
Abstract
Introduction:
Alcohol use (AU) and disorders (AUDs) have been increasing among women over the past decade, with the largest increases among women of child-bearing age. Unprecedented stressors during the COVID-19 pandemic may have impacted AU for women with and without children. Little is known about how these trends are impacting women in the military.
Methods:
Cross-sectional study of active-duty service women (ADSW) in the U.S. Army, Air Force, Navy, and Marine Corps during fiscal years (FY) 2016–2021. We report the prevalence of AU and AUD diagnoses by FY, before/during the COVID-19 pandemic (2016–2019; 2020–2021, respectively), and by parental status. Log-binomial and logistic regressions examined associations of demographics, military, and family structure characteristics, with AU and AUD, during pre-COVID-19 and COVID-19 timeframes.
Results:
We identified 281,567 ADSW in the pre-COVID-19 period and 237,327 ADSW in the during COVID-19 period. The prevalence of AU was lower during the COVID-19 period (47.9%) than during the pre-COVID-19 period (63.0%); similarly, the prevalence of AUD was lower during the COVID-19 period (2.7%) than during the pre-COVID period (4.0%). ADSW with children had larger percentage decreases during the COVID-19 period. ADSW with children had a consistently lower prevalence and odds of AUD compared with ADSW without children in the pre- and during COVID-19 periods.
Conclusion:
Decreasing trends in AU and AUD among ADSW were unexpected. However, the prevalence of AU and AUD may not have been accurately captured during the COVID-19 period due to reductions in access to care. Continued postpandemic comparison of AU/AUD among women by parental status and demographic factors may guide targeted health efforts.
Introduction
Binge drinking, heavy alcohol use (AU), and alcohol-related morbidity and mortality have been increasing in the United States since the early 2000s, with women and middle-aged populations most at risk. 1,2 The National Institute on Alcohol Abuse and Alcoholism (NIAAA) defines binge drinking as five or more drinks per drinking occasion for men and four or more for women; heavy drinking is defined for men as either binge drinking or 15 or more per week, or binge drinking or eight or more drinks per week for women. 2 Per capita alcohol consumption increased by approximately 8% and binge drinking by 7.7% among men and women aged 18 and older since 2000. 1,3,4 From 2006–2018, binge drinking increased among women, regardless of their parenting status, across all age groups. 5 Heavy AU may be particularly consequential for women, as they are at increased risk for liver disease, breast cancer, and alcohol-related consequences compared to men. 6,7
Women with children typically report lower levels of heavy AU and alcohol use disorder (AUD), a medical condition characterized by an impaired ability to stop or control alcohol use despite adverse social, occupational, or health consequences, compared with women without children, yet drinking has been increasing among women with and without children. 2,5,8 –11 Several studies have shown pronounced increases in heavy AU among women in their reproductive years. 5,8 –10 Women with higher levels of education and income have experienced greater increases in binge drinking, which is often associated with delaying or forgoing motherhood. 12 There have also been shifts in cultural norms that may influence drinking among women. Social acceptability of drinking among mothers has shifted, and the alcohol advertising industry has expanded its “pinking” of alcohol products targeting women (e.g., low-calorie wines, hard seltzers). 5,13 Social media has also fostered “mom-wine” culture which has the potential to influence mothers’ drinking behavior—at a time when women’s drinking rates are already increasing. 14,15 The COVID-19 pandemic exacerbated stressors for mothers, including reduced childcare options, distance learning for school-aged children, and isolation from physical support systems, all of which may have created additional reliance on social media and virtual communities. 15 Studies have found that alcohol consumption during the pandemic increased among women and parents. 16,17
The research literature indicates that U.S. military service members represent a subgroup at increased risk for heavy drinking, placing them at risk for AUD. 18,19 In 2013, an Institute of Medicine report on Substance Use in the U.S. Armed Forces declared substance use a public health crisis in the military, with heightened concern for heavy AU. 20 Findings from the 2015 Department of Defense Health-Related Behaviors Survey (DoD HRBS) found, using data from AUDIT-C cut-points of four or more drinks on one occasion for men and three or more for women, that the Marine Corps had the highest prevalence of probable hazardous or disordered alcohol use at 48.6% of Marine Corps respondents, followed by Navy (39.8%), Coast Guard (34.0%), Army (33.1%), and Air Force respondents (26.1%). 21 However, since the U.S. military is predominantly male, there has been far less investigation into heavy AU among female service members, but findings from the 2011 DoD HRBS found that active-duty service women (ADSW) reported using alcohol to cope with emotional problems (e.g., depressed mood) or for reasons consistent with risk-taking propensity. 22 In addition, a study of enlisted ADSW in the Army who returned from an Afghanistan/Iraq deployment in fiscal years 2008–2011 found that ADSW who experienced combat exposure had increased odds of reporting heavy AU upon return from deployment. 23 Notably, this study indicated that ADSW who were mothers had reduced odds of heavy AU compared with women without children. 19
Binge drinking is pervasive in military culture, 20 and alcohol-related morbidity and mortality have been increasing among women of childbearing age in the United States 1 —an age group which includes the majority of women in the military. Despite this potential health risk, there has been little examination into AU and AUD among U.S. ADSW or how the COVID-19 pandemic may have influenced drinking trends in this population. An assessment of alcohol consumption and AUD among ADSW with and without children is needed to better address potential health risks for ADSW and potential impacts on military readiness. We hypothesize that the prevalence of AU and AUD increased during the study period from pre to during COVID-19 among ADSW with and without children and that mothers exhibited a higher rate of increase than nonmothers.
