
Abstract
Objectives:
Although invasive cervical cancer (ICC) rates have declined since the advent of screening, the annual age-adjusted ICC rate in the United States remains 7.5 per 100,000 women. Failure of recommended screening and management often precedes ICC diagnoses. The study aimed to evaluate characteristics of women with incident ICC, including potential barriers to accessing preventive care.
Materials and Methods:
We abstracted medical records for patients with ICC identified during 2008–2020 in five U.S. population-based surveillance sites covering 1.5 million women. We identified evidence of adverse social and medical conditions, including uninsured/underinsured, language barrier, substance use disorder, incarceration, serious mental illness, severe obesity, or pregnancy at diagnosis. We calculated descriptive frequencies and compared potential barriers by race/ethnicity, and among women with and without symptoms at diagnosis using chi-square tests.
Results:
Among 1,606 women with ICC (median age: 49 years; non-White: 47.4%; stage I: 54.7%), the majority (68.8%) presented with symptoms. Forty-six percent of women had at least one identified potential barrier; 15% had multiple barriers. The most common potential barriers among all women were being underinsured/uninsured (17.3%), and language (17.1%). Presence of any potential barrier was more frequent among non-White women and women with than without symptoms (p < 0.05).
Conclusions:
In this population-based descriptive study of women with ICC, we identified adverse circumstances that might have prevented women from seeking screening and treatment to prevent cancer. Interventions to increase appropriate cervical cancer screening and management are critical for reducing cervical cancer rates.
Introduction
Worldwide, over half a million new cervical cancer cases are diagnosed yearly, most occurring in low- and middle-income countries. 1 In the United States, cervical cancer is the fourth most common cancer among women with about 13,000 new cases and 4,000 deaths yearly. 2,3 Half of diagnoses occur in women aged <50 years; one quarter are among young women aged 25–39 years. 2 Cervical cancer diagnosis and treatment can have devastating effects on women and their families for numerous reasons, including future infertility and premature mortality. 3
Almost all cervical cancer is caused by persistent infection with oncogenic human papillomavirus (HPV) types. 4 However, most cervical HPV infections are transient. HPV detection, based on cytologic changes (Papanicolaou [Pap] test) or on a molecular test, forms the basis of screening for asymptomatic precancerous lesions. Precancers can regress or persist, potentially progressing to invasive cervical cancer (ICC) after years or decades. Primary prevention of HPV infection through vaccination, which targets HPV types that most commonly cause cancer, was introduced in the United States in 2006 for female adolescents with catch-up through age 26. 5 The impact of vaccination on cervical cancer will be realized over years to decades as vaccinated girls/women age into older age groups. 5
Although cervical cancer was once a leading cause of cancer deaths among women, U.S. cervical cancer incidence and mortality have greatly declined since screening was introduced. 6 The goal of screening is to detect and allow treatment of precancers before they progress. Guidelines have changed over time; currently, women are recommended to receive screening every 3 or 5 years depending on their risk and the test used. However, even with readily available screening in the United States through private insurance and public programs, the annual age-adjusted rate of new cervical cancers has stagnated at about 7.5 per 100,000 women. U.S. women identifying as Black or Hispanic have higher rates of cervical cancer, and are more likely to be diagnosed later or die from cervical cancer compared to women of other races or ethnicities. 2 Inadequate screening and lack of follow-up of abnormal results are known impediments to detection and treatment of precancers. 7,8
Although screening is safe and effective, almost one-quarter of U.S. women aged 45–64 years have not received timely screening. 9 Previous publications have identified individual and structural/systemic barriers to prevention; 10 these include lack of health insurance, 8,11 lack of language services, 11 competing health care demands from another medical condition, 12 and certain sociocultural beliefs. 8,13 Most population-based data on cervical cancers are limited to information reported to cancer registries, including race, ethnicity, histology, and vital status. These data are invaluable in understanding trends in disease, but do not inform an understanding of the circumstances women experienced that may have contributed to a failure of cancer prevention. Here, we describe sociodemographic and clinical characteristics of women with ICC from a 5-site population-based surveillance system.
