. For both global QOL and HRQL, that is, in all four analytic samples, almost half of the participants were White (by study design), and >60% were married or living as married. For partnered sexual activity analyses, compared to no sexual activity, 3,263 were included in global QOL analyses and 2,576 for HRQL analyses. For sexual functioning analyses, 2,576 were included in global QOL analyses and 1,876 for HRQL analyses (Supplementary Tables S1 and S2, Supplementary Figs. S1 and S2).
Characteristics at Participant's First Visit Included in Analyses
First collected at screener (conducted before baseline visit); N = 3,263.
First collected at sixth annual follow-up; N = 2,576.
HT, hormone therapy; QOL, quality of life; SD, standard deviation; SF-36, short form-36.
Sexually active with a partner versus inactive
Global QOL
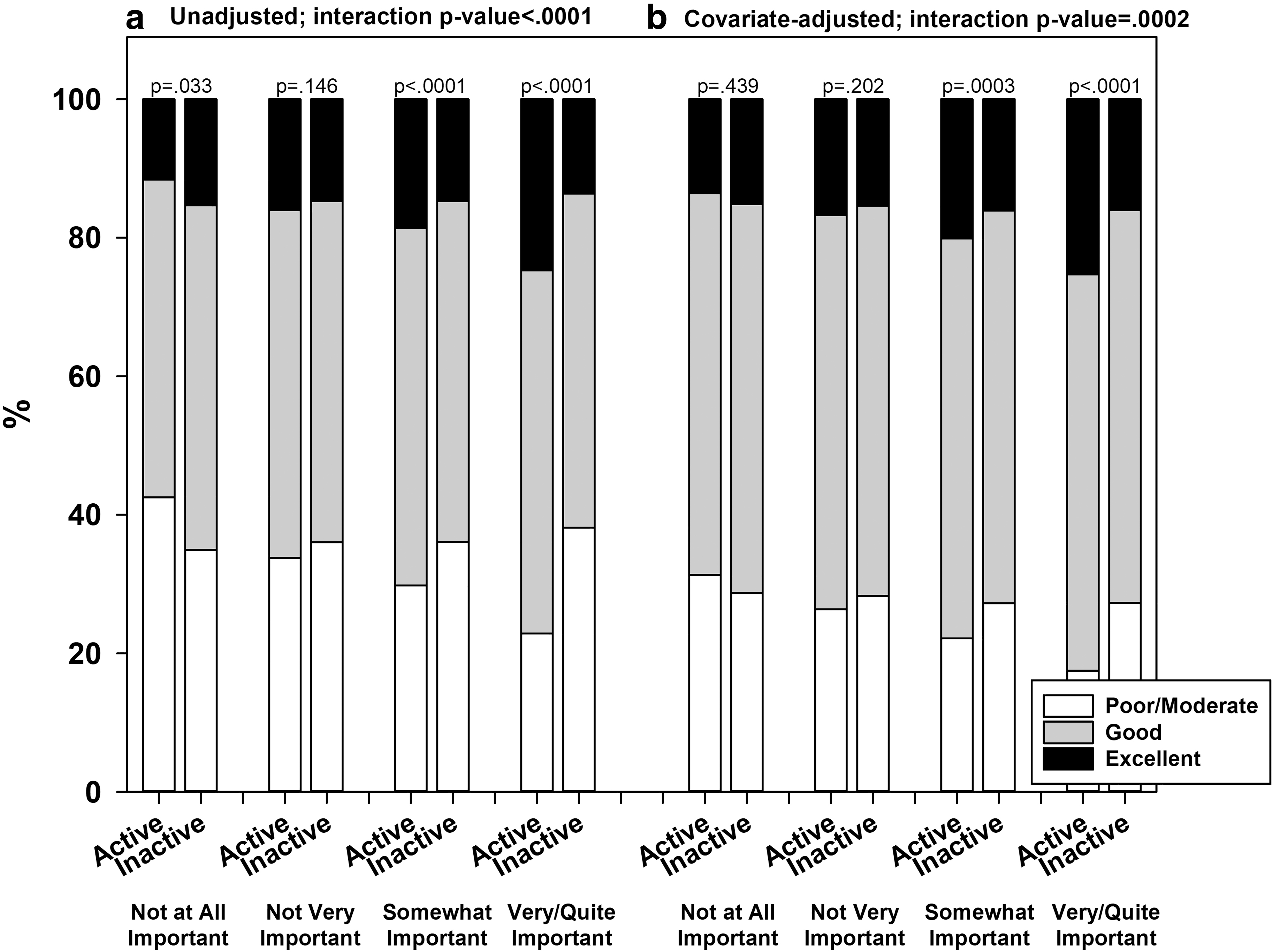
In unadjusted analyses, partnered sexual activity was associated with better global QOL (p < 0.0001). Global QOL percentages for those with (without) partnered sexual activity were 28.5% (35.7%) for poor/moderate, 52.0% (49.5%) for good, and 19.5% (14.8%) excellent. Covariate adjustment attenuated but did not eliminate these differences (p < 0.0001): 26.8% (31.7%), 56.8% (54.9%), and 16.4% (13.4%), respectively. Importance of sex modified this association before and after covariate adjustment (Fig. 1a, b). In unadjusted analyses, when sex was not at all important, QOL was lower—rather than higher—with partnered sexual activity (p = 0.033), with the percentage reporting poor/moderate 31.3% versus 28.7%. Otherwise, QOL was higher with partnered sexual activity, with the difference widening with greater importance of sex. Differences were attenuated with covariate adjustment, but effect modification remained significant (p = 0.0002).
Health-related quality of life