Materials and Methods
Study design, population, and data sources
We conducted a cross-sectional study utilizing beneficiary and health care claims data from the Military Health System (MHS) Data Repository (MDR). The MDR houses all health care encounter and claims data for MHS beneficiaries who receive care either at military treatment facilities (i.e., direct care) or at civilian private sector facilities (i.e., private sector care) using their TRICARE benefit. 24 The study population included all ADSW ages 18 and older in the U.S. Army, Air Force, Navy, and Marine Corps during fiscal years (FYs) 2016–2021, serving both within the United States and abroad. Service women in the National Guard and Reservists, both active and inactive, were excluded. As a requirement of military service, ADSW are required to have an annual physical examination within the MHS, which should provide an opportunity for alcohol screening and identification of potential AUD. Self-reported AU was from the MDR’s vitals file recorded during ambulatory appointments at military treatment facilities. AUD diagnosis data came from the health care claims files from either direct or private sector care. Demographic and military and family characteristics were derived either from the Defense Enrollment Eligibility Reporting System (DEERS) or at the time of encounter if information was missing from their DEERS record. Person-level data were linked by a unique patient identifier across all MDR datasets.
Variables
The study outcomes were as follows: (1) self-reported AU and (2) AUD diagnosis during the pre (i.e., FY 2016–2019) and during COVID-19 (i.e., FY 2020–2021) periods. AU was defined as yes or no based on self-reporting “whether or not the patient uses alcohol” during ambulatory appointments at military treatment facilities and was not captured from health care visits in the private sector. If a patient reported both “yes” and “no” during a timeframe they were recorded as a “yes” to capture the period prevalence. Missing AU data were coded as no in the descriptive and trend analyses (see Supplementary Table S1; imputation was used in the AU regression model—see below). AUD diagnosis was defined as “yes/no” during the pre and during COVID-19 periods and was identified using International Classification of Diseases, 10th revision (ICD-10), diagnostic codes F10.1, F10.2, and F10.9.
Demographic variables included age categories and race. Military characteristics included branch of military service and military rank (Junior Enlisted, Senior Enlisted, Junior Officer, Senior Officer, Warrant Officer, Other). Family structure characteristics included marital status (single, married). In this study, single refers to unmarried and includes single, never married/divorced, and potentially some forms of separation (e.g., interlocutory divorce decree). Parental status was determined by identifying ADSW in the population with one or more dependents designated as a ‘child’ in the ADSW’s DEERS record receiving TRICARE. Number of children receiving TRICARE as a beneficiary was categorized into an ordinal variable (0, 1, or 2+). This is a surrogate method of determining parental status in the MDR, due to the nature and availability of data in the MDR.
Data analysis
Descriptive statistics were performed on demographics and military and family structure characteristics; chi-square tests were used to test for differences between the total ADSW population and those with AU and AUD. The annual prevalence of AU and AUD was calculated for each year between FY2016-2021, as well as the pre- and during COVID-19 periods; trends were analyzed by calculating the percent change in prevalence for each successive FY. To address missing AU responses, and differences in missingness in the pre- and during COVID periods, we used the reweighted estimated equations (RWEE) method to impute AU using complete observations from all patient demographics. 25 Multivariate log-binomial regressions for prevalence ratios with 95% confidence intervals were conducted to assess associations of demographics, military characteristics, and family structure characteristics with AU during the pre-COVID-19 pandemic period and the COVID-19 pandemic. Univariate and multivariate logistic regressions with 95% confidence intervals were conducted to assess associations of demographics, military characteristics, and family structure characteristics with AUD during the pre-COVID-19 pandemic period (FY2016-2019) and the COVID-19 pandemic (FY2020-2021). Statistical significance was determined with a p value < 0.05. All analyses were performed using SAS (version 9.4). This study was reviewed and considered exempt by the Institutional Review Board at the Uniformed Services University of the Health Sciences.