Materials and Methods
The Human Papillomavirus Vaccine Impact Monitoring Project (HPV-IMPACT) began in 2008 as a U.S. multisite, population-based, active laboratory surveillance system for cervical precancer, with sites in Oregon (28 zip codes, Portland metropolitan area), California (8 cities, Alameda County), New York (Monroe County), Connecticut (New Haven County), and Tennessee (Davidson County). 14 In 2017, the California site expanded retroactively to all of Alameda County, resulting in HPV-IMPACT having a 5-site catchment area home to ∼1.5 million women. Starting in 2019, the project included ICC cases retrospectively from 2008. Histologically confirmed incident cervical carcinoma cases among women aged ≥18 years were identified by state cancer registries and reports from histopathology laboratories. Sites also reported a small number of clinically diagnosed cases (by cytology and/or imaging) that were not histologically confirmed.
Sites identified and reported all cancers diagnosed in catchment area residents in 2008–2020, and abstracted medical records from all relevant cancer care providers (e.g., primary care, gynecology, hospital). Cases reported without completed medical record chart abstraction by November 1, 2022, were excluded.
Demographic data collected included age and year of diagnosis, race/ethnicity, and insurance status (public, private, no insurance, unknown). Clinical information collected included symptoms at presentation (yes, no, unknown), symptoms (vaginal bleeding, pelvic pain, pain with intercourse, and a free-text field “other”). Free text from the symptoms category “other” were categorized and grouped as pain, genitourinary, constitutional, gastrointestinal, and other. We collected Pap and HPV tests in the 5 years preceding diagnosis, exposures that might influence natural history (immunocompromising medical conditions, history/current cigarette smoking, diethylstilbestrol exposure), cancer stage (International Federation of Gynecology and Obstetrics [FIGO] staging system: Stages I–IV, other, unknown), histologic type (squamous cell, adenocarcinoma, adenosquamous, other carcinoma, multiple types, unknown), history of HPV vaccination (yes, no, unknown), and vaccination date. We also identified women with precancers reported to HPV-IMPACT previously.
Potential barriers to preventive care
Abstractors at each site identified chart-based evidence of social and medical conditions hypothesized to interfere with accessing screening and management of cervical disease within the 5 years before cancer diagnosis (Supplementary Table S1). Hereafter, we refer to these conditions simply as “barriers.” Barriers were predefined in our data collection instrument because they were either previously identified in the literature 8,12 or in a pilot study 15 : uninsured/underinsured; utilization of translation services, non-U.S.-born, or preferred language other than English (language barrier); current/history of substance use disorder; severe obesity (body mass index ≥40); current/history of housing insecurity; current/history of incarceration; current/history of serious mental illness; and pregnant at diagnosis. Abstractors at two sites also reported additional adverse circumstances noted in charts that did not meet a priori definitions.
Additional potential barriers constructed from these abstractor notes were current/history of chronic medical condition, and medical system disengagement (e.g., lack of care for years, lost to medical follow-up, distrust, and/or fear of the medical system).
Test history
Pap and HPV tests were categorized by temporal relationship to cancer diagnosis. The first category, “Pap or HPV test within 6 months prior to cancer diagnosis,” likely captured tests performed as part of a cancer workup due to temporal proximity; other studies 7,16,17 have defined this time frame as “prediagnostic.” We further stratified these as symptomatic and asymptomatic/unknown. The second category, “test occurring ≥6 months before cancer diagnosis,” was more likely to have been a routine screen, rather than part of a diagnostic evaluation. The other categories were “no tests documented,” or “tested, date unknown.”
Test results
HPV test results were categorized as high-risk positive, high-risk negative, or unknown. Pap test results were categorized as abnormal, normal, or unknown. For Pap tests, unknown included samples that were unsatisfactory or could not otherwise be evaluated by the reading pathologist. Abnormal Pap results were reported using the Bethesda System for Reporting Cervical Cytology. 18
Statistical analyses
We calculated descriptive frequencies of demographic and clinical characteristics, test history, and potential barriers for all women with invasive cancer. Test history, symptoms, stage at diagnosis, and a priori barriers identified for ≥100 women were compared by race/ethnicity, using chi-square tests, with p < 0.05 indicating statistical significance. Women with and without symptoms at diagnosis were compared. Analyses were conducted using SAS (version 9.4).
