
Abstract
Background:
Black birthing people have significantly higher risks of maternal mortality and morbidity compared with White people. Preconception chronic conditions increase the risk of adverse pregnancy outcomes, yet little is known about disparities in preconception health. This study applies an intersectional framework to examine the simultaneous contributions of racial marginalization and economic deprivation in determining disparities in preconception risk factors and access to care.
Methods:
Using data from the Pregnancy Risk Assessment Monitoring System, 2016–2020 (N = 123,697), we evaluated disparities by race and income in self-reported preconception hypertension, diabetes, obesity, depression, and smoking, as well as preconception insurance coverage and utilization of health care. We estimated linear regression models and calculated predicted probabilities.
Results:
Black respondents experienced higher probabilities of preconception obesity and high blood pressure at every income level compared with White respondents. Higher income did not attenuate the probability of obesity for Black respondents (linear trend p = 0.21), as it did for White respondents (p < 0.001). Conversely, while White respondents with low income were at higher risk of preconception depression and smoking than their Black counterparts, higher income was strongly associated with reduced risk, with significantly steeper reductions for White compared with Black respondents (difference in trends p < 0.001 for both risk factors). White respondents had higher probabilities of utilizing preconception care across all income levels, despite similar probabilities of insurance coverage.
Conclusions:
Higher income does not protect against the risk of preconception obesity and other preconception risk factors for Black birthing people as it does for White birthing people. Results point to the need to consider multiple forms of intersecting structural factors in policy and intervention research to improve preconception and maternal health.
Introduction
In the United States, there are staggeringly large and persistent racial inequities in maternal mortality and morbidity. 1,2 The risk of maternal mortality is 3.5 times higher for non-Hispanic Black birthing people compared with non-Hispanic White people, and risks of preeclampsia, eclampsia, and cardiomyopathy are 5 times higher. 3 Among the leading medical causes of maternal mortality are cardiovascular disease and hypertensive disorders. 3,4 From a life course perspective, improving health in the period before pregnancy to address preexisting chronic conditions has been increasingly recognized as playing a significant role in preventing maternal deaths and reducing racial disparities, 5 particularly as Black women are disproportionately burdened by chronic health conditions such as cardiovascular disease, hypertension, and obesity. 6,7 Pregnant people who have two or more chronic conditions have a nearly two times higher risk of maternal intensive care admission and four times higher risk of severe maternal morbidity compared with those without these conditions. 8,9
Structural racism is a key driver of racial and ethnic health inequities in maternal health. 10 –13 Defined as the totality of ways by which social and political institutions work in interlocking and mutually reinforcing ways to disenfranchise racially and ethnically marginalized populations, 12,14 structural racism adversely affects health through restriction of socioeconomic opportunity, exposure to environmental and psychosocial stress, and discrimination and bias in health care. 15,16 A prominent pathway through which structural racism negatively impacts health is via economic deprivation, with Black women greatly overrepresented among those living in poverty and working low-wage jobs. 6,17 –19 Conditions of socioeconomic disadvantage, such as inability to afford housing, nutritious food, and health care, are strongly predictive of preconception and maternal health. 6,20,21 Yet, racial disparities in maternal health are even more pronounced among Black and White birthing individuals with high income and education. 1
A key explanation for this is the role of stress and trauma owing to negative life events, experiences of interpersonal racism, and living in segregated neighborhoods, which adversely affect health across the life course, in particular by increasing risk of hypertension and cardiovascular disease. 10,22 –26 Structural racism shapes the distribution of these stressors, which are more likely to be experienced by Black versus White people independent of socioeconomic position, as well as the resources needed to cope with stress. 10,25 For example, a recent study found that hypertension associated with racial discrimination disproportionately affected Black women with the highest education compared with Black women with lower education. 27
The complexity of these structural influences on maternal morbidity underscores the need for research that examines the impact of multiple dimensions of structural marginalization on preconception health and care. Intersectionality is a framework that allows us to consider the interlocking and compounding effects of structural determinants like racism and economic deprivation simultaneously, providing insight on how these systems combine to shape preconception health disparities. 14,28 –30 Ultimately, this framework can be used to identify those most at risk of poor outcomes and guide the development of policies and programs to advance health equity. Although some studies have examined racial disparities in preconception health, 31 –33 and previous work has explored racial and socioeconomic disparities in preconception obesity, 32 more research is needed on a broader set of preconception risk factors and how they intersect with race and socioeconomic status.