Results
Sample/population characteristics
We identified 281,567 ADSW during the pre-COVID-19 period and 237,327 ADSW during the COVID-19 period for inclusion in our study. Of the total ADSW identified for pre-COVID-19 period, 63% reported AU and 4.0% had AUD. The majority of the population was 18–24 years old (50.8%), White (57.5%), serving as Junior Enlisted (54.6%), and in the Army (36.9%). Of the ADSW, 59.4% were single, and 56.6% had no children, 20.7% had 1 child, and 22.7% had 2+ children. For the COVID-19 period, age, race, rank, and service branch trends remained similar. Single ADSW for this period represented 54.4% of the population, a decrease from the pre-COVID-19 period. ADSW with no children represented 63.4% of the population (an increase from the pre-COVID-19 period), while 18.2% had 1 child and 18.5% had 2+ children.
Prevalence and trends
Table 1 details the demographic distributions of AU and AUD among ADSW during the pre-COVID-19 and COVID-19 periods. Self-reported AU among ADSW was higher in the pre-COVID-19 period compared with the COVID-19 period (63.0% versus 47.9%, chi-square p < 0.001). Similarly, prevalence of AUD diagnoses was higher in the pre-COVID-19 period compared with the COVID-19 period (4.0% versus 2.7%, chi-square p < 0.001). In the pre-COVID-19 period, prevalence of AU was lowest among women without children (60.4%) and was higher among women with 1 child (64.8%) and 2+ children (68.1%). While AU was lower during the COVID-19 period, there was similar pattern of AU prevalence by parental status with women without children having the lowest prevalence (47.0%) and women with 2+ children having the highest prevalence (51.4%). Compared with prevalence of AU, prevalence of AUD diagnoses had the opposite relationship with parental status. When looking at parental status, women without children had the highest prevalence of AUD in both the pre-COVID-19 (2.6%) and COVID-19 (2.9%) periods, and women with 2+ children had the lowest prevalence of AUD in both periods (1.5% and 1.9%, respectively). When examining AU and AUD among ADSW by FY during the study period, the prevalence of AU was 50.5% in FY2016; 51.3% among those without children, and 49.0% among those with children (Fig. 1). In FY2021, the prevalence of AU was 34.9%; 35.0% among those without children, and 34.6% among those with children. When examining changes in AU from pre-COVID-19 pandemic to during COVID-19 pandemic, there was a decrease of -23.9% (−22.2% for ADSW without children,−25.4% for ADSW with children) (Supplementary Table