Ethics
As public health surveillance, this work was exempt from review by the Institutional Review Board (IRB) at Centers for Disease Control and Prevention (CDC) and University of Rochester School of Medicine and Dentistry, and was reviewed and deemed nonresearch by Vanderbilt University Medical Center, Oregon Department of Human Services, and the Connecticut Department of Public Health. The project was approved by the IRBs at Kaiser Permanente Northern California, California Department of Public Health and University of California, Berkeley. Activities were reviewed by CDC and done in accordance with applicable federal law and CDC policy.
Results
Demographic and clinical characteristics
During 2008–2020, 1,696 ICC cases were reported; of these, 1,606 (94.7%) had complete data at the time of analysis (1,599 histologically confirmed). A total of 113 (7.0%) women with cancer had a precancer reported to HPV-IMPACT ≥6 months before diagnosis. The median age at cervical cancer diagnosis was 49 years (interquartile range: 39–61) (Table 1). Of women with cervical cancer, 52.6% identified as White, non-Hispanic; almost half (47.7%) had public health insurance, 40.3% had private insurance, and 6.3% were uninsured.
Demographic and Clinical Characteristics of Women with Invasive Cervical Cancer, Human Papillomavirus Vaccine Impact Monitoring Project, 2008–2020
Symptoms/signs and immunocompromise categories were not mutually exclusive.
Other constitutional symptoms comprised bloating, decreased appetite, fever/chills/hot flashes, headache, weight gain.
Ten cases were Stage II but not specified whether IIA or IIB.
Within 6 months before diagnosis was chosen as a category because this was considered to be within the time frame of a workup for cancer, rather than a screening test.
The majority (68.8%) of women with cancer had symptoms or signs at diagnosis, most commonly vaginal bleeding or discharge (61.0%), pelvic pain (18.9%), or a mass (6.1%). Almost 10% (9.7%) had immunocompromising conditions, most commonly renal failure or dialysis; <1% had documented HIV infection. Stage at diagnosis was Stage I, 54.7%; Stages II–IV, 40.4%, including 14.9% stage II, 14.6% stage III, 11.0% stage IV; and unknown, 4.9%. The predominant histology was squamous cell carcinoma (62.1%).
More than two-thirds of women with cervical cancer (68.9%, 1,106/1,606) had ≥1 Pap test, HPV test, or cotest preceding diagnosis. Over one quarter (30.0%, 481/1,606) were tested ≥6 months before diagnosis, which was likely a routine screen. Half (49.6%, 796/1,606) had a test <6 months before cancer diagnosis, including one-third of women whose only documented test occurred <6 months before diagnosis (33.6%, 539/1,606). A lower proportion of women (55/155, 35.5%) with immunocompromise underwent a screen test than women with cervical cancer overall. This included those with the most common immunocompromising condition evaluated, renal failure or dialysis, where 46.5% (20/43) were screened (not shown).
Among women with Pap or HPV test results available, most had abnormal results regardless of cancer histologic type (Supplementary Table S2). However, among those diagnosed with squamous cell carcinoma, 7.0% had a normal Pap test preceding diagnosis, and among those with adenocarcinoma, 18.8% had a normal Pap test preceding diagnosis.
Overall, 38 (2.4%) had documented history of HPV vaccination; 15.6% (n = 251) were aged ≤26 years in 2006 (i.e., age-eligible for HPV vaccination) (not shown). 19 Of 33 women with documented vaccination date, none was vaccinated at age 11–12 years (the recommended routine age). Twenty-one (63.6%) were vaccinated at catch-up ages, including 4 in adolescence [ages 13–17]), and 17 at ages 20–26; 12 (36.4%) were vaccinated at older ages (range: 34–42).
Barriers to preventive care
Almost half of women with cancer (45.9%) had ≥1 barrier to preventive care identified; 30.4% had one identified barrier; 15.5% had multiple barriers (Table 2). The most frequently identified barriers were being uninsured/underinsured (17.3%), language barrier (17.1%), and serious mental illness (10.7%). Among the two sites that frequently reported additional barriers using free text, two barriers appeared frequently: 9.9% (87/877) had a chronic medical condition identified in chart abstraction and 18.5% met our definition of medical system disengagement (162/877) (not shown).