In this study, we apply an intersectional framework to examine the simultaneous contributions of race and reported income to disparities in preconception health and health care. Race is a social construct. We consider differences by race to be attributed to root causes such as racial marginalization, not to race itself. 12 Using population-based data from 48 states, we evaluated disparities in 5 preconception risk factors—diabetes, high blood pressure, obesity, smoking, and depression—which are highly associated with maternal morbidity and adverse birth outcomes. 33 We also examined disparities in health care access and utilization in the preconception period.
Materials and Methods
We used data from sites participating in the CDC's (Centers for Disease Control and Prevention) Pregnancy Risk Assessment Monitoring System (PRAMS) between 2016 and 2020 (n = 47 sites including 45 states, District of Columbia, and New York City). 34 Participating sites use birth certificate records to select a representative sample of individuals who delivered a live-born infant in their jurisdiction. Individuals are contacted by mail to complete a survey and are followed-up by phone if there is no initial response. The weighted data are representative of each site's annual birth population. When aggregated, PRAMS data represent 83% of all U.S. births. 34 PRAMS does not collect data on the gender identity of participants. Recognizing that not all people who give birth are women, we use gender-neutral terms when referring to our own findings.
Race and ethnicity were obtained from the birth certificate. We included participants who identified as non-Hispanic Black or non-Hispanic White (hereafter referred to as Black or White participants, n = 134,634). We focus on Black and White participants because of the substantial disparities in maternal mortality for these groups and sample sizes are large enough to disaggregate by both race and income. We show results for other racial and ethnic groups in the Supplementary Data. We excluded participants who were missing data on income or household size (8.1%). The final sample size was 123,697. Supplementary Appendix Table SA1 shows sample sizes for all sites and years. We used complete case analysis for our main results; in sensitivity analysis we compared results with multiple imputation. The data were deidentified and this study was deemed exempt from review by Rutgers University Institutional Review Board.
Income was self-reported as total household income in the 12 months prior to pregnancy, collected in categorical brackets. Following previous work using income data in PRAMS, continuous income was inferred as the highest value on the corresponding income bracket. 35 We merged PRAMS with data on federal poverty limits (FPL) by household size for each year for the contiguous states, Alaska, and Hawaii, from the historical poverty guidelines obtained from the U.S. Department of Health and Human Services, and categorized household income as ≤100%FPL, 101%–200%FPL, 201%–400%FPL, and >400%FPL. 36
We examined five binary preconception risk factors: smoking, obesity, high blood pressure or hypertension (hereafter high blood pressure), type 1 or type 2 diabetes (hereafter diabetes), and depression. These modifiable risk factors are strongly associated with pregnancy-related outcomes, including preterm birth, stillbirth, gestational diabetes, obstetric complications, and maternal death, 23,33,37 –39 and have implications for long-term health of both the childbearing individual and infant. 40,41
Smoking was ascertained by a survey question that asks how many cigarettes the participant smoked on average per day in the last 3 months before pregnancy; this was coded as a binary variable for any number of cigarettes >0.
Obesity, defined as body mass index (BMI) ≥30, was obtained from a calculation of self-reported height and weight before pregnancy. BMI is a flawed measure of health, particularly among Black populations, in which cutoffs for obesity are less accurate than for White populations. 42 –44 Nevertheless, a large literature finds that at the population level, obesity among Black birthing individuals is significantly associated with a range of pregnancy-related conditions including hypertensive disorders, gestational diabetes, stillbirth, and preterm birth. 45 –48 In addition, BMI is a widely used risk factor for guiding clinical decision making during pregnancy and thus shapes pregnancy experiences for birthing people with obesity. 46 Therefore, we include this measure in our analysis, and return to the limitations of its use in the discussion.