S1). In FY2016, the overall prevalence of AUD was 1.9%; 2.1% among those without children, and 1.4% among those with children (Fig. 2). In FY2021, the prevalence of AUD was 1.8%; 2.0% among ADSW without children, and 1.4% in those with children. The change in overall prevalence of AUD from the pre-COVID-19 period to the COVID-19 period was −35.1% (−35.6% for ADSW without children, and −35.3% for ADSW with children) (Supplementary Table S3).
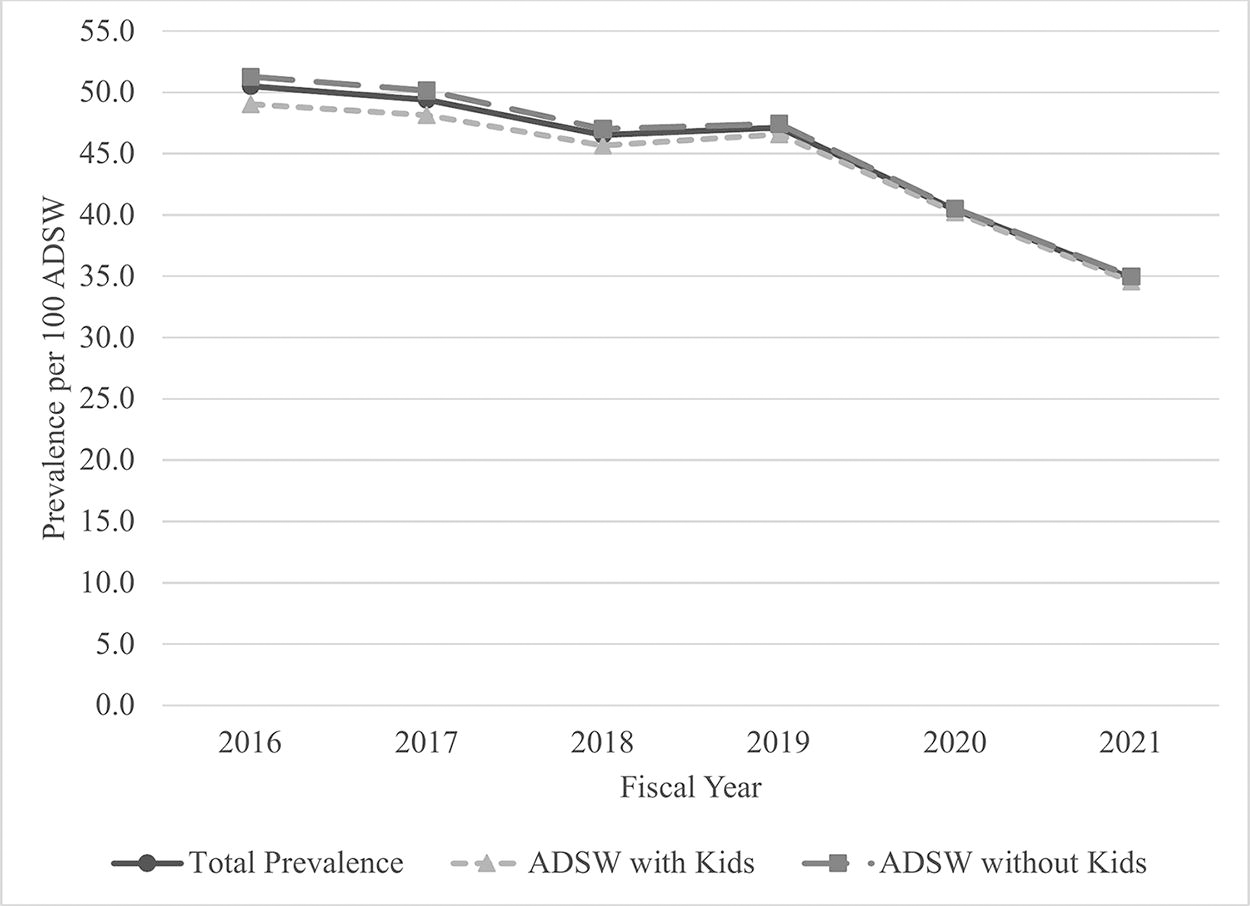
Prevalence of AU among ADSW, FY2016–2021. Total populations per year are as follows: FY2016 = 182,400; FY2017 = 184,624; FY2018 = 190,451; FY2019 = 194,826; FY2020 = 202,761; FY2021 = 207,553. Abbreviations: AU = alcohol use; ADSW = active-duty service women.

Prevalence of AUD among ADSW, FY2016–2021. Total populations per year areas follows: FY2016 = 182,400; FY2017 =184,624; FY2018 = 190,451; FY2019 = 194,826;FY2020 = 202,761; FY2021 = 207,553. Abbreviations: AUD = alcohol use disorder; ADSW = active-duty service women.
Demographics of ADSW during the Pre- and COVID-19 Period, by Self-Reported Alcohol Use and AUD Diagnosis Status
ADSW, active-duty service women; AU, alcohol use, self-reported as yes/no or the value was missing; AUD, alcohol use disorder diagnosis, defined using F10.1, F10.2, F10.9 ICD-10 diagnostic codes.
Associations of alcohol use
Figure 3 displays selected results from the comparison of adjusted prevalence ratio (aPR) results for AU during the pre-COVID-19 pandemic period to the COVID-19 pandemic period, using imputed AU information. Compared with ADSW with no dependent children, ADSW with children were less likely to report AU in both periods and this relationship became stronger during the COVID-19 period (see Fig. 3). Reporting of AU was more likely among ADSW in all age groups between 25 and 54 compared with ADSW age 21 to 24 and strengthened during the COVID-19 period (see Fig. 3). The greatest increases in the aPR for AU were observed in ADSW ages 45 to 54. ADSW of Asian/Pacific Islander race were less likely to report AU during both periods (pre-COVID-19: 0.89 aPR, 0.87–0.90 95% CI; COVID-19: 0.89 aPR, 0.87–0.91 95% CI) compared with ADSW of White race. Prior to the pandemic, ADSW of Black and ‘other’ race were less likely to report AU; however, no significant differences were observed during the COVID-19 period among ADSW of Black, American India/Alaskan Native, and “other” race. The full results for unadjusted and adjusted regression analyses with AU can be found in the Supplemental Materials (Supplementary Table S2).