Characteristics and Barriers to Preventive Care Among 1,606 Women with Invasive Cervical Cancer, by Race/Ethnicity, Human Papillomavirus Vaccine Impact Monitoring Project, 2008–2020
Barriers with N < 100 not shown by race/ethnicity. See Methods section text and Supplementary Table for definitions of barriers.
p < 0.05 by race; Chi square tested among those with stage known only for stage, and among squamous versus adenocarcinoma for cancer type.
Stage unknown not shown by race/ethnicity due to small numbers.
Cancer types other than squamous cell carcinoma and adenocarcinoma not shown by race/ethnicity due to small numbers.
Among women with known stage, similar proportions with any versus no barrier (42.5% vs. 42.3%) were diagnosed at stages II–IV (not shown). Barriers were equally frequent among those with and without history of documented screen test before diagnosis (46% for both).
Barriers and other clinical characteristics by race/ethnicity
Compared to women with ≥1 barrier, women with no barrier were more frequently White, non-Hispanic than other race/ethnicities (p < 0.05) (Table 2). Over two-thirds (69.8%) of women identifying as Hispanic had ≥1 barrier, compared to about half of Black, non-Hispanic (49.0%) and Asian, and non-Hispanic women (51.1%). The most common barrier identified among Hispanic and Asian women was language (56.4% and 42.6%, respectively), and the most common barrier among Black, non-Hispanic women and White, non-Hispanic women was uninsurance or underinsurance (19.4% and 16.2%, respectively). Women with ≥1 barrier more frequently had private health insurance (not shown; p < 0.05).
A greater proportion of Black, non-Hispanic women compared to other racial/ethnic groups presented with symptoms on cervical cancer diagnosis (p < 0.05). Similarly, Black, non-Hispanic women had a comparatively higher proportion diagnosed at advanced stage (p < 0.05). Black, non-Hispanic women were also disproportionately diagnosed with squamous cell carcinoma. Test history was similar across racial/ethnic groups.
Characteristics associated with symptoms at diagnosis
Women presenting with symptoms at cancer diagnosis differed from those with no documented symptoms by several characteristics (Table 3). Compared with women with no symptoms at diagnosis, those with symptoms were older (median age 51 vs. 43 years), were more likely to have public insurance, to have Stage II-IV cancer, and to be diagnosed with squamous cell carcinoma. Presence of any barrier was more frequent among women with symptoms than without symptoms (48.1% vs. 41.1%, p < 0.05) (Fig. 1).