For the risk factors of diabetes, high blood pressure, and depression, the survey question asked the respondent to self-report whether they had those health conditions in the 3 months before pregnancy. Finally, we calculated the total number of risk factors out of 5, as risk factors may interact synergistically. 33
We also examined two binary preconception measures of access to and use of preconception health care. Insurance coverage was measured via self-reported insurance status in the month before pregnancy. Use of preconception care was assessed via a survey question that asked if the respondent had any health care visits in the 12 months before pregnancy.
We considered maternal age, education, marital status, and parity, alongside state and year of delivery, as covariates. We selected these covariates based on their identification in the literature as known demographic predictors of preconception health. 30,33
First, we estimated separate linear regression models of each risk factor on an interaction between income and race, minimally adjusting for maternal age, state, and year. We used the results from the models to calculate predicted probabilities and 95% confidence intervals (CIs) of preconception risk factors by race and income, averaging over covariates. We then added further covariates into our models, including education, marital status, and parity, recognizing that some of these variables may mediate the relationships between race, income, and outcomes, producing conservative estimates. 49,50 This sequential approach to adjustment for covariates allowed us to assess disparities with and without covariates. 51 As results did not substantially differ, our main estimates shown are minimally adjusted, with fully adjusted estimates provided in the Supplementary Data.
Regressions were weighted by the PRAMS survey weights for each state-year to account for sampling design and standard errors were clustered at the state level. 52 We tested for a socioeconomic linear trend by including FPL level in the regression linearly and tested for a difference in slopes for Black versus White respondents using a chi-squared test. Analyses were conducted in Stata v18.
Results
Table 1 provides weighted descriptive characteristics of non-Hispanic Black and non-Hispanic White respondents in the sample. Black respondents were significantly more socioeconomically disadvantaged than White respondents: they were less likely to be married (Black 30.7% vs. White 73.4%), and to have a college degree (Black 20.0% vs. White 47.2%). While 34.7% of Black respondents had income below 100%FPL and 36.8% had income between 101% and 200%FPL, for White respondents these percentages were 13.6% and 20.3%, respectively. On average, compared with White respondents, Black respondents had 1.1-fold higher risk of preconception diabetes, 1.9-fold higher risk of high blood pressure, and 1.6-fold higher risk of obesity. Conversely, compared with Black respondents, White respondents had 1.3-fold higher risk each of depression and smoking.
Socioeconomic Characteristics, Preconception Risk Factors, and Preconception Access and Utilization of Care Among Study Sample, by Race
Percentages are weighted by PRAMS survey weights.
FPL, federal poverty limit; PRAMS, Pregnancy Risk Assessment Monitoring System; SD, standard deviation.
Figure 1 shows predicted probabilities of preconception risk factors by race and income level from the minimally adjusted models. The predicted probability values were multiplied by 100 to be reported as percentages. Regression coefficients are given in Supplementary Appendix Table SA2. Tests of significance for linear trends are given in Supplementary Appendix Table SA3. Black respondents experienced higher probabilities of preconception obesity compared with White respondents across all income levels and there was a significant difference in the socioeconomic linear trends by race (p < 0.001). For Black respondents, the predicted probability of obesity was 38.9% (95% CI, 37.1–40.6) in the lowest income group and 35.8% (95% CI, 33.3–38.3) in the highest income group (linear trend p = 0.21), whereas for White respondents the probability decreased over these income groups from 32.0% (95% CI, 30.7–33.2) to 17.2% (95% CI, 16.4–18.0) (trend p < 0.001).