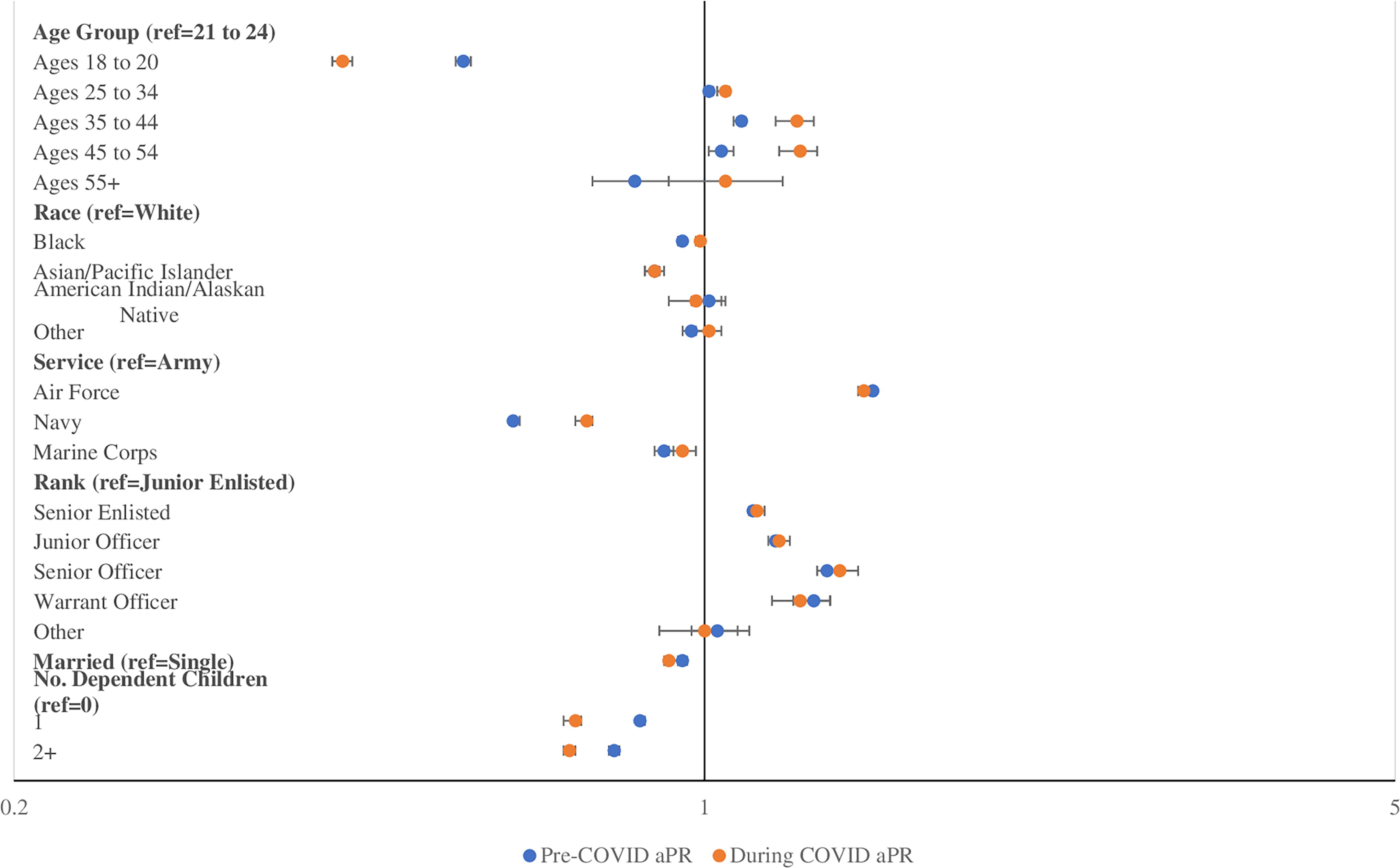
Comparison of adjusted prevalence ratios for alcohol use among ADSW, before and during the COVID-19 pandemic. X-axis is on a logarithmic scale with a base of 5. After the removal of observations with missing data, n = 272,723 for the pre-COVID-19 period and n = 230,799 during the COVID-19 period. Abbreviations: ADSW = active-duty service women; AU = alcohol use; aPR = adjusted prevalence ratio.