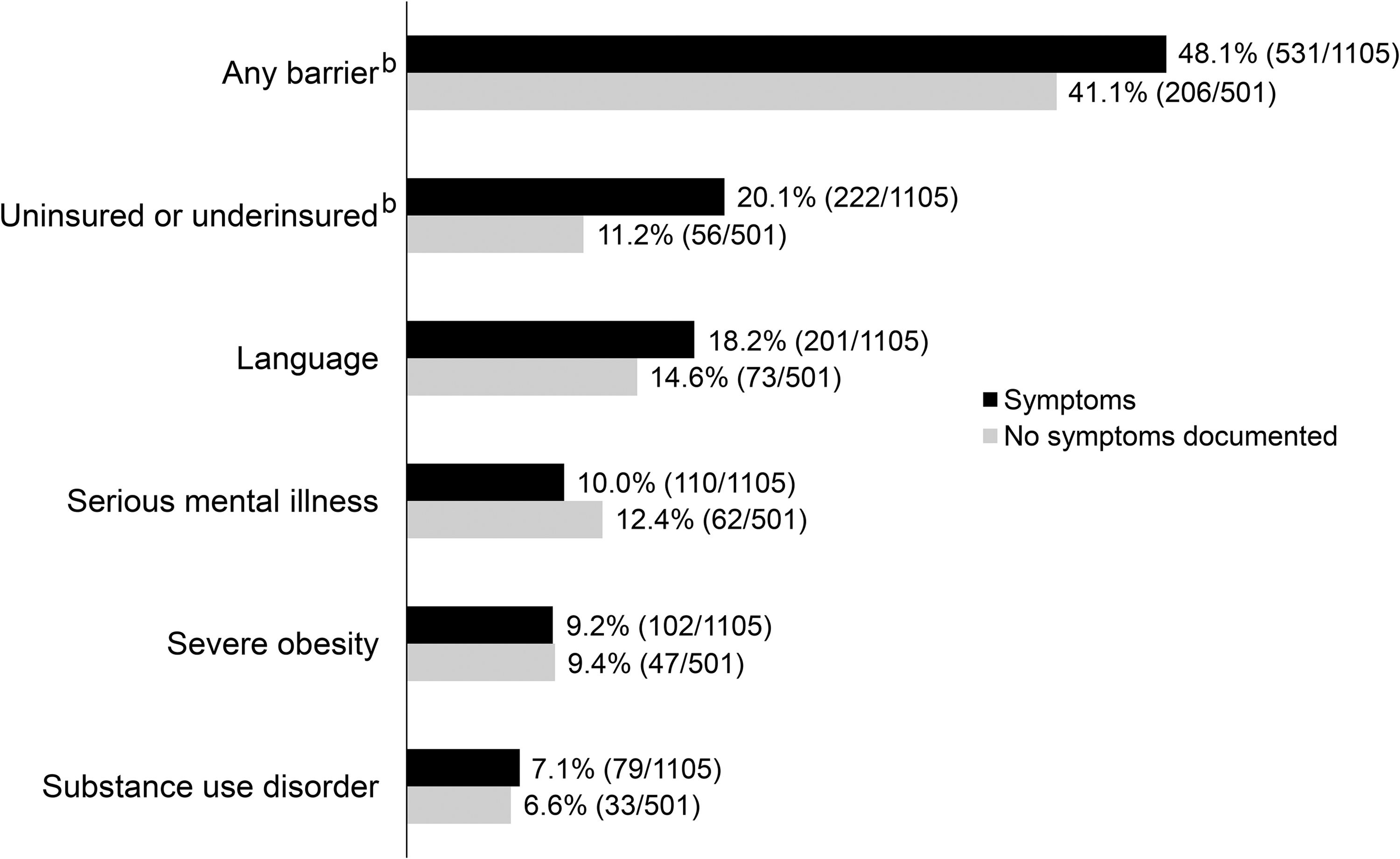
Prevalence of selected barriersa among women with and without symptoms at invasive cervical cancer diagnosis, HPV-IMPACT, 2008–2020.aBarriers with N < 100 not shown. See Methods section text and Supplementary Table S1 for definitions of barriers.bSignificant difference between those with and without symptoms (p < 0.05).HPV-IMPACT, Human Papillomavirus Vaccine Impact Monitoring Project.
Characteristics and Barriers to Preventive Care Among 1,606 Women with Invasive Cervical Cancer, by Symptoms at Diagnosis, Human Papillomavirus Vaccine Impact Monitoring, 2008–2020
p < 0.05 by symptom history.
Chi square tested only among those with known stage.
Chi square tested among those with squamous cell and adenocarcinoma only.
Barriers with N < 100 not shown by symptom history. See Methods section text and Supplementary Table for definitions of barriers.
Pap/HPV test history was also associated with symptoms. A smaller proportion of women with symptoms (714/1,105, 64.6%) compared with those without symptoms (392/501, 78.2%) had a screen test documented before cancer diagnosis. Of all women who had a test within 6 months before diagnosis, 484 had symptoms (suggesting the test was part of a diagnostic evaluation), whereas 312 had no symptoms documented, suggesting that their cancers were screen-detected.
Of all 1,606 women with cancer in our analysis, 378 (23.5%) were diagnosed by abnormal Pap/HPV in the absence of symptoms, consistent with routine screening (not shown). Among these, 331 (87.6%) were Stage I, 19 (5.0%) were Stage II, 9 (2.4%) were Stage III, and 2 (0.5%) were Stage IV.
Discussion
Although substantial additional cervical cancer prevention related to HPV vaccination is expected in the coming years, ICC is largely preventable now with currently available screening and treatment of precancers. 6 In this population-based study, we report demographic and clinical characteristics, testing history, and potential barriers to preventive care among women with ICC. These data are unique in that they represent all cancers diagnosed in catchment area residents, including in medically underserved residents. The majority of women diagnosed with cervical cancer had symptoms on presentation, indicating that their cancers were likely not screen-detected during routine preventive care. Less than one-third of women with cancer had evidence of routine screening.