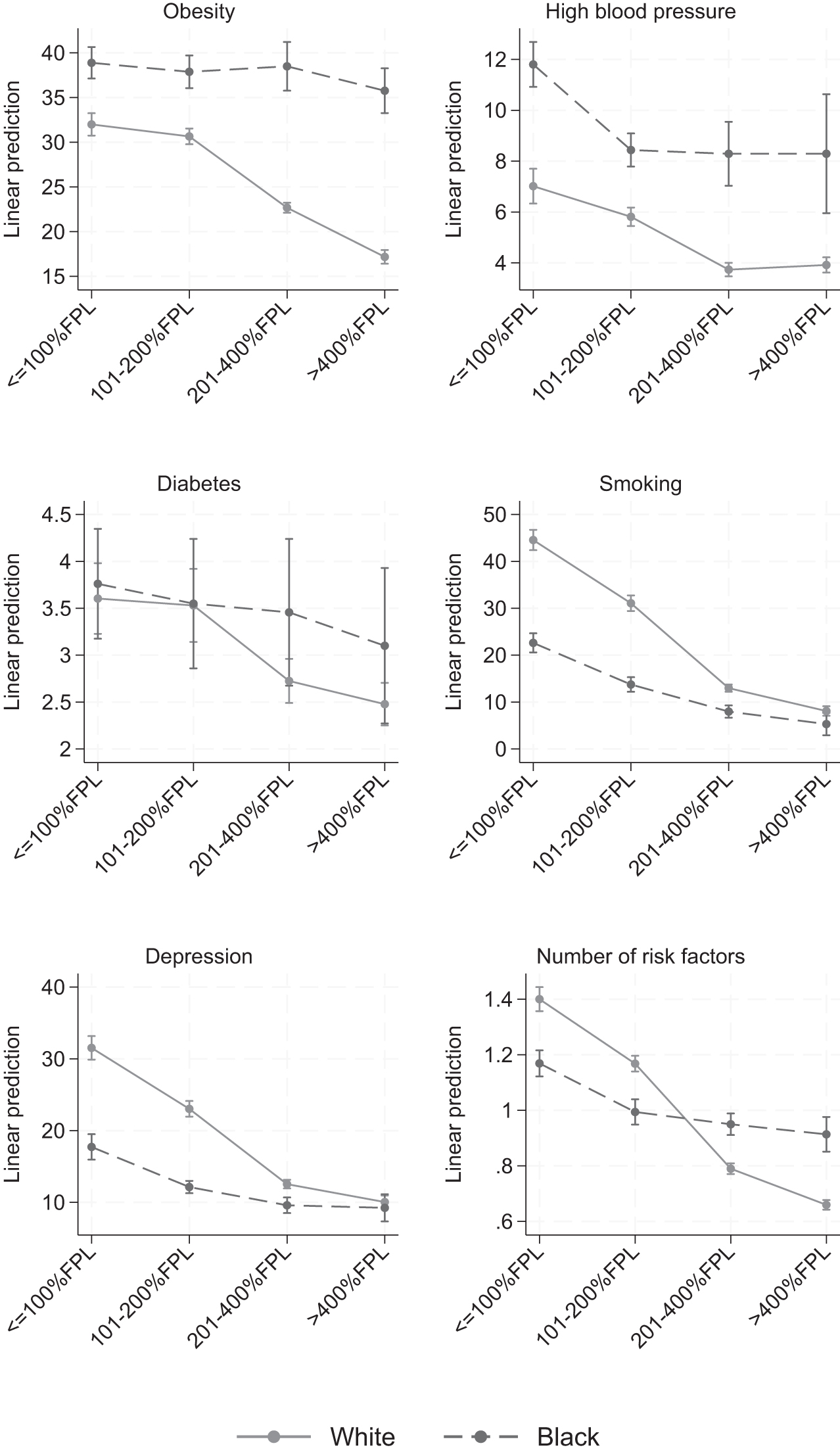
Predicted probabilities of preconception risk factors by race and income level. Predicted probabilities are weighted to account for sample design. The predicted probability values are multiplied by 100 to be reported as percentages. Data are adjusted for age, state, and year. FPL, federal poverty limit.
Similarly, at every income level, Black respondents experienced higher probabilities of high blood pressure compared with White respondents. However, the difference in trends was not statistically significant (p = 0.34). Probability of diabetes was similar for Black and White respondents in the bottom two income groups. For the top two income groups, probability of diabetes stayed relatively unchanged for Black respondents (i.e., the socioeconomic trend was flat), whereas it decreased for White respondents, although the difference in trends was not significant (p = 0.17).