Associations of alcohol use disorder
Figure 4 displays selected results in the comparison of the adjusted odds in AUD diagnosis among ADSW. Compared with ADSW with no children, ADSW with children had lower odds of being diagnosed with AUD. No change was observed in the likelihood of women with one child, but the association became weaker in women with two or more children during the COVID-19 period (aORpre = 0.63, 95% CI = 0.60–0.67; aORduring = 0.68, 95% CI = 0.62–0.74). Compared with White women, Black women had higher odds of AUD in both periods and the association was stronger during the COVID-19 pandemic (aORpre = 1.04, 95% CI = 1.00–1.09; aORduring = 1.22, 95% CI = 1.15–1.29); Asian/Pacific Islander women had lower odds of AUD and the association was stronger during the COVID-19 pandemic (aORpre = 0.68, 95% CI = 0.62–0.74; aORduring = 0.65, 95% CI = 0.57–0.73); and American Indian/Alaska Native women had higher odds of AUD but the odds became weaker during the COVID-19 pandemic (aORpre = 1.73, 95% CI = 1.53–1.99; aORduring = 1.62, 95% CI = 1.34–1.95). The full results for unadjusted and adjusted logistic regression analyses can be found in the Supplemental Materials (Supplementary Table S3).
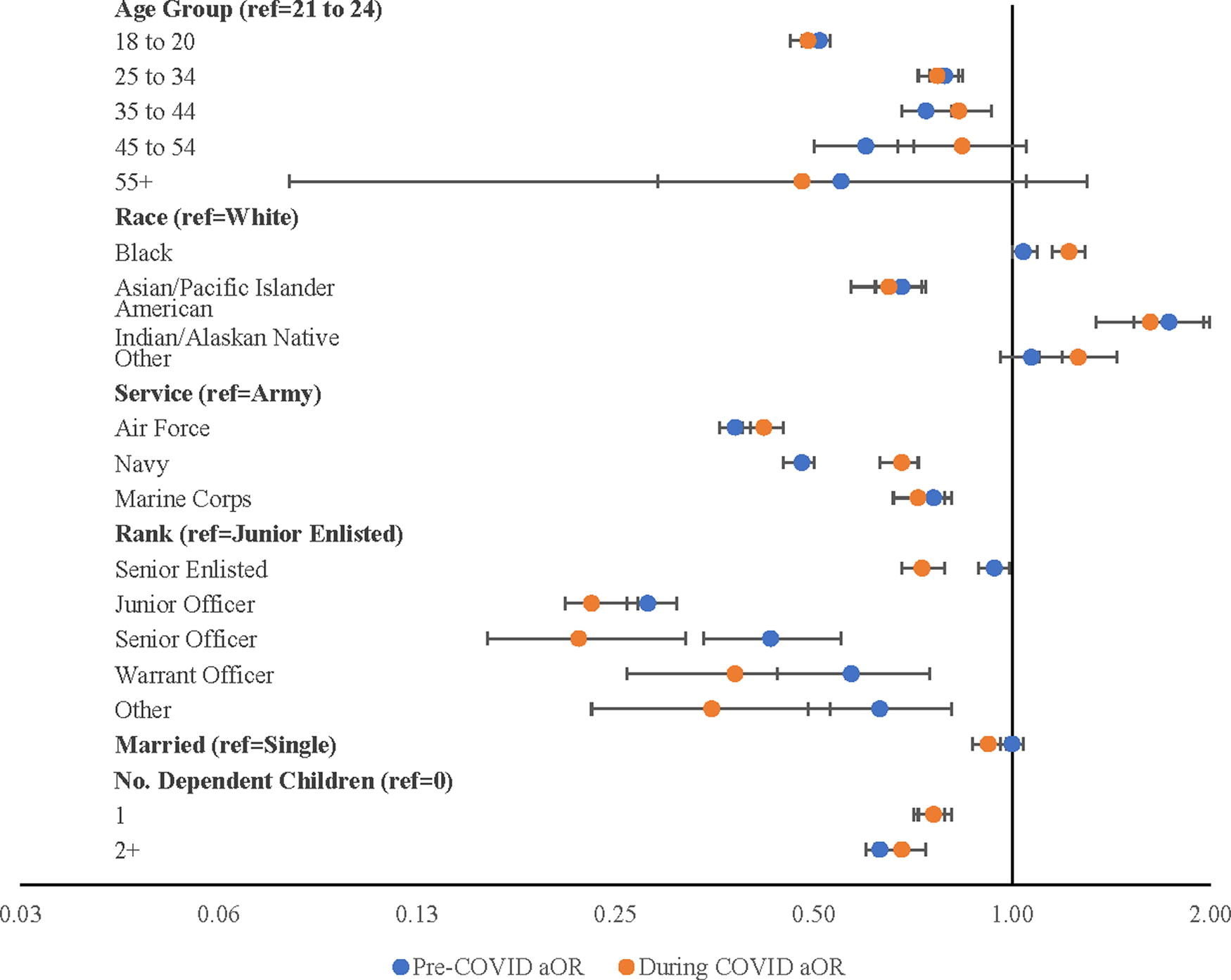
Comparison of aOR for AUD in ADSW, before and during the COVID-19 pandemic. X-axis is on a logarithmic scale. After removal of observations with missing data, n = 272,723 for the pre-COVID-19 period and n = 230,799 during the COVID-19 period. Abbreviations: AUD = alcohol use disorder; OR = odds ratio; aOR = adjusted odds ratio.