In our analysis, almost half of women had at least one potential barrier to preventive care identified; 15% had multiple barriers. Underinsurance, language or immigration status, serious mental illness, and severe obesity were the most frequently identified barriers. In the abstractor notes at two sites, we found that “medical disengagement” described barriers to engaging with the health care system; the frequency of this barrier highlights the complex emotional and sociocultural factors involved in accessing preventive health care or cervical cancer screening. Medical system disengagement due to fear or distrust results in patients avoiding the medical system altogether, until they experience a serious outcome. Competing medical conditions might result in patients prioritizing treatment over preventive care such as cancer screenings, which may not seem as urgent. Barriers were more frequent among those with symptoms; symptoms were more likely among Black, non-Hispanic women, who have higher rates of cervical cancer mortality.
Consistent with other studies conducted in the United States and other developed countries, 20 –22 we found that cervical cancer still often presents symptomatically; two-thirds of women had symptoms at diagnosis indicating that cancer was not detected during preventive health care. Symptomatic cancers were more likely to be a higher stage at diagnosis, and were more common in unscreened women. Barriers were more frequent among those with symptoms compared to those without, similar to a UK retrospective study. 21
Several previous studies have examined barriers to cervical cancer screening in specific populations, 8,11 –13,15,23 using in-person or telephone-based surveys among cervical cancer survivors, women presenting for screening, and focus groups. Much of the literature, even that using chart review, 23 describes barriers to screening in the general population, not necessarily among women with cervical cancer. These have identified systemic barriers such as poor access to health care services, insurance or financial status, and lack of interpreter services, and personal barriers, including lack of knowledge, fear of finding cancer, or anxiety. 11,24 In a telephone survey of women with health insurance, those with multiple chronic conditions were less likely to have been screened for cervical cancer 12 ; possibly because disease management took priority over preventive health care.
Obesity is a known barrier to preventive care in general, and has been specifically associated with lack of appropriate screening before cervical cancer diagnosis, and underdetection in those who are screened. 25 –27 A recent study of women with severe mental illness documented a screening rate less than half of that in the general population. 28 In our study, women with immunocompromise, including those with renal failure or dialysis, were screened less frequently than women with cancer overall. While patients with renal failure or dialysis are not considered immunocompromised according to cervical cancer screening guidelines, they may have increased risk for cervical cancer, which may be due to lack of screening or a biological mechanism. 29,30
In the United States, women identifying as Black or Hispanic have higher rates of cervical cancer, and are more likely to be diagnosed later or die from cervical cancer compared to women of other races or ethnicities. 2 We found that the predominant barriers differed by race/ethnicity, similar to other reports. 31 –34 Language as a barrier was most frequent among women who identified as Hispanic and Asian, while underinsurance was most frequent among those who were Black, non-Hispanic and White, and non-Hispanic. In our analysis, White, non-Hispanic women were most likely to have had a screen test before cancer diagnosis. Black, non-Hispanic women were more likely to present with symptoms, at more advanced stages than other racial/ethnic groups, and were more likely to have squamous cell carcinoma, consistent with other reports. 35,36
Several previous studies found that levels of medical mistrust were higher in racial/ethnic minority women 37 –39 ; although this construct was not evaluated systematically in our analysis, it was explored using data from two sites. A systematic review among immigrant and ethnic minorities in the United States identified sociocultural factors influencing health-related beliefs that impact health care utilization. 40 Other studies describe sociocultural beliefs that may contribute barriers to preventive care, 8,10,13,16 such as distrust of the medical system, fear of being diagnosed with cancer, or lack of knowledge about cervical cancer screening. Similarly, a survey of uninsured women presenting for subsidized cervical cancer screening identified cost, fear of finding cancer, and anxiety as among the most common barriers to receiving a Pap test. 13 Outreach focusing on women who do not access the health care system and those who engage with care for chronic conditions only is needed.