Conversely, compared with Black respondents, White respondents experienced higher probabilities of preconception smoking and depression than Black respondents at lower income levels, but similar probabilities at higher income levels. For both risk factors, the socioeconomic downward trends were significantly steeper for White respondents (p < 0.001). From lowest to highest income group, probability of preconception smoking reduced from 44.6% (95% CI, 42.4–46.7) to 8.1% (95% CI, 7.1–9.1) for White, and from 22.6% (95% CI, 20.6–24.7) to 5.3% (95% CI, 2.9–7.7) for Black respondents. Probability of preconception depression reduced from 31.5% (95% CI, 29.9–33.2) to 10.1 (95% CI, 9.1–11.0) among White and 17.7% (95% CI, 16.0–219.5) to 9.2% (95% CI, 7.3–11.1) among Black respondents.
The mean total number of risk factors was higher for White compared with Black respondents for those in the bottom two income groups, but this pattern was reversed for those in the top two income groups. This was because the linear downward trend was more pronounced for White than for Black respondents (difference in trend p < 0.001).
Figure 2 presents predicted probabilities of preconception insurance coverage and utilization of preconception care by income and race. Both variables show strong positive relationships with income for both White and Black respondents. Probability of insurance coverage was similar between White and Black respondents, with Black respondents having slightly higher probability of insurance coverage at the lowest income level (86.8% Black vs. 82.3% White). Compared with Black respondents, White respondents had higher probabilities of utilizing preconception care across the top three income groups, although differences were largest for the middle two income groups.
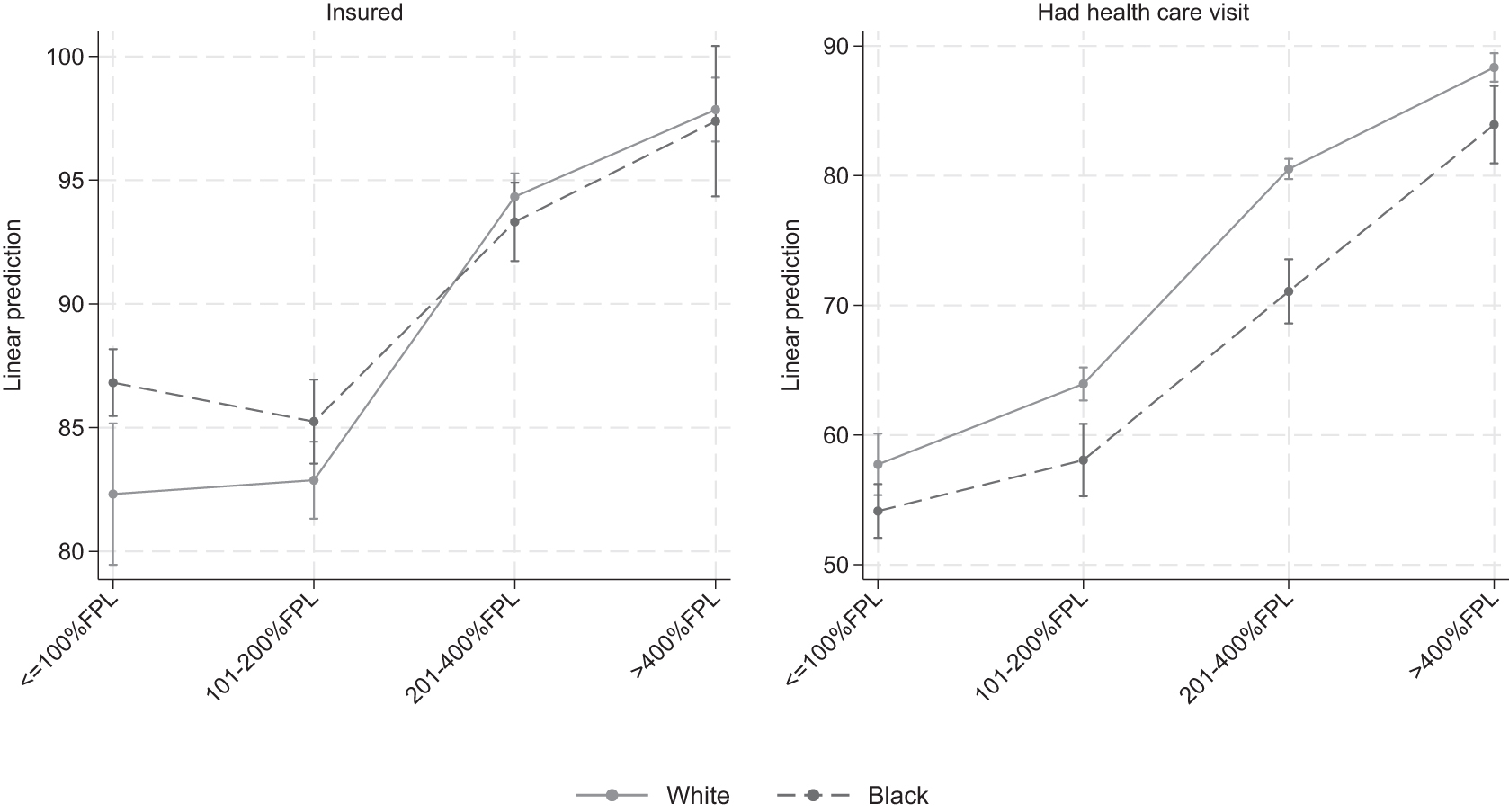
Predicted probabilities of preconception insurance coverage and utilization of preconception health care by race and income level. Predicted probabilities are weighted to account for sample design. The predicted probability values are multiplied by 100 to be reported as percentages. Data are adjusted for age, state, and year.
In sensitivity analysis, results from multiple imputations were found to be nearly identical as complete case analysis (Supplementary Appendix Table SA2). Fully adjusted models were also very similar to the minimally adjusted models (Supplementary Appendix Table SA4). Figures showing predicted probabilities of risk factors and access to care variables for all race and ethnicity categories are given in Supplementary Appendix Figures SA1 and SA2.
Discussion