Before covariate adjustment, partnered sexual activity was associated with higher mean PCS (Table 2; 50.00 (0.18) vs. 48.02 (0.20), p < 0.0001) and MCS (51.31 (0.18) vs. 50.67 (0.19), p = 0.0022). Covariate-adjusted associations were smaller and no longer statistically significant. For PCS, effect modification by importance of sex was not statistically significant regardless of covariate adjustment. For MCS, before covariate adjustment, the difference by partnered sexual activity varied significantly by importance of sex (interaction p-value = 0.0168), ranging from a mean difference of −1.27 (0.68)—that is, lower MCS with partnered sexual activity—for sex not at all important to 1.42 (0.51) for sex very/quite important. Covariate-adjusted effect modification and differences by partnered sexual activity were not statistically significant.
Mean Physical Component Summary and Mental Component Summary by Partnered Sexual Activity and Importance of Sex
Bolded p-values are significant p < 0.05.
10,317 observations from 2,576 participants
p-value for active × importance of sex.
Sample size and covariates for PCS: 10,173 observations from 2,548 participants; adjusted for race/ethnicity, site, age, menopause status, financial strain, marital status, education, any difficulty sleeping, number of comorbidities, vaginal dryness, urine leakage, physical activity, BMI, smoking, CES-D. Sample size and covariates for MCS: 9,905 observations from 2,437 participants; adjusted for race/ethnicity, site, age, menopause status, financial strain, marital status, education, any difficulty sleeping, self-reported health, negative life events, perceived stress, trait anxiety, vaginal dryness, urine leakage, CES-D.
BMI, body mass index; CES-D, Center for Epidemiologic Studies Depression; MCS, mental component summary; PCS, physical component summary; SE, standard error.