Notably, 55% of women did not have a prespecified barrier identified in chart abstraction. For context, the frequency of women with “no barrier” in our study is not easily comparable to other studies, since studies used different methods and most did not report “no barrier” as we did. 11,13 Given that many women had evidence of the constructed barriers “chronic medical condition” and “medical system disengagement” when free text from medical chart abstraction was reviewed, we suspect that many challenges women faced to prevention and treatment for cervical cancer were not readily evident from medical charts and are underestimated in this study. Also noted is that the frequency of any barrier was similar among those with stage I versus advanced stage, and among those with a documented screen test versus no test. These findings may also suggest the limitation of chart-based review for finding all true barriers to health care.
In our study, a minority of women had evidence of regular screening. A study of insured women found that most ICC cases were attributable to lack of recent Pap testing. 28 In 2018, 80.5% of U.S. women aged 21–65 reported being up-to-date with cervical cancer screening based on the most recent guidelines, below the Healthy People 2030 target of 84.3%. 41 Some screened women do not follow-up for diagnosis and treatment. 20 Just 7% of invasive cancers in this analysis occurred in women who had a precancer reported to HPV-IMPACT previously. While a few precancers preceding cancer diagnosis might not be captured in this surveillance system if the woman moved into the catchment area more recently, or if precancer was diagnosed before 2008, this low percentage suggests that most cancers were not due to inadequate follow-up or treatment of precancers, but from precancers never having been diagnosed in the first place.
Some groups may be less likely to receive guideline concordant cervical cancer screening, specifically those who are racial or ethnic minorities, have limited English proficiency, or other health conditions. 24 Interventions to increase appropriate cervical cancer screening and management, particularly for women who are underinsured, have competing health priorities, or are underserved in the medical system, are important for reducing cervical cancer incidence and mortality. Interventions under investigation include bundling with other screenings, tailored community education, home self-sampling, and patient navigation. 24,42 –45
While screening can detect precancers and prompt treatment to prevent progression to invasive cancers, HPV vaccination protects against HPV infections that can progress to both precancer and cancer. 46 Few women in this analysis were vaccinated; none at the routinely recommended age of 11 or 12 years. 19 Only 16% were vaccine eligible based on age at the time of HPV vaccine licensure in the United States. Thus, cancers among vaccinated women in this study are probably due to HPV exposure before vaccination and unlikely to be due to vaccine failure. In future HPV-IMPACT analyses, HPV typing data will be available to determine whether vaccine types or nonvaccine types are detected in these cancers.
National data show that among U.S. adolescents aged 13–17 years, coverage with ≥1 HPV vaccine dose in 2021 was 77% and 62% were up-to-date; efforts are ongoing to increase coverage. 47 HPV vaccination should eventually reduce cancers in both vaccinated and unvaccinated individuals, given strong herd protection from HPV vaccination. 48
Our study has several strengths. Because these data were collected from medical charts, they may be less subject to recall, selection, or other biases that may occur when surveying research study participants or health care providers. 8,49 Also, our analysis using population-based public health surveillance data provides a unique window into how women's circumstances might lead to ICC since it includes medical chart information on all women diagnosed with ICC in the catchment areas, including women who may be unlikely to participate in research studies. We acknowledge several limitations. The prevalence of barriers is almost certainly underestimated because some might not be documented. In addition, only individual-level barriers were assessed; additional potential barriers presented by the fragmented health care system were not captured. The data also do not capture information about management or follow-up after abnormal test results or health care encounters.
Conclusions
In this population-based study of U.S. women with cervical cancer, circumstances that might have interfered with adequate preventive care were frequent. Interventions to increase appropriate cervical cancer screening and management, particularly for those who are underserved in the medical system, underinsured, or have competing health priorities or health-related impediments, are important for reducing cervical cancer rates.
Footnotes
Authors' Contributions
All authors made substantial contributions to the concept of the article; H.G.R., J.W.G., and L.E.M. drafted the article; all authors contributed to substantial revision and editing for important intellectual content; all authors approved of the final version of the article.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
National Center for Immunization and Respiratory Diseases, Grant/Award Numbers: U50CK000482, U50CK000484, U50CK000486, U50CK000488, U50CK000491
Supplementary Material
Supplementary Table S1
Supplementary Table S2
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.