This study documented significant disparities in preconception risk factors at the intersection of racial marginalization and economic deprivation. Comparing Black with White birthing people overall, Black individuals were more likely to experience preconception diabetes, high blood pressure, and obesity, whereas White individuals were more likely to experience preconception smoking and depression. However, these overall risks masked important socioeconomic trends. Of note, higher levels of income did not attenuate the risk of obesity among Black birthing people the way that it did for their White counterparts. Similarly, although higher income was associated with reductions in probability of preconception depression and smoking for everyone, the reductions were substantially steeper for White compared with Black people. Our results are consistent with a body of evidence, which finds that higher socioeconomic status does not produce the same health gains for Black individuals as it does for White individuals. 30,53 –55
Our work also contributes to the growing literature linking structural racism to inequities in maternal outcomes. 10,12 Racist policies, practices, and norms across mutually reinforcing societal and institutional domains perpetuate health inequities through a variety of mechanisms. One such mechanism is exposure to economic deprivation; however, our results provide evidence that other mechanisms unrelated to socioeconomic status, for example, residential segregation, racial bias in health care, and stress because of perceived discrimination and negative life events, may play a significant role in explaining preconception health disparities. 10,15,55,56
This study also documented disparities in preconception health care access (health insurance coverage in the month before pregnancy) and utilization (health care visit in the year before pregnancy). For both variables, there was a strong positive relationship with income for both White and Black birthing people, suggesting that economic resources are key drivers of access to preconception care. However, despite similar levels of insurance coverage, Black individuals had lower probability of utilization of care, particularly in the middle-income groups. This is consistent with recent work, which finds that racial disparities in utilization of services is not merely predicated on health insurance. 57 For example, when Black women experience racism, discrimination, or other poor quality treatment in health services, they consciously choose to stay away from those services in the future. 58
Implications for Research and Policy
Our study has implications for health and social policy. Improving preconception health is critical to reducing racial disparities in maternal mortality and morbidity. 5,59 Preeclampsia, eclampsia, and cardiomyopathy are leading causes of maternal death for non-Hispanic Black birthing people, with rates up to five times higher for Black compared with White individuals. 3 Preconception care supports continuity of health care across the life course, which is essential to address the rising rates of chronic disease among birthing people. 59 Systematic reviews have found that some preconception interventions are effective at improving pregnancy outcomes 60,61 ; however, more research on the effectiveness of preconception interventions and policies is needed.