Discussion
Among this population-based study of 281,567 ADSW during the pre-COVID period and 237,327 ADSW from the COVID-19 period serving in the military between FY2016–2021, we observed significant differences in the prevalence of self-reported AU and AUD diagnoses by parental status during the pre- (FY 2016–2019) to COVID-19 periods (FY 2020–2021). Adjusted analyses revealed that ADSW with children were less likely to report AU compared with ADSW without children during the pre-COVID-19 period, and this association became stronger during COVID-19. A similar relationship was observed with AUD diagnosis. ADSW with children were less likely to have an AUD diagnosis compared with ADSW without children in both the pre- and COVID-19 periods, and the association strengthened during COVID-19.
Taken together, our results contrasted with findings from Pollard et al. and Capasso et al. that indicate increases in alcohol consumption among both women and parents during the pandemic (13,14). However, it is unclear if differences in study measures may explain these divergent findings. Our study focused on any AU assessed by a military provider during a medical encounter during the pre- and COVID-19 periods, while these other studies focused on changes in frequency and quantity of AU and self-reported changes in AU, from pre- to during the pandemic, respectively (13,14). Decreasing trends in AU and AUD among ADSW were unexpected. However, the actual prevalence of AU and AUD may not have been accurately captured due to reductions in access to care. Documentation of AU, which is self-reported during routine medical visits at military treatment facilities, and diagnosis of AUD both require interaction with the health care system and may have been impacted by an overall reduction of health care visits during the COVID-19 pandemic, which was not examined in this study. The COVID-19 pandemic caused delays and cancellations of nonemergency healthcare services, which included routine visits and nonemergency sick visits that may have led to delayed AU assessment and/or AUD diagnosis. 26 During the COVID-19 pandemic, especially in 2020, there was a shift to telehealth visits in the MHS similar to civilian settings. 27,28 Telehealth visits, including any self-report of AU or AUD diagnoses that occurred during these visits, were included in our study; however, we still observed these decreases. Future study should examine if there were differences in assessment of AU or diagnosis of AUD within telehealth visits versus in-person visits.
Specific to ADSW with children, the COVID-19 pandemic caused disruptions to schooling and childcare resources. ADSW without access to childcare may have struggled to schedule medical appointments, even if appointments were available. This lack of school and childcare has been associated with increased parental stress. 29 Experiencing stress is a known factor for heavy AU and AUD among women. 30,31 Our study findings of overall reductions in prevalence of self-reported AU and diagnoses of AUD likely capture the interruption of regular services during the COVID-19 pandemic. The finding that ADSW with children had larger percentage decreases during the COVID-19 pandemic warrants future study. Additional longitudinal studies are needed beyond 2021 to examine if these decreasing trends continue or if we observe a shift back to increasing rates of AU and AUD and to determine if there is variation by parental status. This is of particular importance as studies during the early months of the pandemic have found larger increases in alcohol use among women and parenting adults. 16,17,32
Our findings of reductions in AU and AUD among ADSW during our study time period do not correlate with the national trends of increasing AU and AUD among women, especially AU during the pandemic. 15 Using data from the National Health Interview Survey from 2006 to 2018, McKetta and Keyes found an increase in binge drinking among all age groups of women from 2006 (prevalence of 21%) to 2018 (prevalence of 42%). 5 Additional research is needed describing drinking patterns of ADSW across branches to assess for differences. The increased rates were seen both in women with and without children, but consistently lower levels of excessive drinking were reported by women with children. 5 Women who are mothers typically have reduced risk for AUD. 5,10,15 This is consistent with our study findings. Future longitudinal study is needed to examine if the gap in AU and AUD is closing between women by parental and marital status, particularly following the challenges introduced for mothers by the COVID-19 pandemic. In addition, future study is needed to examine if the emergence of “mom-wine” culture and social media groups promoting alcohol consumption among mothers may play a role in changing drinking habits among ADSW with children. 15
While not the focus of this study, we note that Black ADSW had a 22% higher odds of being diagnosed with AUD during the COVID-19 pandemic, compared to White ADSW. Past surveys of nationally representative samples have reported the highest levels of AU among White women and lower risk of AUD in Black women compared to White women.(26) However, studies suggest that differences in AU and problematic drinking among Black women compared to White women have been narrowing over the past 2 decades. 33,34 Black women face more severe health outcomes from AUD and alcohol-related diseases than White women; these disparities may be related to cultural, socioeconomic, and/or discriminatory factors. 34,35 Literature among the veteran population likewise indicates an increased prevalence of AUD among Black veterans compared to White veterans, which is suggested may be due to racial and ethnic bias by providers. 36,37 While it is possible that provider bias within the MHS is a contributing factor to the increased odds of AUD diagnosis among Black ADSW observed in our analysis, there is currently no literature on provider bias and AUD diagnosis within the active-duty population. Black women make up 4.5% of the active-duty population and 25.7% of ADSW. 38,39 More research is needed to understand why Black women in the military had elevated AUD diagnosis rates during COVID-19, to examine if these findings persist in future years, and to examine if these findings varied among Black women by parental status.