Sexual functioning score
Global QOL
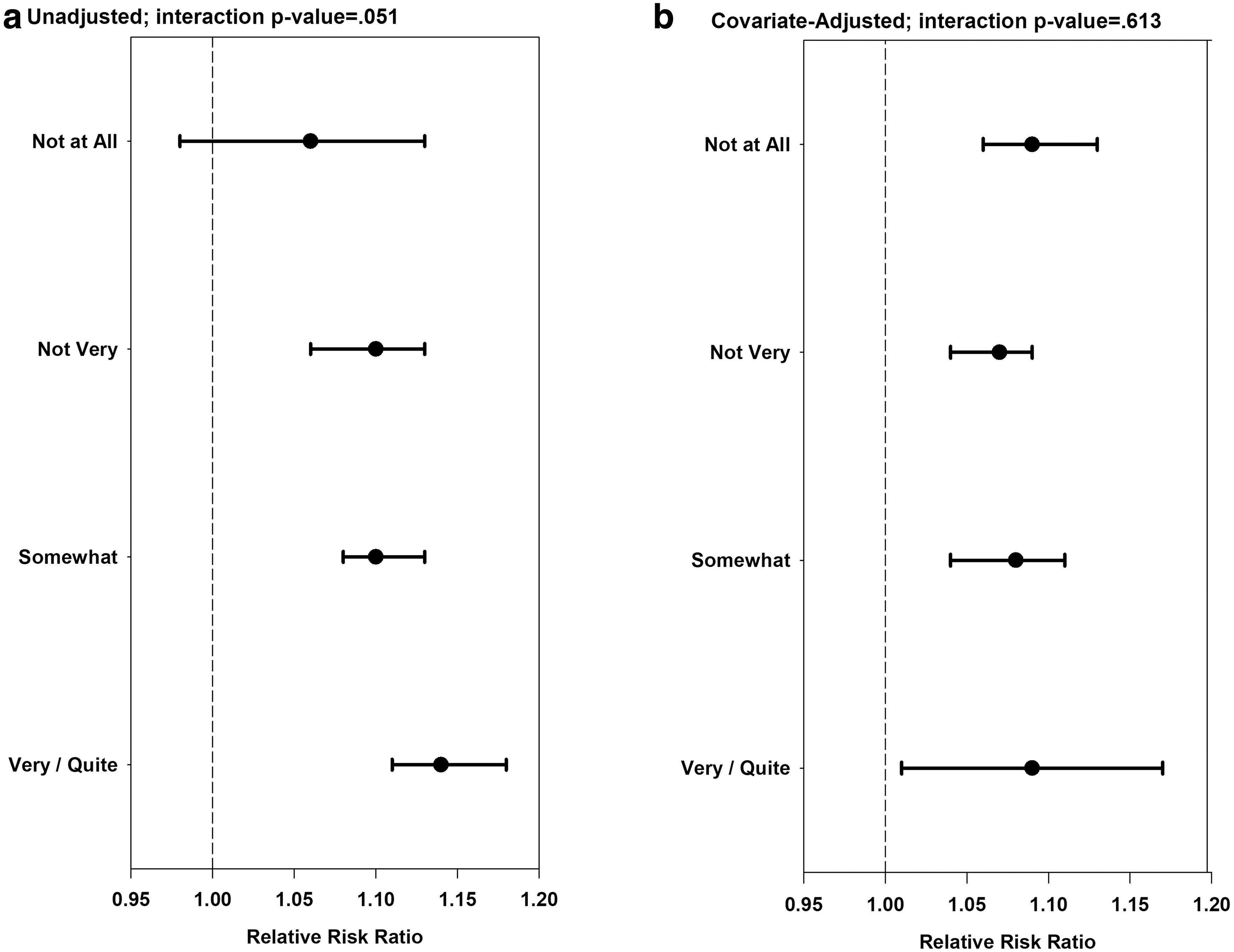
At visits with partnered sexual activity, sexual functioning score was significantly positively associated with better global QOL. Before covariate adjustment, the odds ratio (95% confidence interval [CI]) for global QOL corresponding to a 1-unit increase in sexual functioning score was 1.12 (1.10–1.14), p < 0.0001. The covariate-adjusted odds ratio was slightly attenuated, at 1.08 (1.06–1.10), p < 0.0001. Importance of sex modified the association of sexual functioning score and global QOL in unadjusted analyses (Fig. 2a; p-value for interaction = 0.051); the odds ratio (95% CI) for sexual functioning score increased from 1.05 (0.98–1.13) for sex not at all important to 1.14 (1.11–1.18) for sex very/quite important. In covariate-adjusted analyses (Fig. 2b), sexual functioning score remained significantly associated with global QOL but effect modification was not statistically significant.