Specifically, our research points to the importance of evaluating complex structural determinants across the life course. First, research is needed to investigate the impact of policies to address economic disadvantage among Black women and low-income birthing people, such as increasing minimum wages; expanding paid leave, Medicaid coverage, and social services; and implementing other poverty-alleviation programs, on preconception health indicators. 17,62,63
Second, greater understanding is needed on the role of mechanisms of structural racism such as residential segregation, chronic stress, and health care discrimination, on health care utilization and outcomes in the preconception period. Finally, research using an intersectional approach is needed to understand the interactive and cumulative effects of multiple exposures across multiple systems of oppression simultaneously and across different life stages, including early childhood, adolescence, and preconception adulthood. 64 Such research would provide insight on the synergistic effects of multiple dimensions of structural determinants on preconception and maternal health and point to appropriate policies to address them.
This study has some limitations. Income was reported categorically. This may result in measurement error in the exposure variable, which, if random, would bias our results toward the null. 65 In addition, household income does not capture total wealth, such as assets, and does not encompass broader structural determinants such as neighborhood economic conditions. There were some missing data; however, we compared complete case analysis with multiple imputation and found very similar results. Although our data include 47 U.S. states and sites across 5 years, there is some limitation in generalizability as the data, while population level, are not nationally representative.
Furthermore, all risk factors were self-reported and may be subject to reporting bias owing to stigma or lack of access to health services where a respondent could obtain a diagnosis. For example, studies have found that Black women underreport depressive symptoms and are less likely to seek care. 66 Finally, obesity as measured by BMI is an imperfect measure of maternal health, particularly for Black people. 42,43 Moreover, a focus on obesity in pregnancy can lead to weight bias, stigma, and discrimination in health care, as well as increased risk of postpartum depression for affected individuals. 67,68 Better measures of adiposity, including waist circumference, body fat percentage, or other tools would improve our analysis; however, we are limited to what is collected in the PRAMS data. Further research examining racial disparities in preconception adiposity using better measures is needed.
Conclusions
In this study, we found significant racial and socioeconomic disparities in preconception risk factors among Black and White birthing people, including diabetes, hypertension, obesity, smoking, and depression. Of importance, higher socioeconomic status, as measured by income, did not reduce the probability of many of these risk factors for Black women, whereas socioeconomic reductions were pronounced for White women. There has been increasing focus on the role that health before pregnancy and across the life course plays in maternal health outcomes. Our results underscore the importance of addressing multiple forms of intersecting structural disadvantage, including structural racism and economic inequity, to improve preconception and maternal health. 69
Footnotes
Authors' Contributions
S.R.: Conceptualization, analysis, writing—original draft, writing—review and editing; visualization; M.M.: writing—review and editing.
Data Availability
PRAMS data are publicly available for researchers by submitting a proposal to the CDC.
Author Disclosure Statement
No competing financial interests exist.
Acknowledgment
We thank the PRAMS Working Group, which includes the PRAMS Team, Division of Reproductive Health, CDC and the 47 included PRAMS sites for their role in conducting PRAMS surveillance and allowing the use of their data. We also thank Devin English and Mark McGovern at the Rutgers School of Public Health, as well as an anonymous reviewer for their useful feedback.
Funding Information
This work was supported by Eunice Kennedy Shriver National Institute of Child Health and Human Development (NICHD; Grant No. 1R01HD110482-01).
Supplementary Material
Supplementary Data
Supplementary Appendix Table SA1
Supplementary Appendix Table SA2
Supplementary Appendix Table SA3
Supplementary Appendix Table SA4
Supplementary Appendix Figure SA1
Supplementary Appendix Figure SA2
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.