The size and inclusiveness of the study population is a substantial strength. The study population included 281,567 ADSW during the pre-COVID-19 period and 237,327 ADSW from the during COVID-19 period from all branches of service, ranks, and age groups. The military population is diverse and we were able to include information about self-reported race; however, we did not have information about self-reported ethnicity in this study. 40 The MDR provides a broad, far-reaching data pool that extends across the entire population of ADSW for the study period, limiting selection bias. Conversely, the limitations of the study are related to the use of secondary claims data and classification of outcomes and exposures. AUD was identified using diagnostic coding reported in encounter and claims data. Provider coding practices can vary and can affect prevalence estimations. AU was self-reported; subjects were verbally asked if they consume alcohol during visits at military treatment facilities, which could result in self-reporting bias. There is also a possibility that the question was not posed to each ADSW at every appointment. This variable was only available for medical visits occurring within the MHS; no data regarding AU was captured from private sector healthcare visits; however, ADSW predominantly use care at medical treatment facilities and are required to have an annual physical examination within the MHS in which AU should be assessed. Overall, 13.6% of the sample had missing AU data in the pre-COVID-19 period and 23.6% had missing AU data in the during COVID-19 period. To address missing AU data, we applied the RWEE imputation method in our regression analysis (Supplementary Table S3). In addition, we did not examine the extent to which decreasing trends in AU or AUD may have been partially explained by decreasing trends in use of any healthcare utilization during the COVID-19 period. Future study should examine if any or number of interactions with the healthcare system during the pre or COVID-19 periods are associated with AU or AUD findings. In addition, future research should extend the “during” COVID years and examine if including or excluding the last 3 months of 2019 significantly impacts study findings. There is potential for misclassification bias in ADSW with children who are married to other service members and may be incorrectly categorized as nonmothers in these analyses if the spouse claims the dependent child(ren) in DEERS.
Conclusions
National increases in AU and AUD among women have been observed since the early 2000s, causing an increased burden on the U.S. health care system. 3,34 This increased observance and risk may pose a public health concern for women. 6 Our study found unexpected trends in decreasing rates of AU and AUD among ADSW, which were likely impacted by access to care during the pandemic, with women who were mothers having larger decreases in AU during COVID-19. The trends of AU and AUD prevalence among ADSW, especially those with children, should continue to be assessed and analyzed as the healthcare sector recovers from the COVID-19 pandemic. Additional research into stressors and influences of alcohol use for military women could inform public health interventions identify target areas to enhance health and improve readiness among ADSW.
Disclaimers
The contents of this publication are the sole responsibility of the authors and do not necessarily reflect the views, assertions, opinions, or policies of the Uniformed Services University of the Health Sciences (USUHS), Boston University School of Public Health, the Henry M. Jackson Foundation for the Advancement of Military Medicine, Inc. (HJF), the Department of Defense (DoD), or the Departments of the Army, Navy, or Air Force. Mention of trade names, commercial products, or organizations does not imply endorsement by the U.S. Government. Dr. Adams reports grants from the National Institutes of Health (NIH) and Uniformed Services University (USU)/Department of Defense (DoD). She has an Intergovernmental Personnel Act agreement for work with the VHA Rocky Mountain Mental Illness Research Education and Clinical Center. All other authors report no conflicts of interest or financial conflicts.
Footnotes
Authors’ Contributions
All authors have contributed equally.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This work was conducted with the Center for Health Services Research and funded by the Department of Defense, Defense Health Agency, grant #HU0001-21-2-0089. The funding agency played no role in the design, analysis, or interpretation of findings.
Supplementary Material
Supplementary Table S1
Supplementary Table S2
Supplementary Table S3
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.