Health-related quality of life
Sexual functioning score was significantly positively associated with PCS (β [SE] = 0.14 [0.03]) and MCS (β [SE] = 0.28 [0.04]) in unadjusted analyses (Table 3). Covariate adjustment attenuated both associations, and the former was no longer statistically significant. Importance of sex significantly modified associations with PCS (p = 0.02) and MCS (p < 0.0001) before covariate adjustment. Sexual functioning score was negatively related to both PCS and MCS for sex not at all important although not statistically significant (p > 0.05), but positively associated at other levels of importance, with the strongest associations for very/quite important (β [SE] = 0.19 [0.07] for PCS, 0.55 [0.08] for MCS). Covariate-adjusted associations with PCS in the somewhat and very/quite important categories were attenuated, and effect modification was no longer statistically significant (p = 0.07). For MCS, effect modification remained statistically significant (p = 0.005) but associations were attenuated and only the association for very/quite important remained statistically significant (β [SE] = 0.24 [0.06]).
Physical Component Summary and Mental Component Summary Versus Concurrent Sexual Functioning Score, Visits with Partnered Sexual Activity
Bolded p-values are significant p < 0.05.
6,019 observations from 1,876 participants.
p-value for sexual functioning score × importance of sex.
Sample size and covariates for PCS: 5,931 observations from 1,852 participants; adjusted for race/ethnicity, site, age, menopause status, financial strain, marital status, education, any difficulty sleeping, number of comorbidities, vaginal dryness, urine leakage, physical activity, BMI, smoking, CES-D. Sample size and covariates for MCS: 5,803 observations from 1,789 participants; adjusted for race/ethnicity, site, age, menopause status, financial strain, marital status, education, any difficulty sleeping, self-reported health, negative life events, perceived stress, trait anxiety, vaginal dryness, urine leakage.
Discussion
Consistent with other studies that have examined sexual dysfunction, 20,21 we found that sexual functioning was significantly related to both global QOL and HRQL in unadjusted analyses. When adjusted for a wide range of covariates (including marital status, sociodemographic factors, health, and psychosocial factors), sexual functioning remained independently related to global QOL and the MCS, but not the PCS. Our finding with respect to the PCS is similar to that of Biddle et al. 21 It is not surprising that sexual functioning was unrelated to physical aspects of HRQL when adjusted for relevant covariates, as symptoms and comorbidities are likely to have a greater impact on PCS than sexual functioning. Unlike Biddle et al., we found that sexual functioning score remained related to the MCS even after adjustment. This difference may reflect Biddle's study design which measured HSDD using a combination of low desire and high distress, rather than the importance of sex. We also found that importance of sex served as an effect modifier for sexual function and unadjusted global QOL, MCS, and PCS, but only for MCS after covariate adjustment.
Other studies have not examined the association between being sexually active with a partner and QOL or HRQL. Although we found that being sexually active with a partner was related to global QOL and both the PCS and MCS in unadjusted analyses, the differences in PCS and MCS scores between active and inactive were quite small (1.93 points on the PCS and 0.61 on the MCS). Being sexually active with a partner was related only to global QOL when adjusted for covariates (including marital status). Importance of sex was an effect modifier for both global QOL and MCS in unadjusted analyses, but only for global QOL when adjusted for covariates. These results suggest that for older women being sexually active with a partner is independently related to global QOL, but not HRQL, and that this association is strongest when sex is more important.
This study has several limitations. Although results are based on longitudinal data, analyses do not address the temporal ordering between sexual functioning and outcomes. It is likely that the relationships between sexual activity and sexual functioning and QOL/HRQL are reciprocal. In addition, partnered sexual activity and higher sexual functioning may be markers of closer relationships and companionship, which may contribute to higher QOL/HRQL, although we did adjust for marital status. Analyses related to HRQL only included women who were still active in SWAN at visit 06 and beyond. These women were older on average and, thus, were less likely to contribute visits during pre- and early perimenopause or to contribute visits with concurrent partnered sexual activity; they also reported lower financial strain.
Our results suggest that being sexually active with a partner and having better sexual functioning are related to global QOL for mid-aged women, even after adjusting for a wide range of variables. This association is somewhat stronger when sex is considered important. Being sexually active with a partner and having better sexual functioning is less consistently related to HRQL when adjusted for covariates, and importance modifies only the association between sexual functioning and MCS.
Important strengths of this study include: (1) the availability of multiple covariates related to QOL and HRQL; (2) the ability to assess measures of sexual function and key covariates with longitudinal data; (3) a diverse sample with respect to race, ethnicity, and geography; and (4) the inclusion of the importance of sex as an effect modifier. This study adds to the literature on both global QOL and HRQL by demonstrating the role that sexual functioning has in evaluating QOL. Although many factors have been included in studying QOL/HRQL, sexual functioning has typically been omitted.
Conclusions
Results of this study of midlife and older women suggest that partnered sexual activity and sexual function impact women's QOL and HRQL well into older adulthood. Understanding the importance of sex to midlife and older women contextualizes the impact of sex on QOL.
Footnotes
Acknowledgments
Clinical Centers: University of Michigan, Ann Arbor—Carrie Karvonen-Gutierrez, PI 2021–present, Siobán Harlow, PI 2011–2021, MaryFran Sowers, PI 1994–2011; Massachusetts General Hospital, Boston, MA—Sherri-Ann Burnett-Bowie, PI 2020–Present; Joel Finkelstein, PI 1999–2020; Robert Neer, PI 1994–1999; Rush University, Rush University Medical Center, Chicago, IL—Imke Janssen, PI 2020–Present; Howard Kravitz, PI 2009–2020; Lynda Powell, PI 1994–2009; University of California, Davis/Kaiser—Elaine Waetjen and Monique Hedderson, PIs 2020–Present; Ellen Gold, PI 1994–2020; University of California, Los Angeles—Arun Karlamangla, PI 2020–Present; Gail Greendale, PI 1994–2020; Albert Einstein College of Medicine, Bronx, NY—Carol Derby, PI 2011–present, Rachel Wildman, PI 2010–2011; Nanette Santoro, PI 2004–2010; University of Medicine and Dentistry New Jersey Medical School, Newark Gerson Weiss, PI 1994–2004; and the University of Pittsburgh, Pittsburgh, PA—Rebecca Thurston, PI 2020–Present; Karen Matthews, PI 1994–020.
NIH Program Office: National Institute on Aging, Bethesda, MD—Rosaly Correa-de-Araujo 2020–present; Chhanda Dutta 2016–present; Winifred Rossi 2012–2016; Sherry Sherman 1994–2012; Marcia Ory 1994–2001; National Institute of Nursing Research, Bethesda, MD—Program Officers. Central Laboratory: University of Michigan, Ann Arbor—Daniel McConnell (Central Ligand Assay Satellite Services). Coordinating Center: University of Pittsburgh, Pittsburgh, PA—Maria Mori Brooks, PI 2012–present; Kim Sutton-Tyrrell, PI 2001–2012; New England Research Institutes, Watertown, MA—Sonja McKinlay, PI 1995–2001. The authors thank the study staff at each site and all the women who participated in SWAN. Steering Committee: Susan Johnson, Current Chair; Chris Gallagher, Former Chair.
The authors thank the study staff at each site and all the women who participated in SWAN.
Disclaimer
The content of this article is solely the responsibility of the authors and does not necessarily represent the official views of the NIA, NINR, ORWH, or the NIH.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
The Study of Women's Health Across the Nation (SWAN) has grant support from the National Institutes of Health (NIH), DHHS, through the National Institute on Aging (NIA), the National Institute of Nursing Research (NINR), and the NIH Office of Research on Women's Health (ORWH) (Grants U01NR004061; U01AG012505, U01AG012535, U01AG012531, U01AG012539, U01AG012546, U01AG012553, U01AG012554, U01AG012495, and U19AG063720).
Supplementary Material
Supplementary Figure S1
Supplementary Figure S2
Supplementary Table S1
Supplementary Table S2
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.